
Abstract
Background:
Minor head trauma is frequently presented to the pediatric emergency department. Despite the burden this injury poses on public health, evidence-based clinical guidelines on the assessment and management of pediatric minor head trauma remain unestablished, particularly in children below 2 years. We aimed to assess the diagnostic accuracy of a clinical decision rule (Pediatric Emergency Care Applied Research Network rule) and physician discretion in the recognition of practically important traumatic brain injury in children below 2 years of age presenting with minor head trauma to the emergency department.
Methods:
The medical records of children younger than 2 years presenting with head trauma to the emergency department were reviewed with Glasgow Coma Scale scores of 14–15. Practically important traumatic brain injury is a clinically essential traumatic brain injury including all cranial abnormalities (e.g. skull fracture) detected by computed tomography. All predictor variables of the Pediatric Emergency Care Applied Research Network rule and practically important traumatic brain injury outcomes were validated.
Results:
We enrolled and analyzed 433 children below 2 years. The most frequently observed mechanisms of injury in decreasing order were as follows: falls > 90 cm, head struck by high-impact objects, slip down, and automobile traffic accident. Of 224 children, positive findings were observed in 35 and 144 had one or more predictors of Pediatric Emergency Care Applied Research Network rule. The sensitivity, specificity, and negative likelihood ratio of the Pediatric Emergency Care Applied Research Network rule for practically important traumatic brain injury were 94.3%, 41.3%, and 0.14, respectively.
Conclusion:
The Pediatric Emergency Care Applied Research Network rule would assist in clinical decision-making to appropriately detect potential head injuries in children below 2 years, thereby reducing unnecessary performance of computed tomography scan.
Keywords
Introduction
Traumatic brain injury (TBI), the prominent cause of death or disability in children, is generally caused by minor head trauma (account for 70%–90%). 1 Particularly, Children below 2 years of age are easily susceptible to such trauma, because of a relatively large head, thin and flexible skull, inadequate protective maneuver, and soft and vulnerable brain. Minor head trauma is predominantly characterized by a history of blunt trauma to the head with a demonstration of alertness or awakening to voice or light and touch, respectively; this indicates a Glasgow Coma Scale (GCS) score above 13. Notably, GCS score of 8 or less is recognized as severe TBI. 2 In an event of death resulting from head trauma, neurosurgery, mechanical breathing for a period beyond 24 h, and hospitalization for 48 h, the significance of clinical diagnosis is reiterated by describing the “clinically important TBI” (ciTBI). 3 However, only less than 5% of these minor head traumas are categorized as clinically important head injuries.3–5 “Practically important TBI” (piTBI) was further described as ciTBI including all cranial abnormalities such as skull fracture detected by computed tomography (CT). In very young children with minor head trauma, the concept of piTBI is of relevance because unusual findings cannot be overlooked in cranial CT scan even without the requirement of a momentary hospitalization.
Cranial CT scan is employed as a standard diagnostic tool for rapid evaluation in the emergency department (ED); however, it is posed with challenges including an increase in cancer rate owing to irradiation. Therefore, in the treatment of a child with minor head trauma by a physician, the actual challenge is deciding the child to be evaluated and the time of discharge. These clinical decisions are, however, required to be made rapidly and accurately because of the relatively common incidence of visiting the ED due to minor head trauma and the steady increase in the adoption of cranial CT scan.6,7 Another challenge is the inappropriate expression of symptoms in children (below 2 years or of preverbal age). The clinical evaluation of children in this age group is generally more difficult, thereby reducing the confidence of the clinicians in the assessment of older children. In addition, even with intracranial injury, asymptomatic cases are frequently observed and piTBI such as skull fracture could occur. Moreover, children in this age group are sensitive to radiation; therefore, reduction of cranial CT imaging is of great importance.
A number of guidelines have been recently suggested; one of these is a popularly known age-specific prediction rule, the Pediatric Emergency Care Applied Research Network (PECARN) rule.8,9 The PECARN prediction rule (published in 2009) suggested an algorithm for cranial CT scan with the use of seven risk factors. 3 It was proposed that cranial CT scan can be instantaneously conducted at a high risk of 14 points (of GCS) or other manifestations of an altered mental status, or palpable skull fracture. In the case of other risk factors, CT scan was described as an intermediate risk based on the physician’s experience and the exacerbation of symptoms. In the absence of these risk factors, CT scan was not suggested because of the extremely low risk. Therefore, this study aimed to assess the diagnostic accuracy of a clinical decision rule (PECARN rule) and physician discretion in the recognition of piTBIs in children (below 2 years) with minor head trauma presenting to the ED in a single institution.
Methods
Study design and setting
A retrospective cohort study was conducted to investigate the applicability of the PECARN prediction rules in children below 2 years with minor head trauma. The medical records of the children were reviewed in the ED of a University-affiliated Training Hospital from January 2013 to December 2015. The hospital is a regional level 1 trauma center for both adult and pediatric patients. The study was approved by the Institutional Review Board of the hospital and was conducted in accordance with relevant guidelines and regulations. Due to the retrospective design of the study, the Ethics Committee waived the requirement to obtain informed consent.
