
Abstract
Introduction:
Shock index is defined as heart rate divided by systolic blood pressure. It is reported as a predictor of morbidity and mortality in trauma and acute myocardial infarction in previous studies. It may be valuable in evaluation of calcium channel blocker poisoning. The objective of this study is to examine the probability of serious outcome based on first measured shock index in patients who presented to emergency department with calcium channel blocker poisoning.
Methods:
A retrospective chart review was conducted on calcium channel blocker poisoning cases in Hong Kong Poison Information Centre from 1 July 2008 to 30 June 2017. Shock index was calculated with blood pressure and pulse measurement at emergency department triage. Odds ratios of various variables for major outcome, mortality, intensive care unit admission, length of stay in acute hospital were calculated by multivariate analysis or negative binomial regression where appropriate. The performance of shock index in predicting major outcome was evaluated with receiver operating characteristic curve.
Results:
A total of 390 cases were identified, of whom 25.1% developed major outcome and 5.6% died. Shock index showed significant association with major outcome (odds ratio: 17.017, 95% confidence interval: 5.521–52.455). The area under the receiver operating characteristic curve for shock index in predicting major outcome was 0.7008 (95% confidence interval: 0.64–0.76).
Conclusion:
Higher shock index is associated with worse patient outcome in calcium channel blocker poisoning. However, shock index alone is not reliable in predicting patient outcome. Further research is needed before shock index can be incorporated for use in patient management in poisoning with calcium channel blocker or other anti-hypertensives.
Introduction
Background
Shock index (SI) is defined as heart rate divided by systolic blood pressure. It is postulated to reflect on stroke volume and cardiac output. 1 Studies on its use in trauma patients identified SI as an independent predictor of increased mortality 2 and transfusion requirement.3–5 It is especially useful at an early stage of hypovolaemia with relatively normal blood pressure.6,7
Use of SI is also investigated in myocardial infarction. Studies show that SI is a predictor of mortality in acute ST-elevation and non-ST-elevation myocardial infarction.8–11
SI can also help in identifying critically ill patients in the general emergency department setting with heterogeneous patient presentations. 12 Higher SI measured at triage at emergency department is associated with higher rate of hospital admission and inpatient mortality.1,13,14
However, data on SI in toxicology patients are lacking. Toxicity from cardiovascular drugs causes significant mortality. Cardiovascular drug ranked as the second commonest agent involved in poisoning deaths reported to poison centres in the United States in 2015. 15 Among cardiovascular drugs, calcium channel blockers accounted for 40% on the death cases. 15 Hence calcium channel blocker poisoning is chosen for investigation in this study.
Calcium channel blockers inhibit voltage-gated L-type calcium channels and decrease calcium influx into myocardial cells and vascular smooth muscle cells. Hypotension is a feature of significant toxicity and is due to the exaggeration of the therapeutic effects, namely a combination of negative myocardial inotropy, chronotropy and vasodilatation. 16
We postulate that in patients with calcium channel blocker poisoning, higher values of SI reflect poorer haemodynamic status and hence can predict poorer outcomes.
Study objective
The objective of this study is to examine the probability of serious outcome based on first-measured SI in patients who presented to emergency department with calcium channel blocker poisoning.
Methods
Study design and setting
This is a retrospective chart review of cases in clinical database of Hong Kong Poison Information Centre (HKPIC), from 1 July 2008 to 30 June 2017.
HKPIC provides consultation on poison information and management advice to all healthcare professionals in Hong Kong. It also receives poison reporting from Hospital Authority. It receives more than 3000 consultations and reporting cases each year.
The database (Poison Information and Clinical Manage-ment System – PICMS) contains consultation and reporting cases. The data of each poisoning case were fed to PICMS according to information obtained from the consulting health care professional, medial record, electronic patient record (ePR) of Hospital Authority and other relevant sources.
Description of study subjects
Patients were recruited through data search in the database of HKPIC. Poisoning cases were collected to the database through phone consultation or Hospital Authority poison reporting system.
Inclusion criteria
All patients aged 18 years or older and who were labelled as calcium channel blocker poisoning during the period were included in the review. They were identified by data search in PICMS database.
