
Abstract
Butterfly vertebra and block vertebra are usually reported incidental radiological view, which is a rare congenital defect of spine. Butterfly vertebra is a body formation characterized by anterior and median aplasia. The block vertebra is the result of an embryonically incomplete separation of vertebral bodies or arches or both. This rare congenital anomalies butterfly and block vertebra are usually stable and do not cause clinical symptoms.
Case 1
A 39-year-old female patient presented to our emergency department after motor vehicle accident. She continued to complain of back pain and has no neurological deficit. Examination showed that her spine was fully mobile, but she was tender over the spinous process of T6-12. In the initial radiological evaluation, T8 vertebra height loss was found in the anteroposterior (AP) and lateral view radiographs (Figure 1).
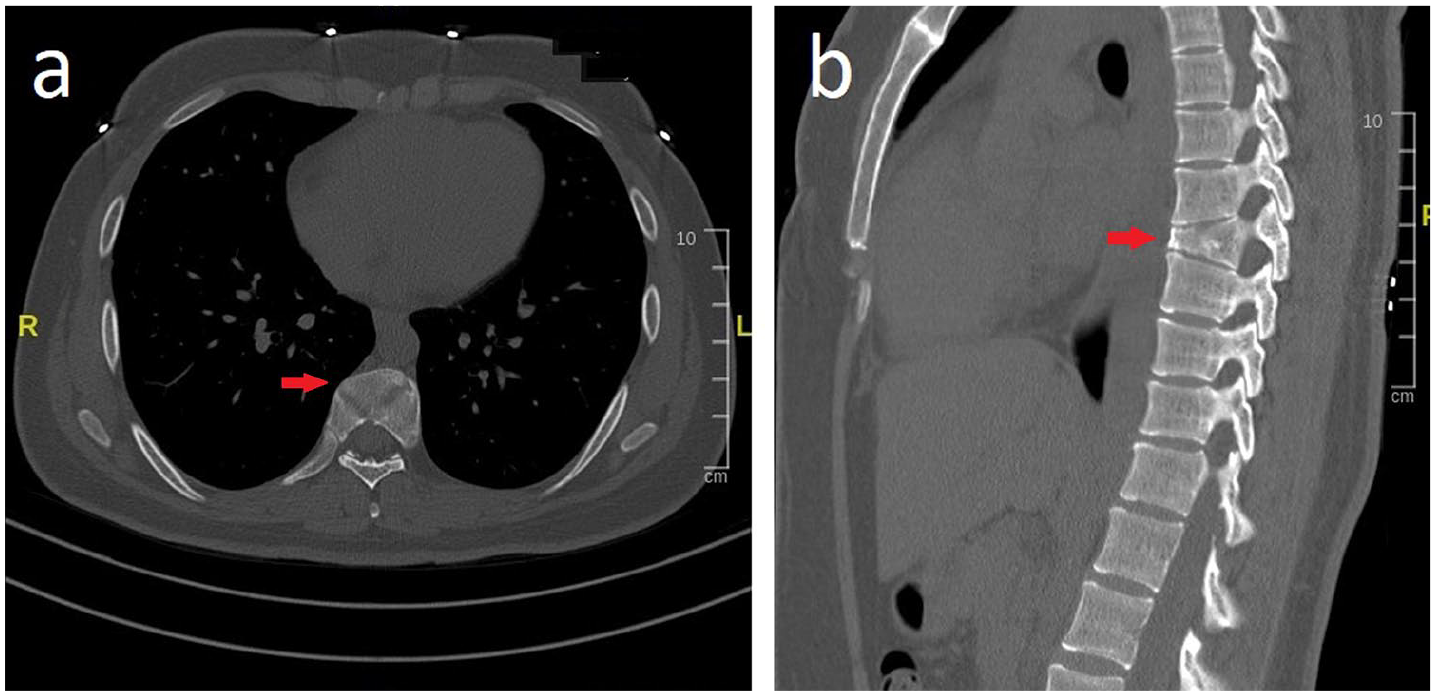
CT scan of the thoracic spine and T8 vertebra height loss (arrow).
Furthermore, evaluations of the tomography and three-dimensional (3D) computed X-ray tomography showed that the presumed injury was a butterfly and block vertebra. This rare congenital anomaly is usually asymptomatic, and awareness of its non-traumatic nature is critical in order to establish a correct diagnosis (Video 1 of Supplemental material).
Case 2
A 38-year-old male presented to the car accident and emergency department with crushing back pain. He was the driver. Neurological examination is normal. On examination, there was a clear sensitivity—sensitivity in the middle line of the dorsal part, at the T3-4 level of the thoracic vertebra. The patient describes a localized pain at that area. Other systemic examinations were normal.
In the computed tomography examination of the patient, loss of height in the anterior of the T5 vertebra corpus and block vertebra were observed in T11-12 vertebra.
These cases were detected accidentally and it was not known by the patients that they had vertebral anomalies before (Figure 2).