PECARN prediction rule (age <2 years)
PECARN TBI prognostic rule is a scoring system for predicting the requirement for cranial CT scan in children with minor blunt head trauma described by GCS scores of 14–15. 3 This rule comprises two age-based criteria as follows: children below 2 years and the ones between ages of 2 and 18. A ciTBI is described as a head injury resulting in one or more of the following: death, neurosurgery, intubation for a period beyond 24 h, and TBI-related admission for two or more nights in the hospital. The predictor variables for children below 2 years were as follows: GCS score of 14, other prognostics of altered mental status (agitation, somnolence, repetitive questioning, slow response to verbal communication), palpable skull fracture, non-frontal hematoma, history of impaired consciousness ⩾5 s, serious mechanisms of injury (automobile crash with patient ejection, death of another passenger, or a rolled-over pedestrian/bicyclist without helmet struck by motorized vehicle, falls >90 cm, and head struck by high-impact objects), and not acting normally per parent.
Selection of participants
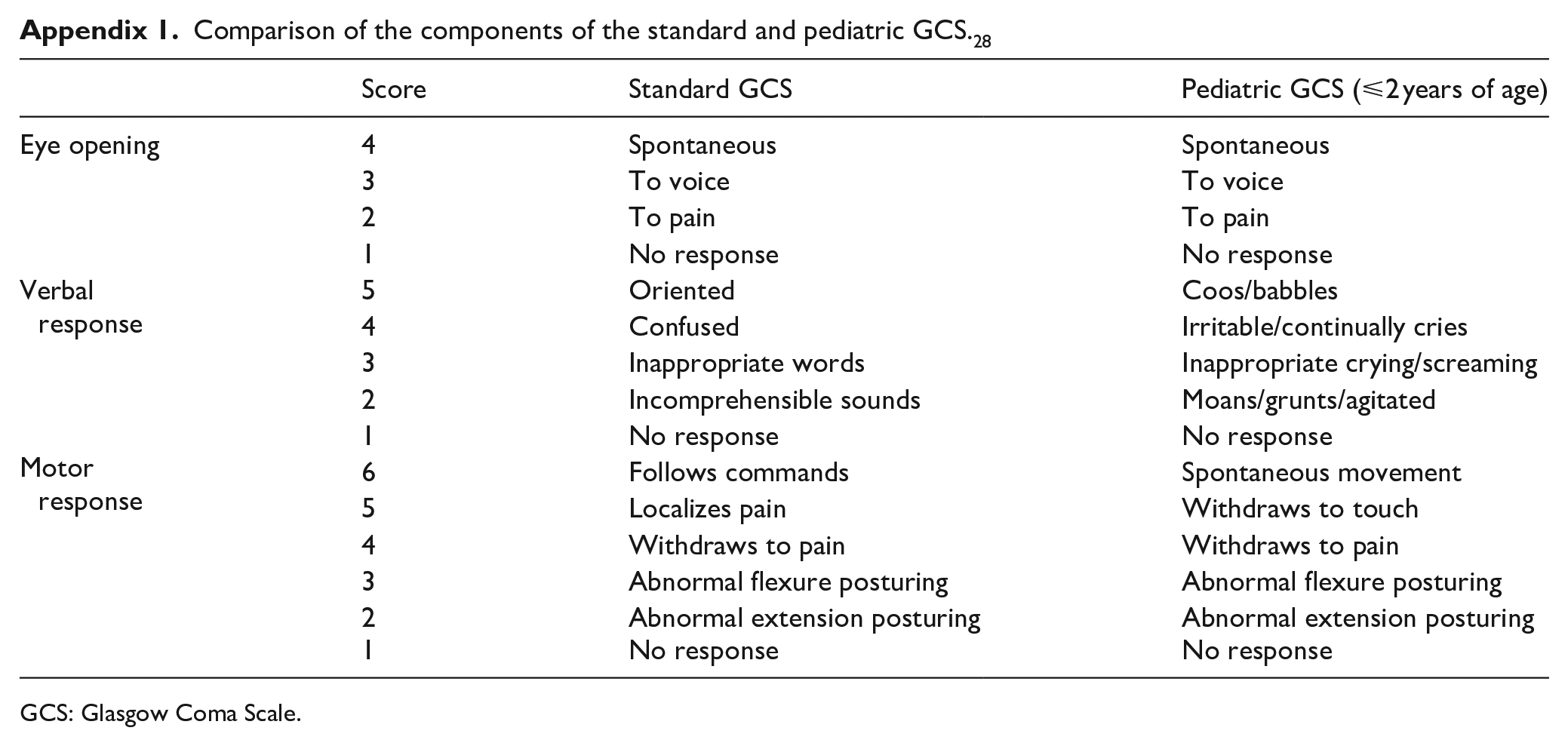
Children below 2 years with minor head trauma (GCS 14–15) who presented to ED within 24 h of their injuries were included. We used the pediatric GCS score for preverbal children, age-appropriate modifications to account for developmental differences in verbal, motor, and cognitive abilities (Appendix 1). On the contrary, children with penetrating trauma, known brain tumors, pre-existing neurological disorders, and who died prior to admission to the emergency ward were excluded. In addition, suspected cases of non-accidental trauma, insignificant facial injury only, or serious injuries to other body parts were excluded.