Exclusion criteria
Patients with unmeasurable blood pressure at triage, incomplete record of blood pressure and heart rate at triage, incomplete clinical records and those with subsequent confirmed non-exposure are excluded. Prisoners were not included in this study.
Variable and outcome
Variables that were recorded for each patient encounter include demographic data, toxin data, and clinical data. Demographic data include age and sex of patient. Toxin data include name and dose of calcium channel blocker ingestion, other co-ingested substance, and the reason of exposure. Clinical data include the first set of blood pressure and pulse measured at triage of emergency department, treatment received, disposition and outcome of the patient.
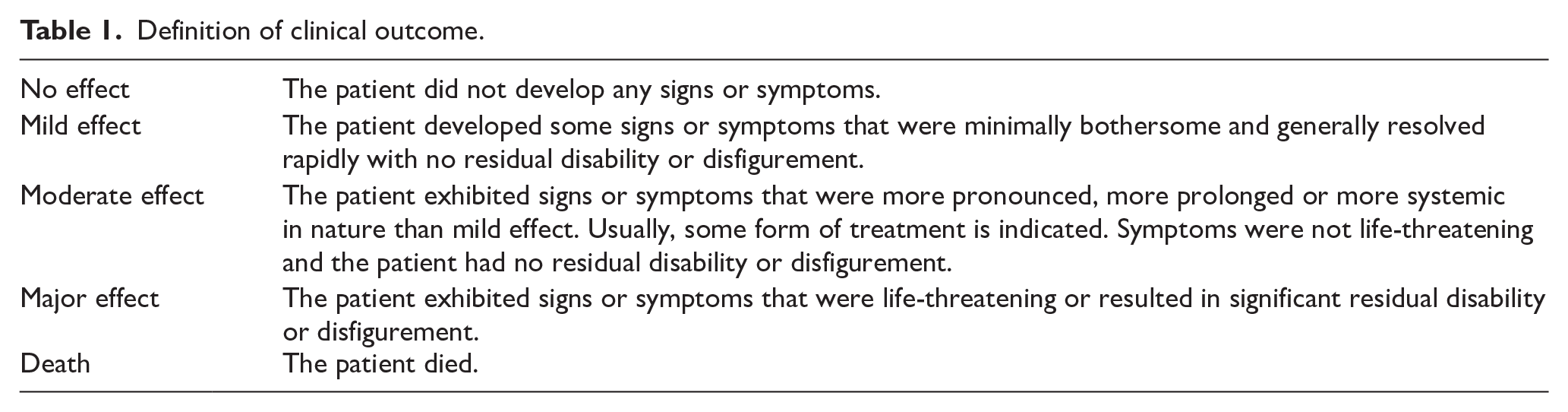
Patient outcome was classified by clinical toxicologists in HKPIC with reference to the American Association of Poison Control Centres’ National Poison Data System. It is divided into five categories: no effect, mild effect, moderate effect, major effect or death, as listed in Table 1. 17 Patient outcome was fed to the PICMS database for every case according to the available clinical information.
Definition of clinical outcome.
Primary and secondary outcomes
Primary outcome of this study is the occurrence of major effect or death (major outcome).
Secondary outcomes include mortality, admission to intensive care unit (ICU) and length of stay in acute hospital ward.
Sample size and calculation
A previous study demonstrated area under receiver operating characteristic (ROC) curve of SI in predicting major injury in trauma patients to be 0.6. 18 Prevalence of major effect or death in calcium channel blocker poisoning is estimated to be 0.25 based on previous experience. Sample size calculation is based on a formula proposed by Obuchowski and Mcclish. 19 Assuming margin 0.1, alpha 0.05, beta 0.2, required sample size for comparison of area under curve is at least 332.
Data collection
The clinical records including Accident and Emergency Department attendance record and in-patient discharge summaries were retrieved from computer database PICMS. The blood pressure and heart rate at triage were recorded on paper record of each patient in emergency department, which was scanned and stored into the database. The blood pressure and heart rate for each patient were manually extracted from scanned paper records to a spreadsheet.
Only data relevant to study purpose were recorded, which include basic patient demographic information including age, sex and other relevant clinical information.
