
Abstract
A 37-year-old HIV-positive woman presented to the emergency department with fever, headache, confusion, and seizures for 3 days. Computed tomography of the head with contrast demonstrated multiple ring-enhancing masses. An eccentric mural nodule in ring-enhanced mass characterizes eccentric target sign, which is pathognomonic for cerebral toxoplasmosis. The patient received anti-toxoplasmic therapy and had marked clinical improvement.
Case history
A 37-year-old woman with a history of acquired immune deficiency syndrome (AIDS) presented to our emergency department with headache, fever, and confusion for 3 days. There was no focal neurologic deficit, but seizure was present. Computed tomography (CT) of the head with contrast (Figure 1(a)) was done.
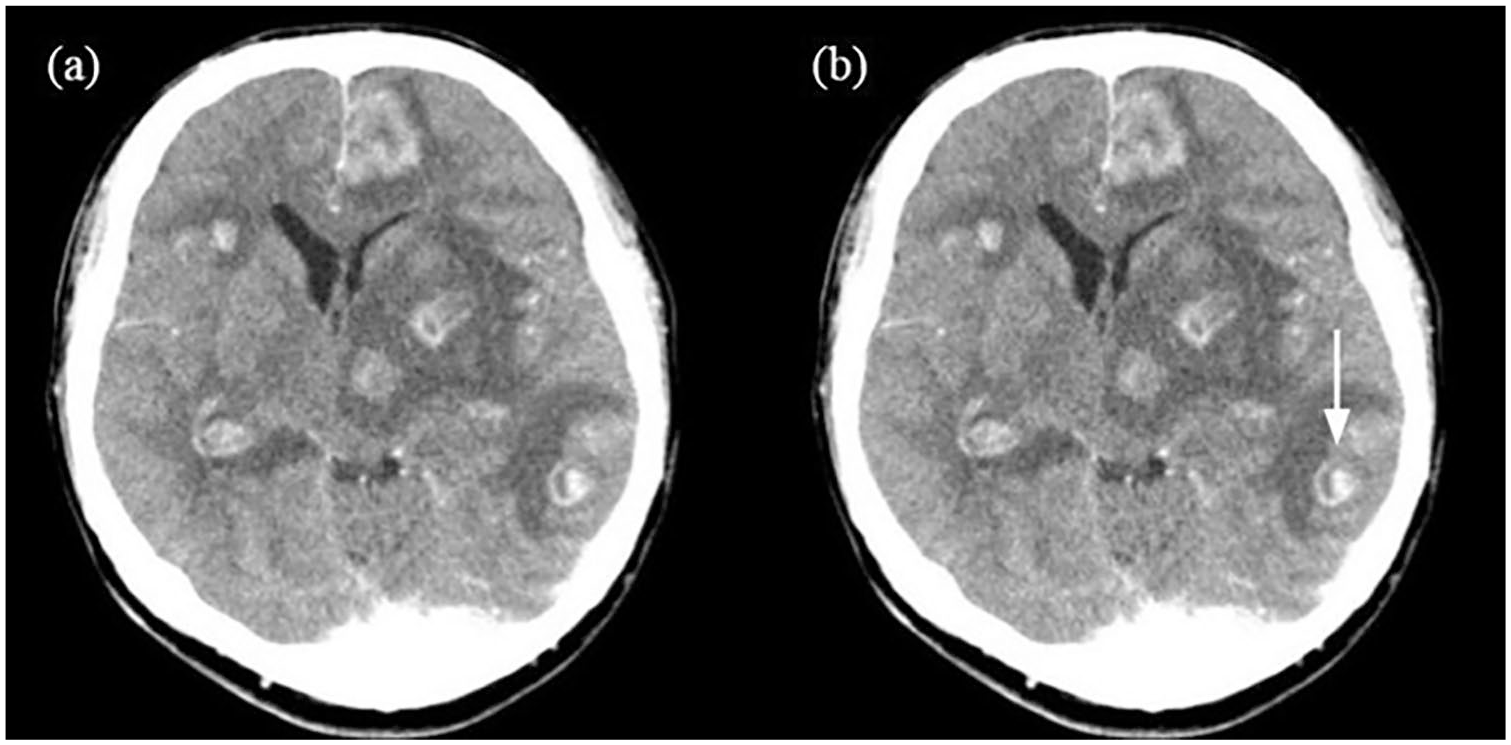
Computed tomography (CT) of the head with contrast revealed eccentric target sign: (a) without arrow and (b) with arrow.
Questions
What is the sign revealed in the CT scan?
What does the sign indicate?
Answers
Eccentric target sign (Figure 1(b)).
Cerebral toxoplasmosis.
The CT of the head with contrast demonstrated multiple ring-enhancing masses with perifocal edema at bilateral cerebrum, left basal ganglia, thalamus, and midbrain, causing significant mass effect. An eccentric mural nodule in ring-enhancing mass characterizes eccentric target sign (Figure 1(b) arrow). CD4+ lymphocyte count was 125/μL (reference range: 404–1612/μL). Serum toxoplasma IgM and IgG were positive. She received anti-toxoplasmic therapy and had marked clinical improvement. Magnetic resonance imaging (MRI) of the head with contrast 2 months later disclosed significant regression of previous ring-enhancing nodules, perifocal edema, and mass effect.
Cerebral toxoplasmosis is the most common opportunistic infection of the central nervous system caused by Toxoplasma gondii and occurred more frequently in patients with AIDS. The symptoms may include fever, headache, confusion, seizure, or focal neurologic deficits. 1 A presumptive diagnosis relies on clinical syndromes, serology, typical radiographic appearance, and clinical response to anti-toxoplasmic therapy. The definite diagnosis of cerebral toxoplasmosis requires a brain biopsy. A decision to start anti-toxoplasmic therapy is often empiric. 2 Typical radiographic manifestations of head CT with enhancement disclose multiple ring-enhancing brain lesions predominantly in the basal ganglia and corticomedullary junction. 3 The eccentric target sign is pathognomonic for cerebral toxoplasmosis, but can be seen in less than one-third of patients.4,5 Standard treatment consists of pyrimethamine, sulfadiazine, and folinic acid.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study procedures were in accordance with ethical standards.
Availability of data and materials
Data sharing is not applicable to this article as no data sets were generated or analyzed during this study.
Informed consent
Written informed consent was not necessary for the anonymized information in the manuscript.
Human rights statement
There is no violation of human rights.