Methods of measurement
Patients were categorized following the PECARN checklist by the attending ED physicians. Four ED physicians with over 5 years of experience were involved in the study; all were faculty staffs who were knowledgeable of the PECARN rule. Cranial CT scan was performed in accordance with the clinical discretion of the ED physician. In particular, in the intermediate risk group, CT scan was recommended on the basis of other clinical factors including the experience of the physician, multiple versus isolated findings (isolated loss of consciousness, isolated headache, isolated vomiting, and certain types of isolated scalp hematomas in infants older than 3 months), worsening symptoms or signs after ED observation, age <3 months, and parental preference. 3 CT scans were interpreted by radiologists, and positive findings on the CT scan were defined by any the descriptions as follows: intracranial hemorrhage, brain contusion, cerebral edema, traumatic infarction, diffuse axonal injury, shearing injury, sigmoid sinus thrombosis, midline shift or herniation, diastasis of the skull, traumatic pneumocephalus, or depressed skull fracture in line with the PECARN study.
Outcome measure
In this study, the ciTBI (cited in the PECARN study) was elaborated to employ the concept of piTBI including all abnormalities detected in the cranial CT scan. In the event it failed to satisfy the ciTBI criterion, there are cases requiring a clinical close observation, particularly in children below 2 years. In a way similar to ciTBI, the study population was structured into three groups (at risk of piTBI) according to the PECARN prediction rules as follows: children with one or more high-risk predictors (GCS score of 14 or altered mental status, or palpable skull fracture) as high risk, children with one or more intermediate-risk predictors (serious mechanisms of injury, impaired consciousness >5 s, non-frontal hematoma, and not acting normally according to parent) as intermediate risk, and children with none of the predictors as extremely low risk. All predictor variables of PECARN rule and outcomes of piTBI were validated.
Statistical analysis
Statistical analyses were performed using SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA) and MedCalc ver. 15.8 (MedCalc Software, Ostend, Belgium). Continuous and categorical data were presented as mean with standard deviation, and frequency with a percentage, respectively. T test was employed for relevance between continuous data. On the contrary, chi-square and Fisher exact tests were employed for categorical variables. Sensitivity, specificity and positive, and negative likelihood ratios (LRs) were estimated to evaluate the value of PECARN rule in the prediction of piTBI and were expressed in percentages with the 95% Clopper–Pearson exact confidence interval (CI). The receiver operating characteristic (ROC) curve was utilized to ascertain the predictive utility of the PECARN rule for piTBI diagnosis. Notably, p < 0.05 was considered statistically significant in all analyses.
Results
Baseline characteristics
In the course of the study, 433 children below 2 years, who presented with blunt head trauma to the ED within 24 h following trauma, were included. In accordance with the PECARN prediction rule, distribution of high risk, intermediate risk, and extremely low risk children were 35 (8.1%), 137 (31.6%), and 261 (60.3%), respectively (Figure 1). The demographics and other clinical characteristics are illustrated in Table 1. Mean age was 11.6 ± 5.5 months and 277 (63.9%) children were males. In decreasing order, the most frequently observed mechanisms of injury were as follows: falls > 90 cm (42.3%), head struck by high-impact objects (30.9%), slip down (22.2%), and in-car traffic accident (4.6%). Notably, 191 (44.1%) children were not subjected to any imaging studies. Of 224 children who underwent cranial CT scanning, positive findings were observed in 35 (15.6%) (20 and 15 children with skull fracture and intracranial hemorrhage, respectively), who were further categorized as piTBI. Only a patient underwent neurosurgery (0.2%). Notably, none of 408 (94.2%) children who were discharged from ED revisited the hospital.
