
Abstract
Background:
Hong Kong rates of bystander cardiopulmonary resuscitation are very low by international standards. Several Hong Kong secondary schools have begun incorporating cardiopulmonary resuscitation training into their curriculums for teachers and students.
Objective:
This study aimed to explore secondary school cardiopulmonary resuscitation programs and better understand school principals’ attitudes toward cardiopulmonary resuscitation training.
Methods:
A cross-sectional survey was sent to all Hong Kong secondary school principals (public and private, except for special education schools) between December 2017 and March 2018. A self-administered questionnaire of 20 items focusing on school characteristics, details of any in-school cardiopulmonary resuscitation materials or training, attitudes toward teaching cardiopulmonary resuscitation, and any barriers or ways to promote school cardiopulmonary resuscitation training was given to all school principals in the territory. This study was approved by the Survey and Behavioural Research Ethics committee of the Chinese University of Hong Kong on September 13, 2017.
Results:
Out of the 506 schools contacted, 110 completed surveys were returned (21.7%). Cardiopulmonary resuscitation training was offered in 33.6% (37/110), while 92.7% (102/110) had an automatic external defibrillator. A majority (69.1% (76/110)) agreed or strongly agreed that cardiopulmonary resuscitation training should be compulsory for secondary school students. In schools where cardiopulmonary resuscitation was taught, most cardiopulmonary resuscitation students were aged 15–17 years, and most courses ran for < 5 h. Increased funding could encourage more schools to offer cardiopulmonary resuscitation training to students in the future.
Conclusion:
One-third (33.6%) of Hong Kong secondary schools offer cardiopulmonary resuscitation training. Increased funding may support school-based cardiopulmonary resuscitation instruction and improve rates of bystander cardiopulmonary resuscitation in the future.
Introduction
Despite advances in resuscitation, out-of-hospital cardiac arrest (OHCA) survival rates in most regions of the world remain low. OHCA survival rates vary greatly between different countries and health systems, ranging between 2% and 11%.1,2 A territory-wide study evaluating the epidemiological characteristics and outcomes of OHCA patients in Hong Kong found an incidence of 72 per 100,000 person-years—higher than the mean global incidence of 55 per 100,000 person years—alongside a very low survival to hospital discharge rate of 2.3%. 2 For comparison, the United States has an overall OHCA survival rate of 10.6% and survival with good neurologic function rate of 8.3%. 3 A local study showed that despite most Hong Kong residents reporting a willingness to summon assistance for victims of OHCA, there remains a reluctance to perform cardiopulmonary resuscitation (CPR), and rates of bystander CPR in Hong Kong remain as low as 20.4%. 4 Bystander performed CPR has been associated with three times the rate of survival for cases of OHCA with ventricular fibrillation. 5 One possible reason for low rates of bystander CPR in Hong Kong is that most laypersons receive little to no training in CPR or in the operation of automated external defibrillators (AEDs). 4
To encourage bystanders to intervene and potentially save more lives, Hong Kong has embraced a multifaceted approach to varying success. Approaches include utilizing a mobile-phone application to quickly locate AEDs in public settings, the installation of AEDs in public places, the provision of CPR and AED training to school staff through the “Heart-safe School Project,” 6 and, most recently, the “Anyone” mascot created by the Hong Kong Fire Services Department (HKFSD) to promote the message that “anyone can save lives.” 7 In Hong Kong, approximately 40% of OHCAs were witnessed with most occurring at home, 2 meaning the timely application of life-support skills by family members including older children can play a key role in improving outcomes for OHCA in Hong Kong.
One solution for increasing rates of bystander CPR is mandating resuscitation teaching in schools. In 2003, the International Liaison Committee on Resuscitation (ILCOR) suggested the incorporation of CPR into school curriculums, and shortly after the American Heart Association (AHA) recommended training in CPR for every teacher and student. 8 Secondary school students are the primary target for CPR training, given their relative maturity and physical development compared with younger students while still being in school thanks to near-universal secondary school attendance in most developed countries. 8 Students and teachers can become “multipliers” forming a group of trained individuals passing on life-saving skills to the community. 9 To date, most local efforts to educate teachers and students about CPR and AEDs are carried out by nongovernmental organizations, namely, the Hong Kong Red Cross (HKRC) and the Hong Kong St. John Ambulance societies. Recently, the HKFSD has also launched multiple educational campaigns including the “CPR Training Program on Campus” for schools, the “Press to Shock—Save a life” public access defibrillation course and the “Community Awareness on Responding to Emergency (CARE)” program for community CPR training. 10 Although multiple school-based resuscitation education programs have been conducted overseas in Spain, Singapore, and New Zealand, and legislation mandating compulsory training was recently established in Denmark, Canada, and several states in the United States,11,12 the current situation regarding CPR training and implementation in Hong Kong secondary schools is still unknown.