Statistical analysis
Univariate and multivariate regression analysis was performed on association of variables with the primary outcome, mortality and ICU admission. Length of stay in acute hospital was analysed using negative binomial regression, and mortality cases were assigned to have the longest length of stay. P value less than 0.05 is defined as statistically significant.
The optimal cutoff for SI in predicting serious outcome in calcium channel blocker poisoning is not known, so the performance of SI in predicting serious outcome in calcium channel blocker poisoning was evaluated by receiver operating characteristic curve.
The statistical analysis was performed using SPSS, version 20.0.
Results
During the period of 1 July 2008 to 30 June 2017, 411 cases of calcium channel blocker poisoning were recorded in the database. Twenty-one of those cases were excluded: 14 had outcome unrelated to calcium channel blocker exposure, 1 had undetectable blood pressure at emergency department, 6 cases were not presented to emergency departments; so 390 cases were included in the final analysis. Patients’ characteristics are shown in Table 2.
Patients’ characteristics.
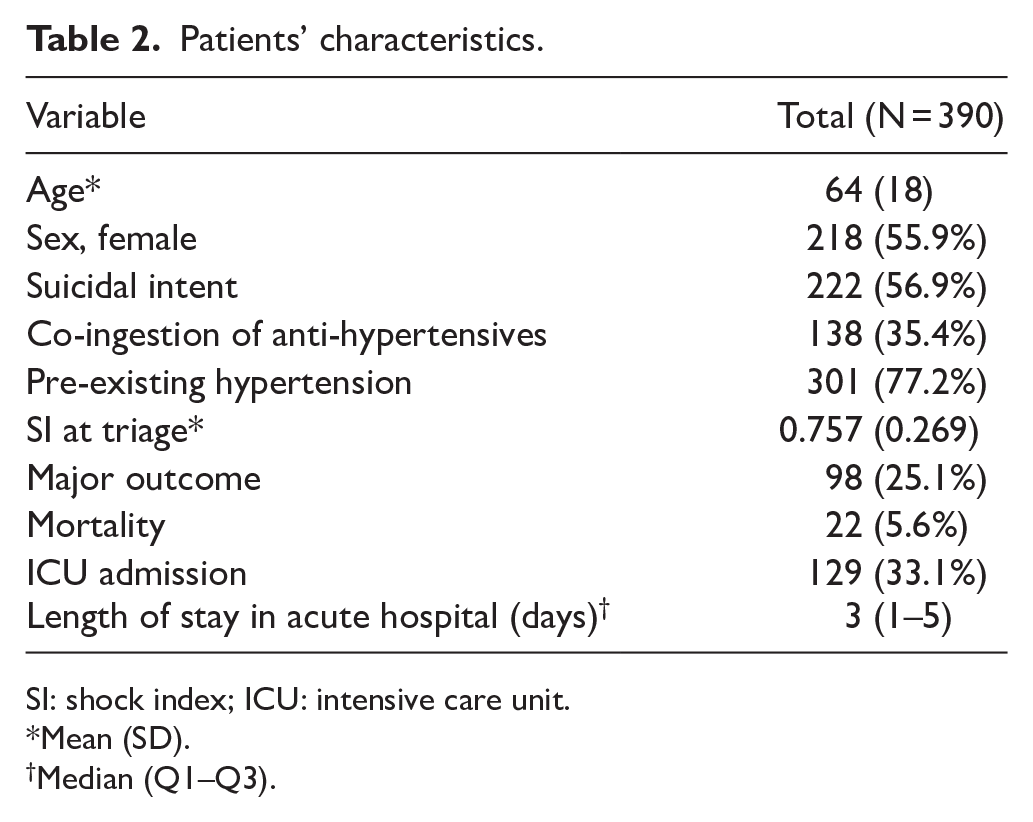
SI: shock index; ICU: intensive care unit.
Mean (SD).
Median (Q1–Q3).
Univariate analysis on association of variables with major outcome, mortality and ICU admission was performed. Age, pre-existing hypertension, anti-hypertensives co-ingestion, suicidal intent and SI were considered to have potential association with the outcomes and analysed. It showed that suicidal intent and SI had significant association with all three outcome measures (Table 3).
Univariate analysis of variables related to major outcome, mortality and ICU admission.