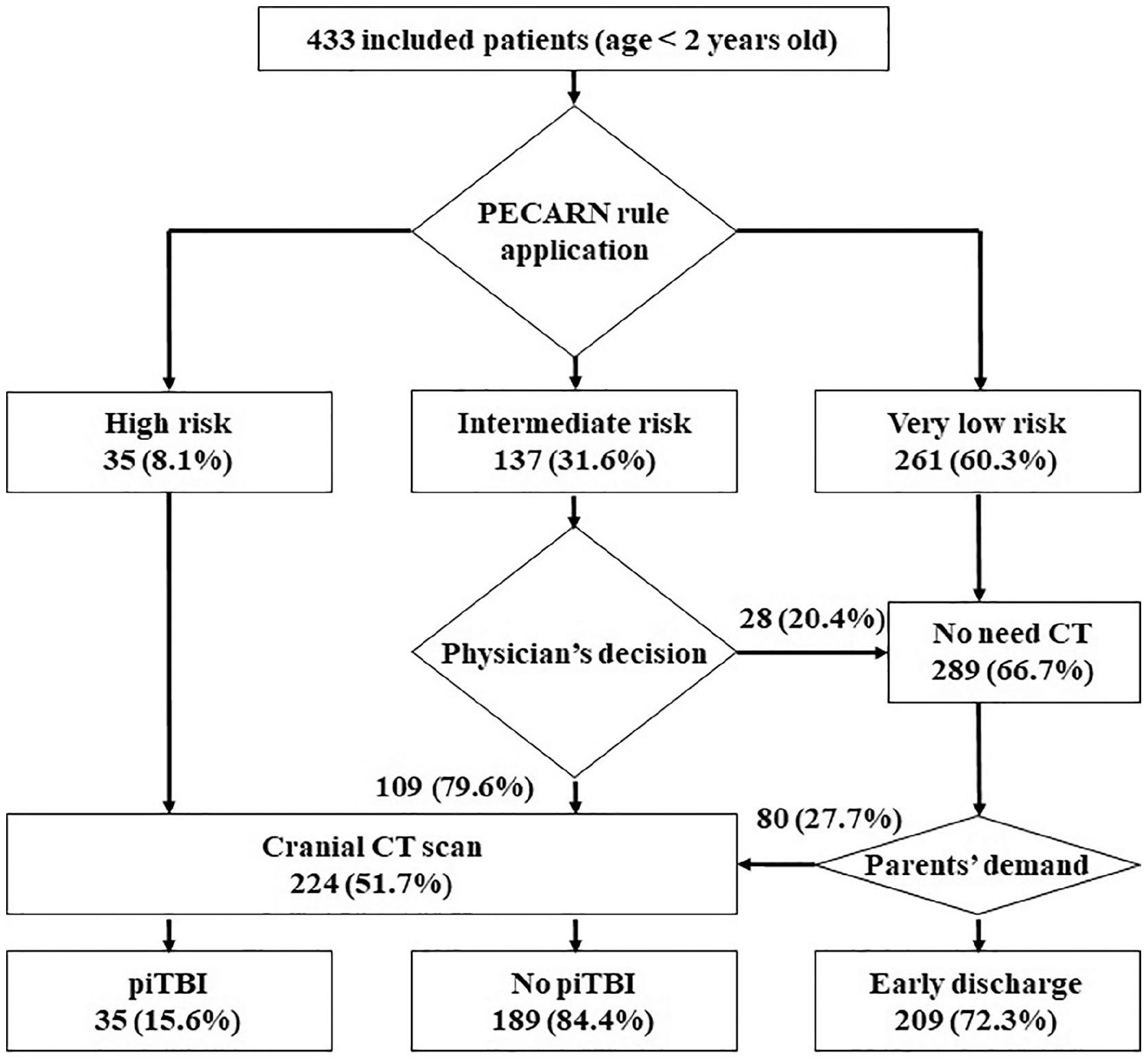
Study flow chart.
Clinical characteristics of the study group (N = 433).
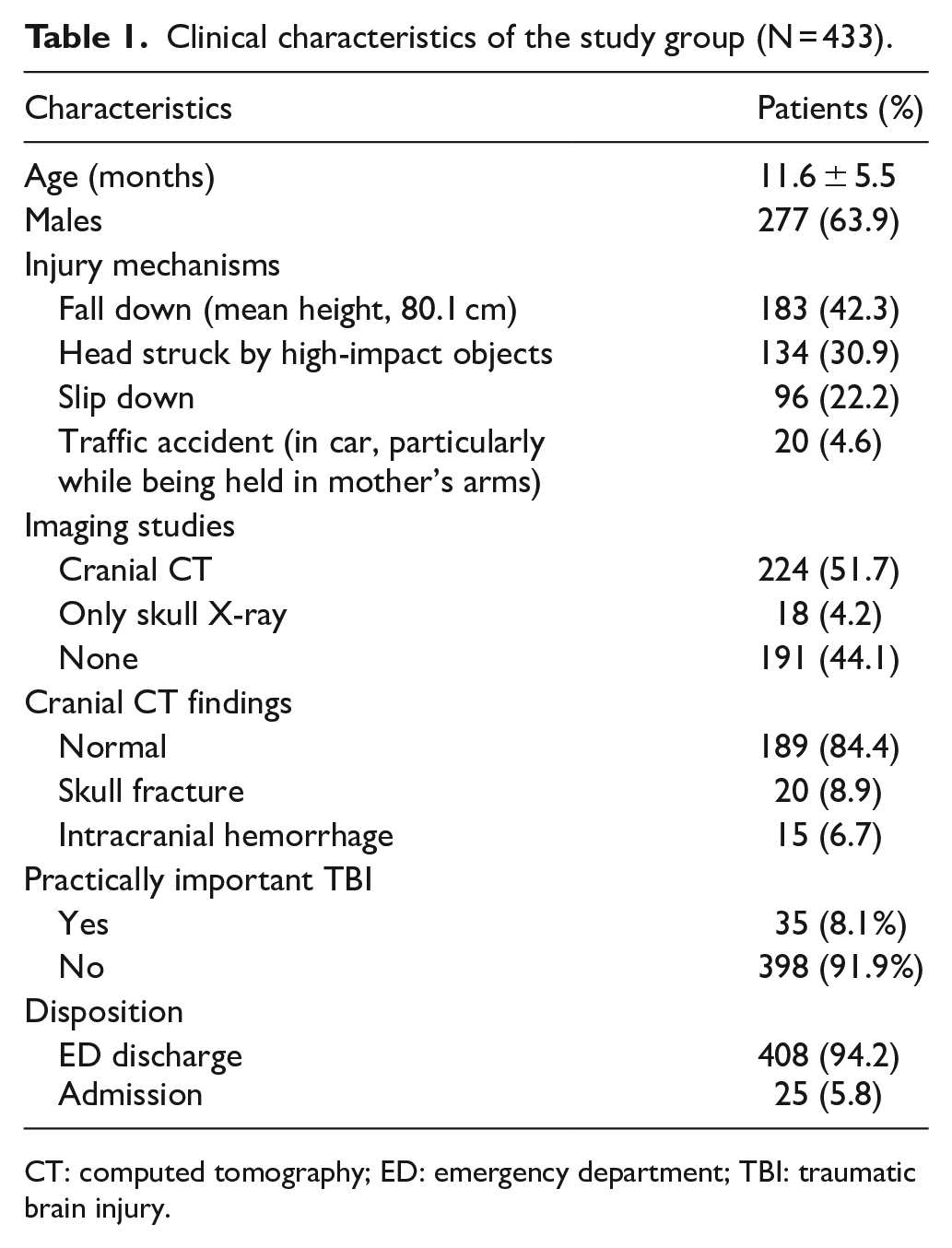
CT: computed tomography; ED: emergency department; TBI: traumatic brain injury.
