
Abstract
A middle-aged man presented to the emergency department after a seemingly trivial head injury. Recognition of pathognomonic radiological findings allowed early diagnosis of a potentially life-threatening condition. The patient recovered uneventfully after prompt neurosurgical intervention.
Case presentation
A middle-aged man lost balance and hit his head against a wall while playing basketball. He presented with lightly blood-stained clear nasal discharge, mainly from the left nostril. There had been no loss of consciousness, headache, dizziness, nor vomiting. He was afebrile, fully conscious with blood pressure 146/83 mmHg, heart rate 89/min, respiratory rate 16/min and SpO2 100% on room air. Examination showed tenderness and swelling over his left face with abrasion and bruises over the infraorbital area. There was no nasal swelling, deformity or septal haematoma. No focal neurological deficit was identified. Computed tomography (CT) scans with brain and bone window were performed (Figure 1).
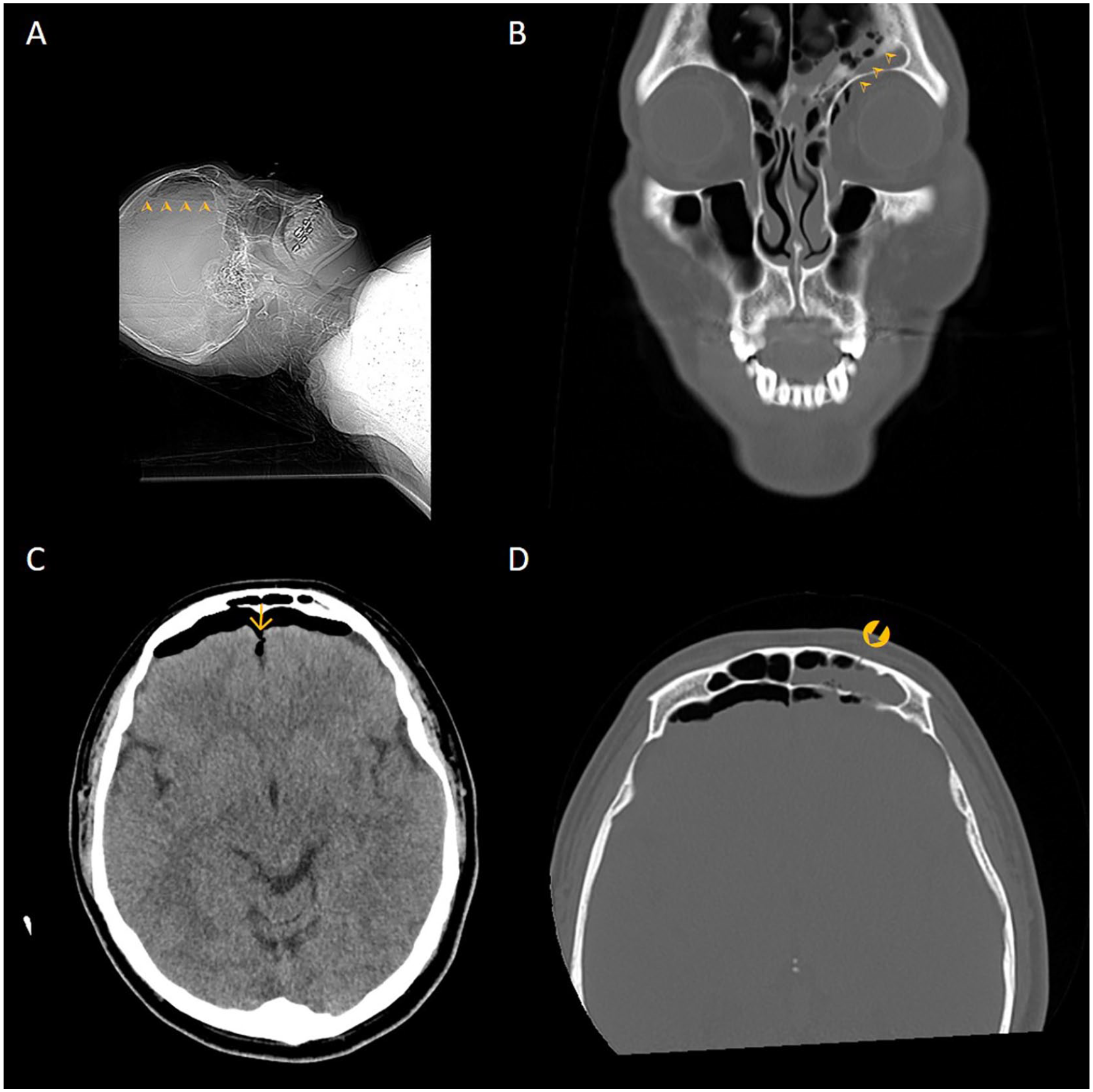
Computed tomography scans with brain and bone window of the patient.