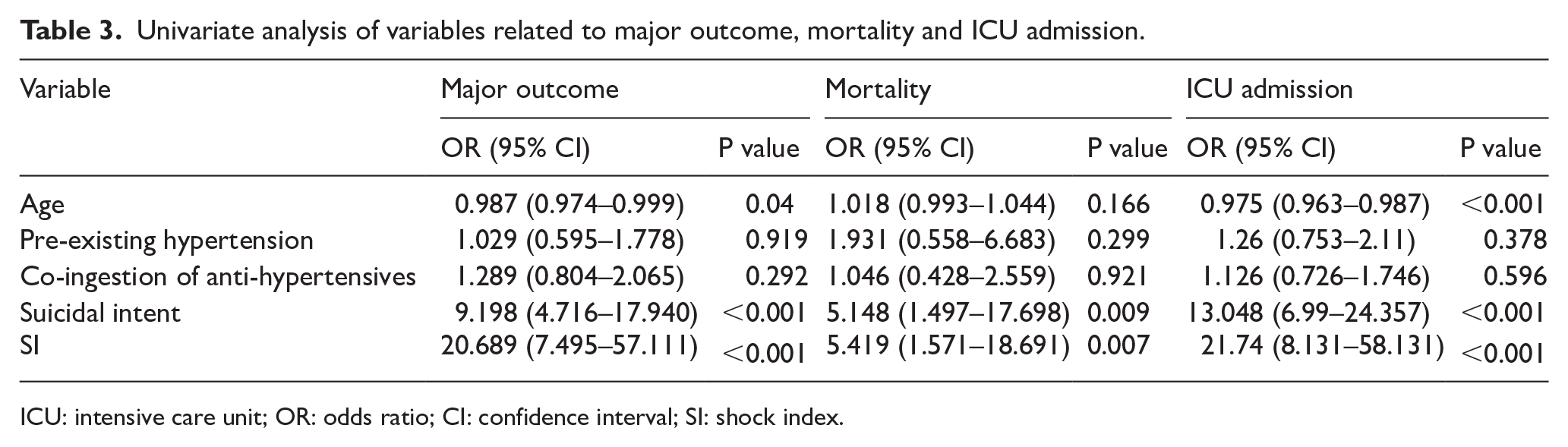
ICU: intensive care unit; OR: odds ratio; CI: confidence interval; SI: shock index.
In the multivariate analysis, final model was created for major outcome, mortality and ICU admission by the backward conditional method. The results are shown in Table 4.
Multivariate analysis of variables.
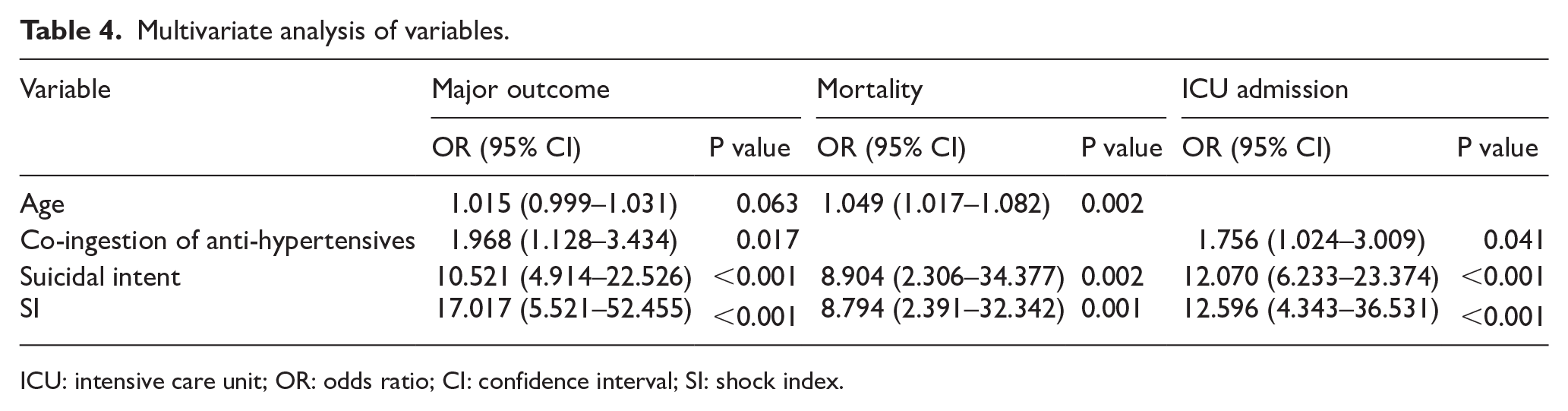
ICU: intensive care unit; OR: odds ratio; CI: confidence interval; SI: shock index.