Application of PECARN rule
Of 224 children who underwent cranial CT scan, 144 (64.3%) children possessed one or more predictors of PECARN rule. This included 109 of 137 patients in the intermediate risk group, and CT scans were recommended in consideration of the other clinical factors mentioned above. In addition, 80 (35.7%) children were subjected to cranial CT scan on the request of their guardians, rather than the discretion of the physician. For analysis, the children were classified into “Meet group” or “Not meet group” based on the presence of predictors. As indicated in Table 2, no difference was observed in age and gender between both groups. Statistically, piTBI was significantly greater in the Meet group (22.9%) than the Not meet group (2.5%); accordingly, dissimilarity was observed with regard to admission. Simple linear skull fracture was observed in all children with piTBI (in the Not meet group) on cranial CT and skull X-ray. Interestingly, no significant difference was observed with regard to any of the following: duration of ED stay, ratio of supplementary sedation for imaging study (from ED visit to home discharge or emergency ward), the requirement of sedation in imaging, and conformance with the PECARN rule. An elongation in the time spent in the ED was observed due to the unwarranted sedation and CT use of various caregivers, who refused the suggestion of the physician.
Comparison of patients according to PECARN rule in the performance of cranial CT scan (N = 224).
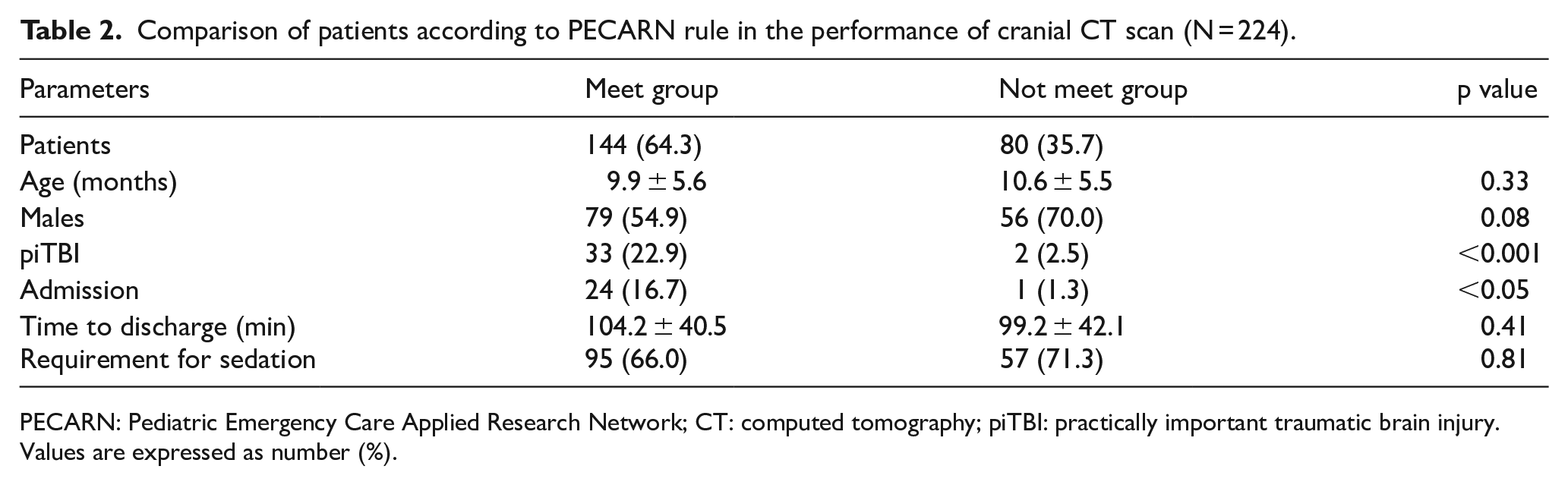
PECARN: Pediatric Emergency Care Applied Research Network; CT: computed tomography; piTBI: practically important traumatic brain injury.
Values are expressed as number (%).