The Education Bureau of Hong Kong currently mandates that “at least two teachers in every school shall be trained in the administration of first aid” and has advised schools to encourage staff to “attend first aid training courses regularly” in preparation for medical emergencies on school premises. 13 Schools are currently not required to provide resuscitation training for their students, 14 and there have to date been no studies investigating the prevalence or acceptance of CPR training in Hong Kong secondary schools. This study aimed to determine what percentage of Hong Kong secondary schools provide CPR training to their students, what CPR resources are available in these schools, and explore school principals’ attitudes toward CPR training in their schools.
Methods
This was a cross-sectional, self-administered survey performed between December 2017 and early March 2018. As of the 2017/2018 academic year in Hong Kong, there were a total of 506 secondary schools in Hong Kong. Of the 506, 473 were “local” schools that teach primarily in Cantonese and English (31 government supported, 360 aided (run by charity organizations), 61 direct-subsidy scheme, 2 caput (nonprofit private schools that charge the same rates as public schools), and 22 private). There were also 33 “international” schools (i.e. schools that teach in English as well as the language of the sponsoring nation such as English and French at the French International School). 15 All 506 secondary school principals or their delegates were invited to participate in this study. One survey was distributed per school.
Each survey contained 20 questions divided over three sections (see Supplemental Appendix 1 for survey instrument). Section one included basic questions regarding the school and also questions related to CPR training efforts, including (a) availability of AEDs, (b) participation in the “Heart-safe School” project, (c) proportion of staff trained in resuscitation skills, and (d) whether schools currently offered resuscitation training. Only schools currently offering a CPR course were invited to complete section two of the survey. Data regarding course instructors, duration, content, target student population, barriers to training, and feedback from participating students were collected in this section. All respondents were then invited to complete section three, which sought their opinions about barriers to CPR training, what measures could help with promoting CPR training in schools, and whether schools were supportive of integrating such training into the curriculum. The questionnaire was distributed via email or fax. Email reminders were used to enhance the response rate.
Demographic characteristics of schools were compared based on their attitude toward incorporating CPR into the school curriculum. Descriptive statistics were used to report characteristics of resuscitation programs currently on offer and feedback from participating students after completion. Opinion questions were also analyzed using descriptive methods. Statistical analysis was performed using SPSS v.25 (IBM corp., Armonk, NY, USA). Pearson’s chi-square test or Fisher’s exact test were used where appropriate, and p values < 0.05 were considered statistically significant. This study was approved by the Survey and Behavioral Research Ethics committee of the Chinese University of Hong Kong on September 13, 2017.
Results
A total of 128 questionnaires were initially collected from 506 secondary schools (25.3%). One survey was excluded as it came back from a primary school; 17 did not answer questions about the integration of CPR into their school curriculum and were thus excluded (Figure 1).
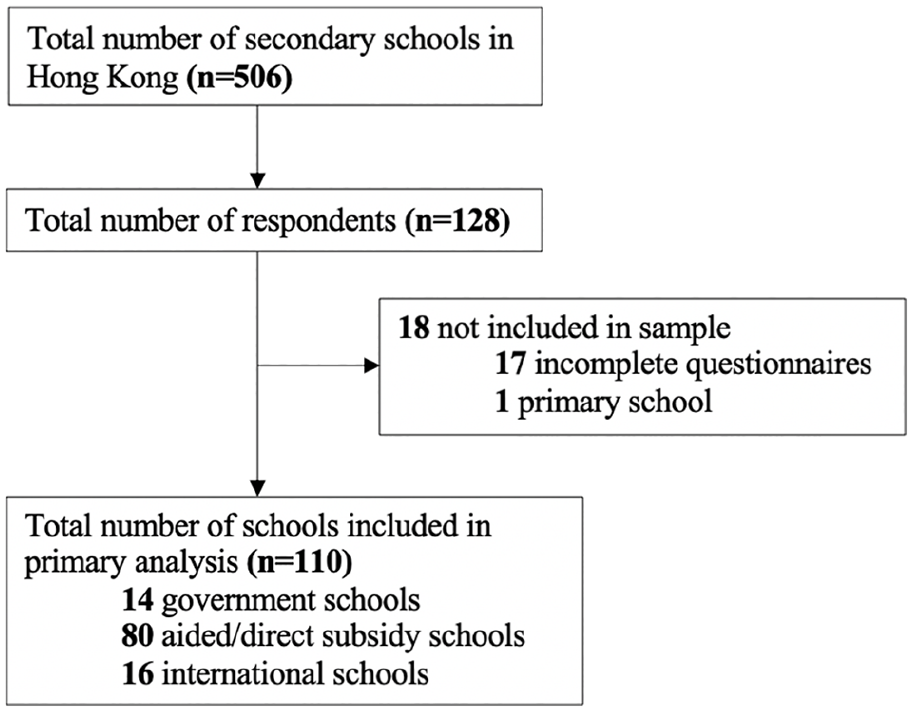
Study flowchart.