SI had the strongest association with major outcome with an odds ratio of 17.017 (95% confidence interval (CI): 5.521–52.455). Suicidal intent had odds ratio of 10.521 (95% CI: 4.914–22.526). Anti-hypertensives co-ingestion had odds ratio of 1.968 (95% CI: 1.128–3.434). Age was only borderline significant with odds ratio 1.015 (95% CI: 0.999–1.031).
Length of stay in acute hospital was analysed using negative binomial regression, and mortality cases were assigned to have the longest length of stay. SI had the strongest association with length of stay with odds ratio 4.177 (95% CI: 2.3337–7.4779; Table 5).
Length of stay in acute hospital (negative binomial regression).
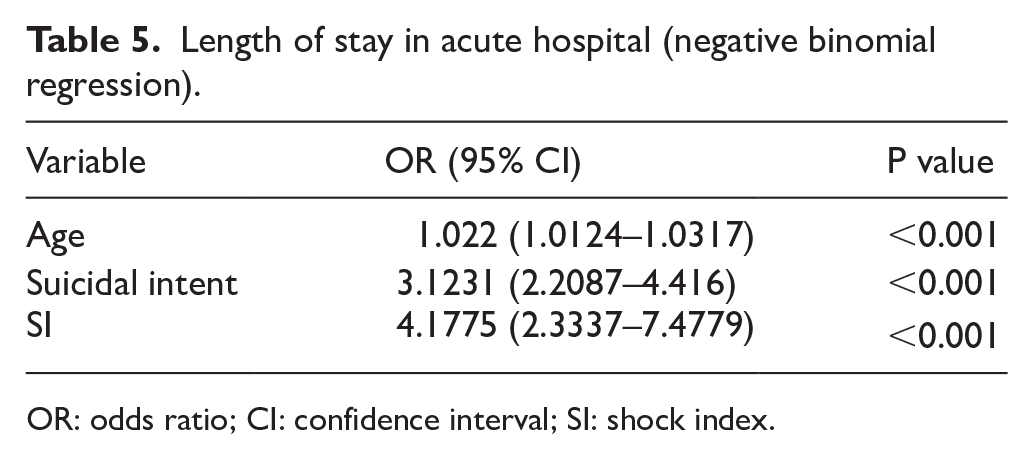
OR: odds ratio; CI: confidence interval; SI: shock index.
Figure 1 shows the receiver operating characteristic curve for SI in predicting major outcome. SI had area under the curve of 0.7008 (95% CI: 0.64–0.76).