PECARN risk factors for piTBI
Table 3 reveals the distribution of PECARN risk factors alongside the outcomes. The piTBI group demonstrated an average of 2.26 for risk factors compared to the non-piTBI group, and the greater the risk factors, the larger the probability of piTBI. In addition to the high risk factors, it was observed that non-frontal hematoma and severe mechanisms of injury were factors of significance in the intermediate risk group. In conclusion, a statistically significant probability of no brain lesion was additionally observed in the absence of a risk factor. Simple linear fracture was observed in two children (with piTBI) who possessed no PECARN risk factor. The diagnostic accuracy of the PECARN rules was assessed for the prediction of piTBI presence as demonstrated in Table 4. The sensitivity, specificity, and negative LR of the PECARN rule for piTBI were 94.3%, 41.3%, and 0.14, respectively. Figure 2 illustrates the ROC curve; the area under the curve (AUC) in the ROC curve delineated into the low, intermediate, and high-risk groups was estimated as 0.734, which was further established as a satisfactory diagnostic tool.
Distribution of PECARN risk factors with outcomes (N = 224).
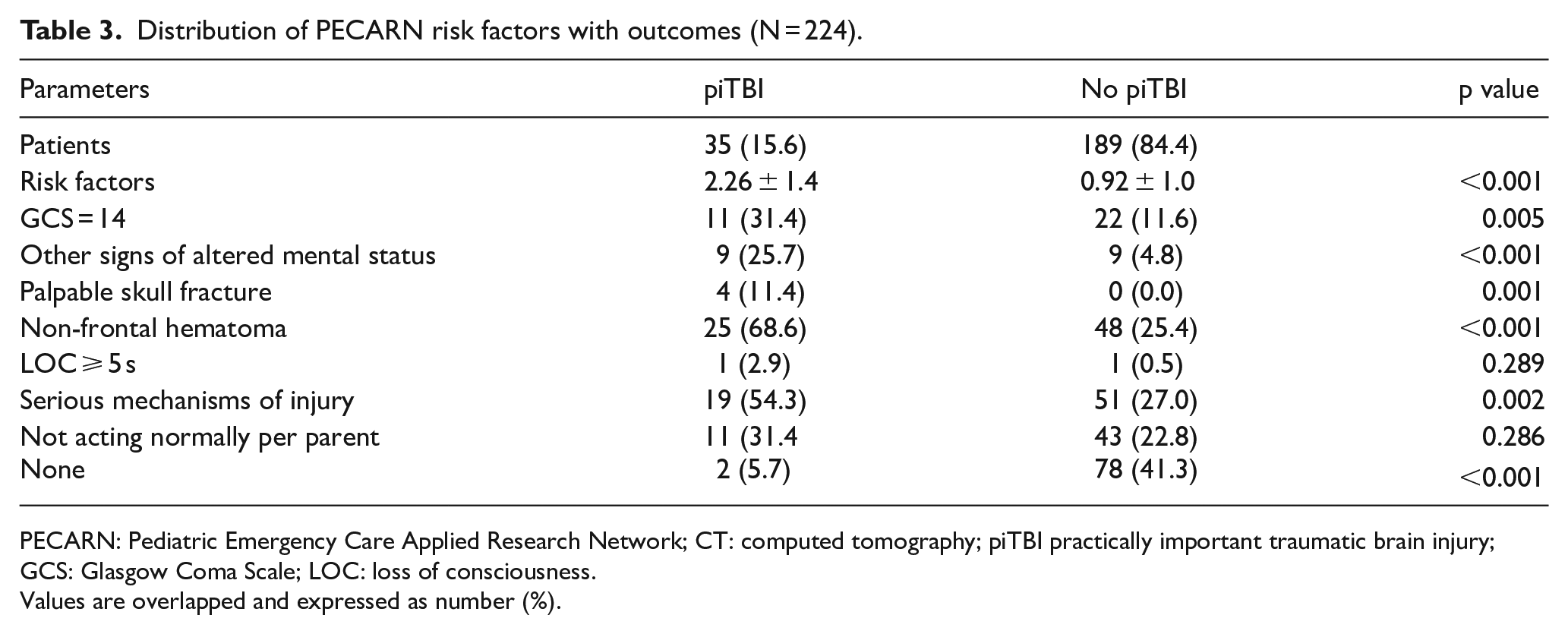
PECARN: Pediatric Emergency Care Applied Research Network; CT: computed tomography; piTBI practically important traumatic brain injury; GCS: Glasgow Coma Scale; LOC: loss of consciousness.
Values are overlapped and expressed as number (%).
Statistical analysis of PECARN rule for piTBI (N = 224).