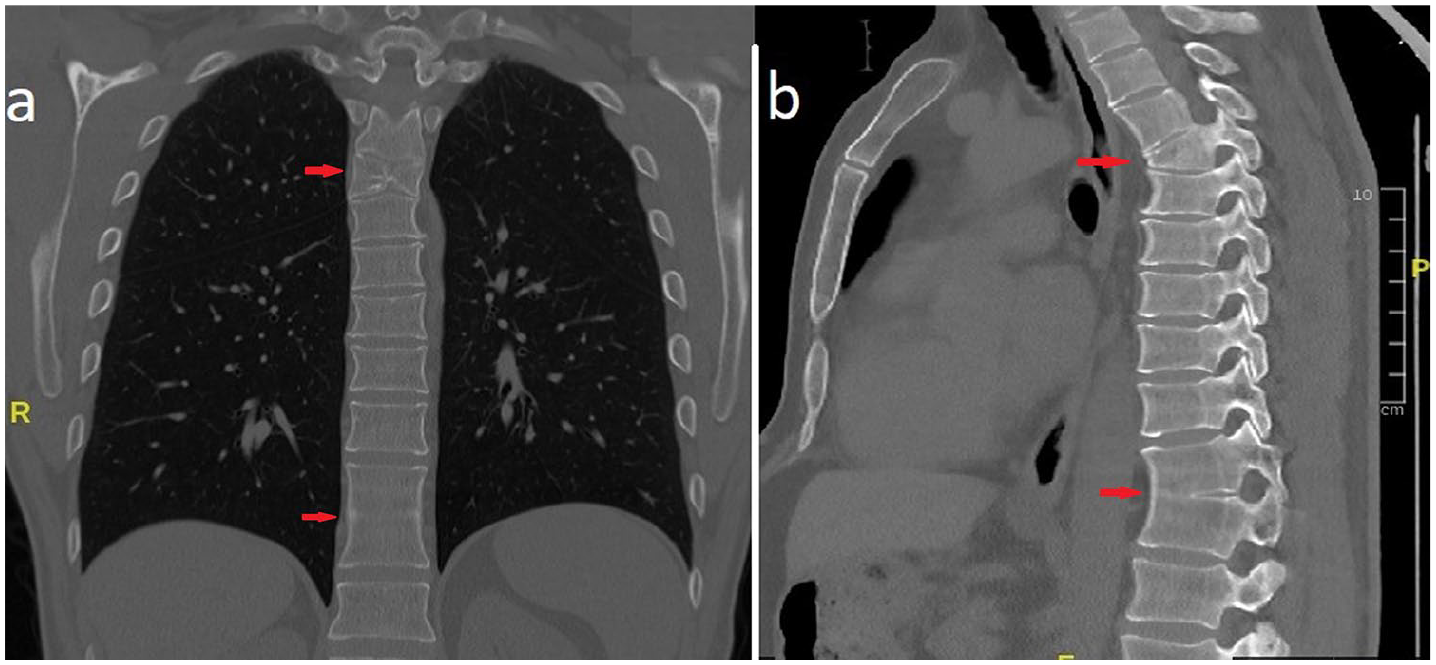
CT scan of the upper segment of the block vertebra showing the appearance of the butterfly vertebra and block vertebra (arrow).
Discussion
This rare congenital anomaly, which is usually without clinical significance, may be mistaken for a wedge fracture unless the AP view is correctly assessed. Furthermore, in the emergency setting, awareness of this entity is needed so that a correct diagnosis can be established.1,2 In simple AP radiographs or computed tomography, the butterfly shape of the body of the vertebra is easily identifiable, while the pedicles may look divergent. In the lateral X-ray view, the butterfly vertebra usually presents with as a wedge-shaped deformity, which may be confused for a compression fracture.1,2 The butterfly vertebra is identified on an AP radiograph as two hemivertebra separated by an empty space, with compensatory midline elongation of the adjacent vertebra. 3 Cases was otherwise healthy and had no significant history of a genetic syndrome. However, multiple abnormalities of the cardiovascular system and aortic arch have been reported to occur with butterfly vertebra, specifically coarctation of the aorta, dextrocardia, and teratology of Fallot. 4 Although it can be seen with multiple or other anomalies in butterfly vertebra, it is rare with block vertebra as in Case 2. 5 It is important to recognize butterfly vertebra on imaging as generally benign and not part of other pathological processes such as trauma or genetic disease. Further evaluation of the patient is necessary to exclude pathologic fracture, infection, or associated vertebral anomalies and syndromes. Furthermore, in the emergency setting, awareness of this entity is needed so that a correct diagnosis can be established. The cases reporting the presence of butterfly vertebra as an incidental finding, 3D tomography is very useful in defining butterfly vertebra.
People who have block vertebra and hemiblock vertebra malfunction may not be aware of their condition because they do not have any symptoms. Knowing these vertebral anomalies by physicians will save patients from unnecessary imaging and follow-up time.
Footnotes
Acknowledgements
The authors thank the dispatch and paramedics in the study area.
Author contributions
İ.B.E. and A. S. were involved in research concept and design. S.K., A.S., and F.R. were involved in writing of this article. Ç.C. and İ.B.E were involved in critical revision of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
There is no additional date available.
Informed consent
Informed consent form is available
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.