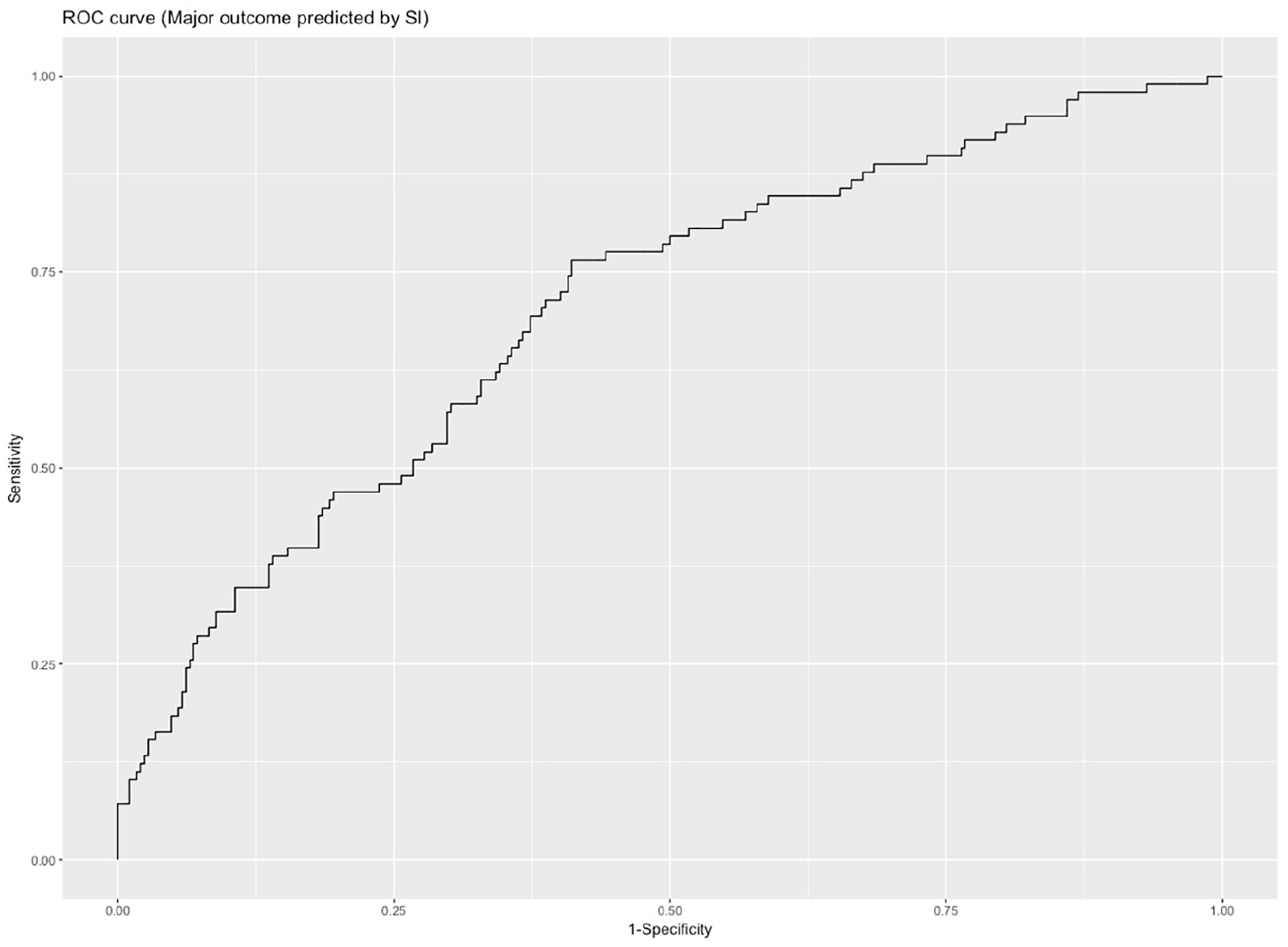
Receiver operating characteristic curve of major outcome prediction with shock index.
The operating characteristic of SI is included in Table 6.
Operating characteristics of SI in predicting major outcome.
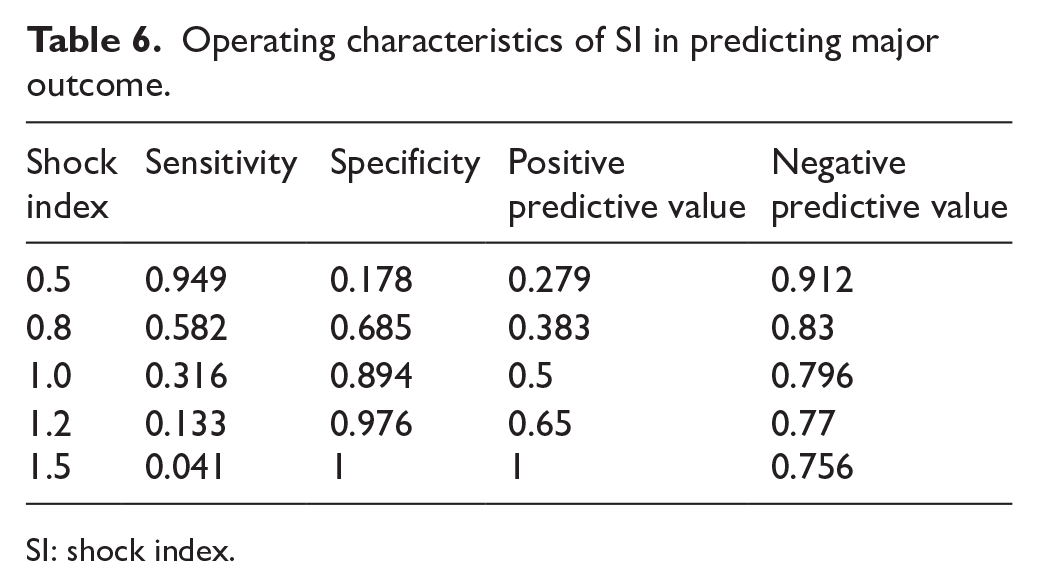
SI: shock index.