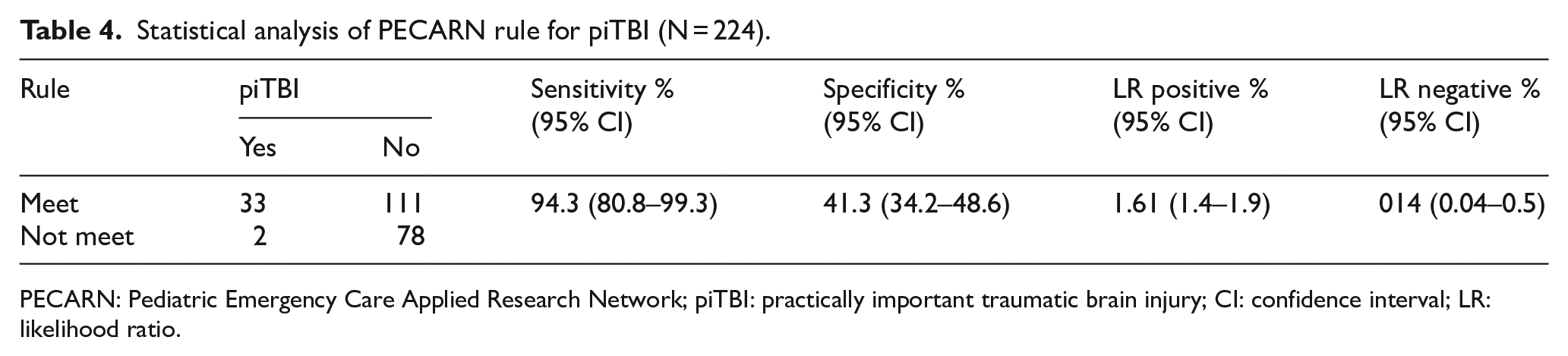
PECARN: Pediatric Emergency Care Applied Research Network; piTBI: practically important traumatic brain injury; CI: confidence interval; LR: likelihood ratio.
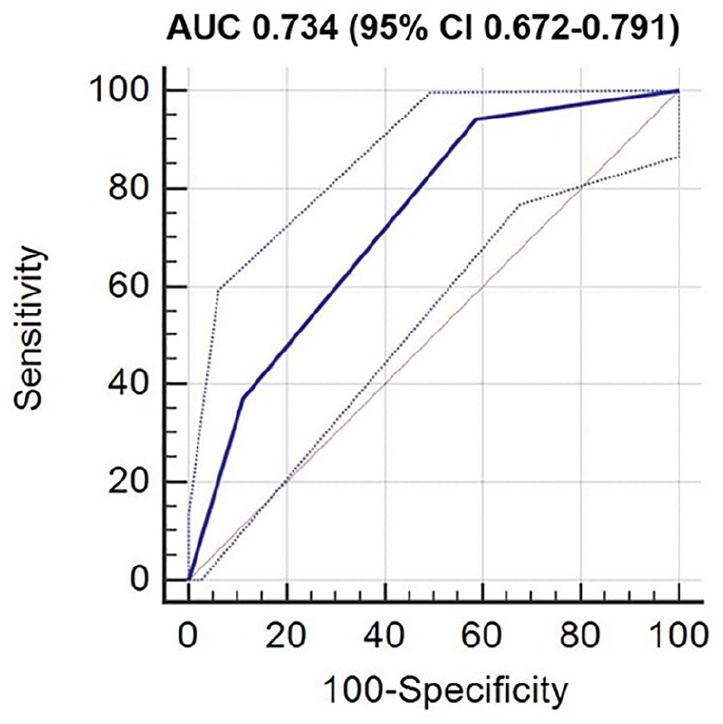
ROC curve of PECARN rule for piTBI.
Discussion
A retrospective cohort study was conducted to evaluate the value of PECARN rule in the prediction of piTBI in children below 2 years with minor head trauma. It was observed that the incidence of piTBI was 8.1% among 433 children, of which 94.3% had PECARN risk factors. The diagnostic value of the PECARN rule for piTBI is great sensitivity (94.3%), fair AUC (0.734), and considerable LR negative (0.14).
Majority of past studies related to cranial CT decision-making aimed to identify ciTBI requiring acute intervention, particularly neurosurgery.3,4,10–12 CT scan is performed only when ciTBI is suspected to reduce the risk of exposure to radiation; however, ciTBI has an extremely low incidence in the range of 0.67% to 1.13%.3,11 TBIs such as numerous skull fractures and ciTBI are observed in less than 10% of CT scans in children with minor head trauma.13–16 In this study, only one patient underwent neurosurgery (0.2%); however, piTBI was relatively high at 8.1%. The skull fracture included in piTBI has been demonstrated to be more frequent in children below 2 years following head trauma. Unlike other age groups, a separate indication is required for CT scan in this age group because the clinical manifestations of intracranial brain injury are not reliable enough. 17 Although majority of simple linear skull fractures required no acute intervention, caution should be exercised with regard to underlying brain injuries.18–20 A study by Powell et al. 21 revealed novel intracranial findings on subsequent CT scan such as small subdural hematoma, extra-axial hematoma, and cerebral contusion in 3 (1.4%) of 222 children with minor head trauma (below 2 years of age) and isolated skull fracture. No child was managed with neurosurgery acknowledging the parents’ concerns; it is therefore obvious that the child’s condition should be closely monitored. Therefore, cranial CT scan should be employed in the detection of piTBI, rather than ciTBI in an actual clinical setting.