The final response rate was 21.7% (110/506). Supporters (69.1%, 76/110) and non-supporters (30.9%, 34/110) of CPR training in schools were compared by type of school, staff, student population, the number of staff with existing resuscitation knowledge, availability of AEDs, participation in the “Heart-Safe School Program,” and availability of a CPR course (Table 1).
Demographic characteristics of secondary schools based on principals’ attitude toward CPR curriculum.
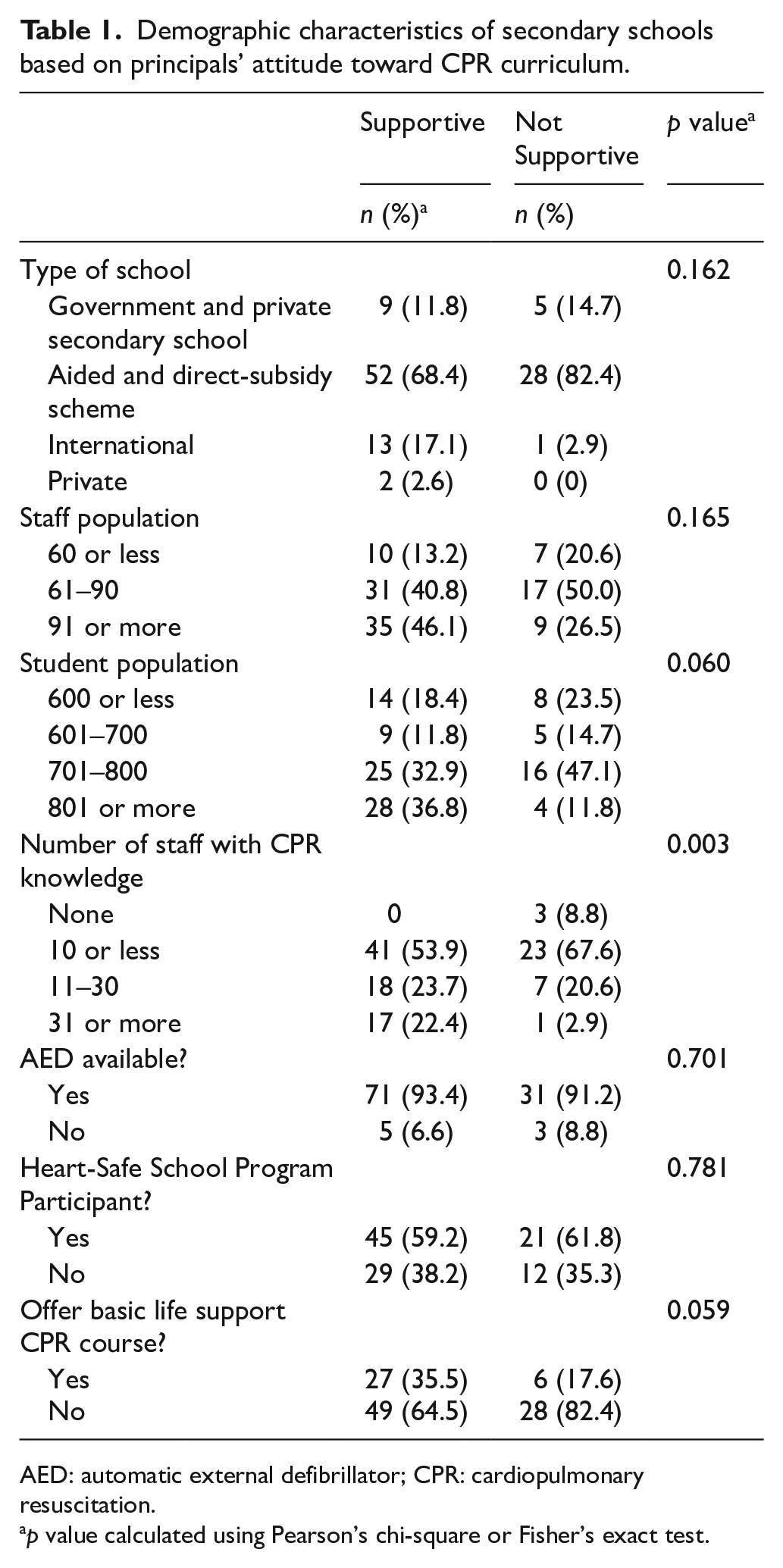
AED: automatic external defibrillator; CPR: cardiopulmonary resuscitation.