Discussion
Calcium channel blocker poisoning causes significant morbidity and mortality. Prompt recognition of patients who are more likely to develop serious outcome is necessary, as it can guide whether to give more aggressive gastrointestinal decontamination treatment and intensive monitoring.
In this study, SI is calculated by systolic blood pressure and heart rate measured at triage in patients with calcium channel blocker poisoning presenting to emergency department. The association of SI and major outcome is examined with multivariate logistic regression. SI was demonstrated to have significant association with major outcome, mortality, ICU admission, and length of hospital stay. This is compatible with our proposed theory that greater value of SI reflects worse haemodynamic status of the patient and hence predicts poorer outcome in patients.
In the analysis of the operating characteristic, SI had only fair performance as a sole predictor of major outcome. This suggests that although SI is associated with serious outcome, there are other important determinants. One possible factor is that a single SI measurement alone does not have sufficient predictive power to predict patient outcome. In a previous study conducted in trauma patients, the change of SI from pre-hospital to emergency department is also a sensitive predictor of mortality. 20
Anti-hypertensives co-ingestion was only shown to have mild association with outcome. There are different anti-hypertensives each with different toxicity profiles, and they affect the blood pressure and heart rate to different extents. Because of small sample size, only the presence or absence of anti-hypertensives co-ingestion was counted in the analysis. The significance of anti-hypertensive co-ingestion in predicting outcome may be underestimated.
This study has several limitations.
First, the blood pressure and pulse were usually measured by nurses at triage using an automated machine. In extremes of blood pressure or irregular pulse, this could lead to inaccurate measurements. This retrospective study cannot prevent this source of error.
Second, the poisoning cases in the database were collected from the treating physicians on a voluntary basis through reporting and consultation. Less severe cases may not be collected.
Third, calcium channel blockers can be classified into dihydropyridines and non-dihydropyridines. They produce different clinical features in overdose. Dihydropyridines produce reflex tachycardia while non-dihydropyridines such as diltiazem and verapamil produce bradycardia.16,21 The issue is further complicated as there are cases with ingestion of both dihydropyridines and non-dihydropyridines. Subgroup analysis could not be done due to the small size of the group with non-dihydropyridines ingestion.
Fourth, due to the retrospective nature of this study, the data on dosage of calcium channel blockers ingestion is incomplete. In many cases, the dosage ingested was not reported or was uncertain. While it is clear that the toxicity of calcium channel blockers is dose-dependent, the relationship between dosage of calcium channel blockers ingested and SI and outcome cannot be shown in this study because of this limitation.
In conclusion, higher SI is associated with more serious patient outcome in calcium channel blocker poisoning. However, SI alone is not reliable in predicting patient outcome. Further research is needed before SI can be incorporated for use in patient management in calcium channel blocker poisoning or other anti-hypertensives poisoning.
Footnotes
Author contributions
M.T.L. researched the literature, conceived the study, gained ethical approval, collected data and wrote the first draft of the manuscript. Both authors were involved in development of the research protocol and data analysis. Both authors reviewed and edited the manuscript and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data
The data sets generated and/or analysed during the current study are available from the corresponding author.
Informed consent
Informed consent was waived by the Hospital Authority Research Ethics Committee.
Ethical approval
The study was approved by the Hospital Authority Research Ethics Committee, Kowloon Central/Kowloon East. (KC/KE-17-0178/ER-3), and the study protocol comply with the Declaration of Helsinki.