Questions
Describe the CT findings.
What is his most worrisome diagnosis?
How should he be managed at the emergency department?
Answers
Pneumocephalus ( ) is apparent on the scout film (A) and coronal scan (B). Bifrontal subdural air with crescentic contour is seen, with pressure effect on the frontal lobes (C). The interhemispheric fissure (
) is apparent on the scout film (A) and coronal scan (B). Bifrontal subdural air with crescentic contour is seen, with pressure effect on the frontal lobes (C). The interhemispheric fissure ( ) is widened and the frontal lobes are separated. Intracranial haemorrhage is absent. The basal cisterns are not obliterated. Fracture of the left frontal sinus (
) is widened and the frontal lobes are separated. Intracranial haemorrhage is absent. The basal cisterns are not obliterated. Fracture of the left frontal sinus ( ) with fluid collection with attenuation in the range of 10–50 Hounsfield units is shown in bone window (D).
) with fluid collection with attenuation in the range of 10–50 Hounsfield units is shown in bone window (D).
Mount Fuji sign on CT should alert the clinician to the diagnosis of tension pneumocephalus.
Patients with tension pneumocephalus should be laid supine with the head of bed elevated to reduce venous backpressure. Valsalva manoeuvres (such as nose-blowing, coughing or sneezing) should be avoided to prevent air in the sinuses from entering the intracranial cavity. High flow of oxygen should be delivered to facilitate de-nitrogenization and air resorption. Prophylactic IV antibiotics and anticonvulsants can be considered. Urgent neurosurgical consultation should be sought and frequent neurological assessment should be performed.
Discussion
Pneumocephalus is the presence of air in the epidural, subdural, or subarachnoid space, within the brain parenchyma or ventricular cavities. The most common aetiology is traumatic (fracture skull base, temporal bone or paranasal sinuses and penetrating injuries) and postoperative, while other causes include neoplastic, infectious, barotraumatic or even, rarely, spontaneous. 1
Tension pneumocephalus is an uncommon but serious complication in which continuous accumulation of air exerts mass effect on the brain resulting in neurological compromise. Two mechanisms of pathophysiology have been postulated. The ‘ball-valve’ theory of Dandy suggests air trapping as a result of unidirectional flow of air through a defect; while the ‘inverted-soda bottle-effect’of Horowitz and Lunsford proposes that air is drawn in by the negative pressure generated by excessive loss of cerebrospinal fluid (CSF). 2
Tension pneumocephalus can develop acutely or chronically (⩾72 h). Clinical presentation can be numerous, ranging from headache, hemiparalysis, to obtundation. 2 Rapid deterioration in mental status should alert the clinician to this condition but diagnosis may be expedited by recognition of characteristic CT findings.
CT is a sensitive imaging tool that can detect as little as 0.55 mL of intracranial air. 1 Radiological signs of tension pneumocephalus include peaking sign, Mount Fuji sign, and air bubble sign. 3 In the peaking sign, the two frontal lobes are pushed towards the midline to form a peak surrounded by air. The ominous Mount Fuji sign heralds the point at which intracranial air pressure exceeds surface tension of CSF between the frontal lobes, separating them into two ‘peaks’. The air bubble sign shows multiple small air bubbles scattered across subarachnoid cisterns due to a tear in the arachnoid membrane. The air bubble sign can also be present in pneumocephalus without elevated intracranial pressure. 4
Tension pneumocephalus is a neurosurgical emergency that warrants immediate management. The objectives are to relieve pressure, repair skull base defect, and reduce risk of post-traumatic infection. Prognosis is generally good with timely intervention. 2 Neurosurgical interventions include needle aspiration, cranial burr hole, craniotomy, and ventriculostomy to relieve intracranial pressure and definitive closure of the dural defect. 5
Our patient underwent emergency burr hole and ventriculostomy with external drainage 7 hours from diagnosis. The CSF rhinorrhoea resolved on day 6 of admission. The external ventricular drain was removed on day 8 of admission and the patient was discharged the next day.
Conclusion
Tension pneumocephalus is a rare but potentially devastating condition that warrants immediate management.
Clinical signs and symptoms may be nonspecific but CT imaging can help clinch the diagnosis.
The peaking sign, the Mount Fuji sign and air bubble sign are characteristic radiological findings.
At an impressive height of 3776.24 m, we hope the peak of Mount Fuji will remind readers of this formidable diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was not necessary because no patient data has been included in the manuscript.