Owing to the accessibility of CT scan and the application of novel CT technologies such as low dose radiation protocol, CT is getting more regularly implemented. 6 In a total of 433 patients, CT scans were performed in 224 (51.7%), 35.7% of which were conducted on the request of parents, rather than the physician’s discretion. Furthermore, delay was observed in the time of home discharge and supplementary sedative therapy was conducted due to unplanned CT imaging. Parents could anticipate CT scan to guarantee an absence of “bleeding” in their children’s brains with a deficiency of information on its risk and advantage. 22 In intermediate-risk children, this preference could partly affect 29% to 54% of CT scan rate. 23 There are still concerns about the inordinate performance of CT scans; however, needs of caregivers cannot be easily disregarded in actual clinical practice. Therefore, rational and fair guidance on appropriate CT scanning is required.
PECARN prediction rule is an optimal screening tool in the recognition of high-risk ciTBI children with mild TBI, which was reported a sensitivity in the range of 85.7% and 100% in children below 2 years.3,12,24,25 In a recent prospective cohort study, this rule had a 100% sensitivity and negative predictive value, respectively, for the incidence of ciTBI in this age group. 4 Application of the prediction rule could minimize unwarranted CT scanning and a lifetime hazard of radiation-induced fatal cancer rates in children ranging from 0.03% to 0.08%.26,27 Interestingly, in a validation study on children who presented with minor head trauma to the ED 24 h after injury, power of PECARN clinical decision rules (to exclude any TBI in cranial CT scan) was lower in the late admission group than the early admission group. 10 It was observed that 94.3% of children with piTBI possessed one or more PECARN risk factors; in addition, this prediction rule for piTBI had a negative LR of 0.14, a value evidently less than 1, indicating its significant utility as a diagnostic tool for screening. Furthermore, high-risk variables can apparently differentiate the piTBI group; however, intermediate-risk variables play a negligible role in the decision regarding the performance of CT scan. 22 In Table 3, variables such as “impaired consciousness >5 s” and “inappropriate parental roles” identified in the report of the guardian showed no significant difference between the piTBI and non-piTBI groups.
This study has some limitations; the most significant is the retrospective nature of the study design and the limited number of recruited patients; these could result in possible selection bias. Therefore, in the future, well-designed large-scale prospective investigations are warranted. In addition, patients discharged from the ED were not followed up; hence, children with piTBI who were consequently confirmed at other hospitals could have been undetected. However, considering the fact the institution is a regional level 1 trauma center and the regional culture of parents revisiting the hospital even for minor skull fractures because of excessive concerns, this would be uncommon. Furthermore, 80 out of 289 patients who were classified as “no need CT scan” had a CT scan in response to the demands of parents and were included in the piTBI analysis. This may affect the calculation of the diagnostic performance of the PECARN rule. However, there are also positive aspects that indicate the actual clinical situation. In conclusion, the comprehensive concept of piTBI was restricted to skull fractures. Because skull fractures can be ascertained by simple X-ray alone, there is an ethical perspective on the performance of a CT scan. However, since a CT scan is required to evidently recognize the intracranial lesion, balanced guidelines are essential.
Because of a susceptible brain, an extended indication for cranial CT scan is required in children below 2 years of age (with minor head trauma) compared to other age groups. It is necessary to establish guidelines that can support the reduction of anxiety in parents about TBIs of importance in the clinical field and assist ED physicians in the conduction of diagnostic tests. The PECARN rule would assist in clinical decision-making to appropriately detect potential head injuries in children below 2 years with mild head trauma, thereby reducing unwarranted CT use.
Footnotes
Appendix
Comparison of the components of the standard and pediatric GCS. 28
| Score | Standard GCS | Pediatric GCS (⩽2 years of age) | |
|---|---|---|---|
| Eye opening | 4 | Spontaneous | Spontaneous |
| 3 | To voice | To voice | |
| 2 | To pain | To pain | |
| 1 | No response | No response | |
| Verbal response | 5 | Oriented | Coos/babbles |
| 4 | Confused | Irritable/continually cries | |
| 3 | Inappropriate words | Inappropriate crying/screaming | |
| 2 | Incomprehensible sounds | Moans/grunts/agitated | |
| 1 | No response | No response | |
| Motor response | 6 | Follows commands | Spontaneous movement |
| 5 | Localizes pain | Withdraws to touch | |
| 4 | Withdraws to pain | Withdraws to pain | |
| 3 | Abnormal flexure posturing | Abnormal flexure posturing | |
| 2 | Abnormal extension posturing | Abnormal extension posturing | |
| 1 | No response | No response |
GCS: Glasgow Coma Scale.
Authorship
J.S.K. collected the data, drafted, and edited the manuscript. J.C.K. collected and analyzed the data. W.Y.S. designed and supervised the study and reviewed the manuscript. All the authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Eulji University Hospital Institutional Review Board (No. 2016-11-002) and was performed in accordance with the relevant guidelines and regulations.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The need to obtain informed consent was waived due to the retrospective design of the study. And the consent waiver was approved by the Eulji University Hospital Institutional Review Board (No. 2016-11-002).
Human rights
This study was approved by the Eulji University Hospital Institutional Review Board (No. 2016-11-002), in compliance with the Informed Consent, Ethical Approval, and Human Rights clauses set forth by the Hong Kong Journal of Emergency Medicine publishing guidelines.
Availability of data and materials
The data sets generated and/or analyzed during this study are available from the corresponding author on reasonable request.