p value calculated using Pearson’s chi-square or Fisher’s exact test.
The average student population size per school was 796 (402,452 total secondary school students in Hong Kong divided by 506 schools), and the average number of teachers per school was 57 (28,863 total teachers divided by 506). 16 Table 2 shows that both local and international schools alike provide CPR training to students, with international schools being more likely to provide such training. In terms of availability of AEDs, 100.0% of government schools, 92.5% of aided and direct-subsidy scheme schools, and 87.5% of international schools had AEDs.
Schools with CPR training or an available AED.
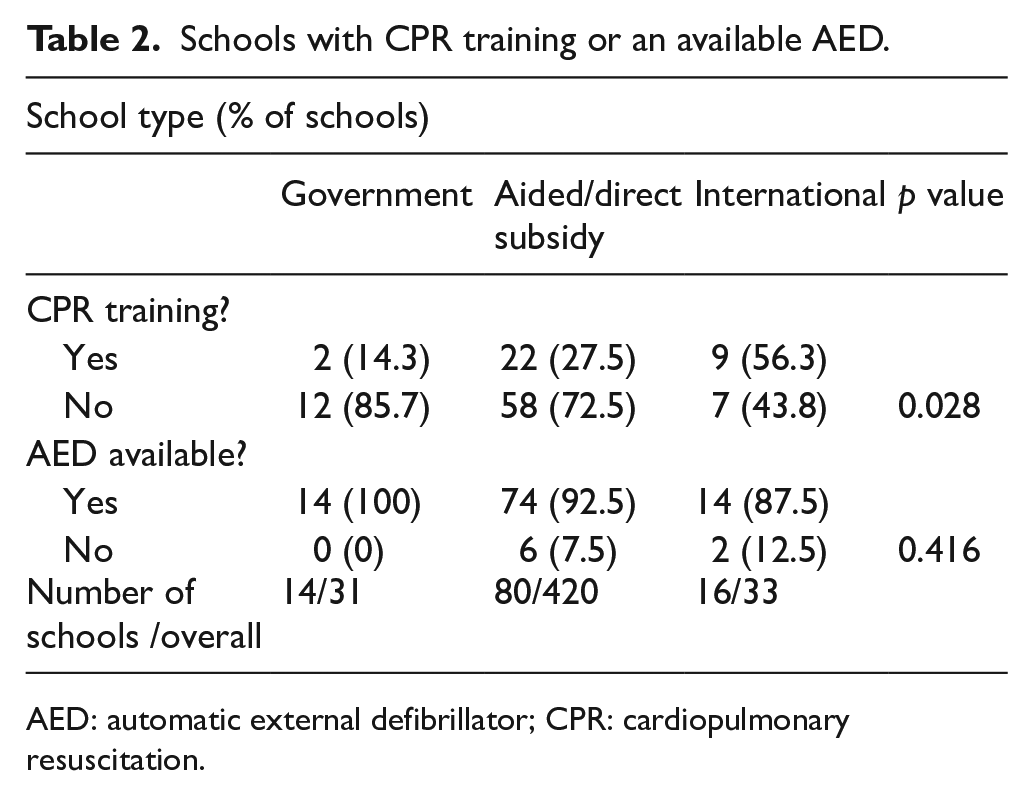
AED: automatic external defibrillator; CPR: cardiopulmonary resuscitation.
In total, the study identified 37 (33.6%) secondary schools that provide CPR training to their students. Information regarding course instructors, duration, content, and level of participation among students are summarized in Table 3. Most CPR students came from Secondary-4 and -5 grades (aged 15–17 years). Course durations were generally short, with 47% of responders reporting 0–5 h of coursework.
Characteristics of CPR training offered by Hong Kong secondary schools.
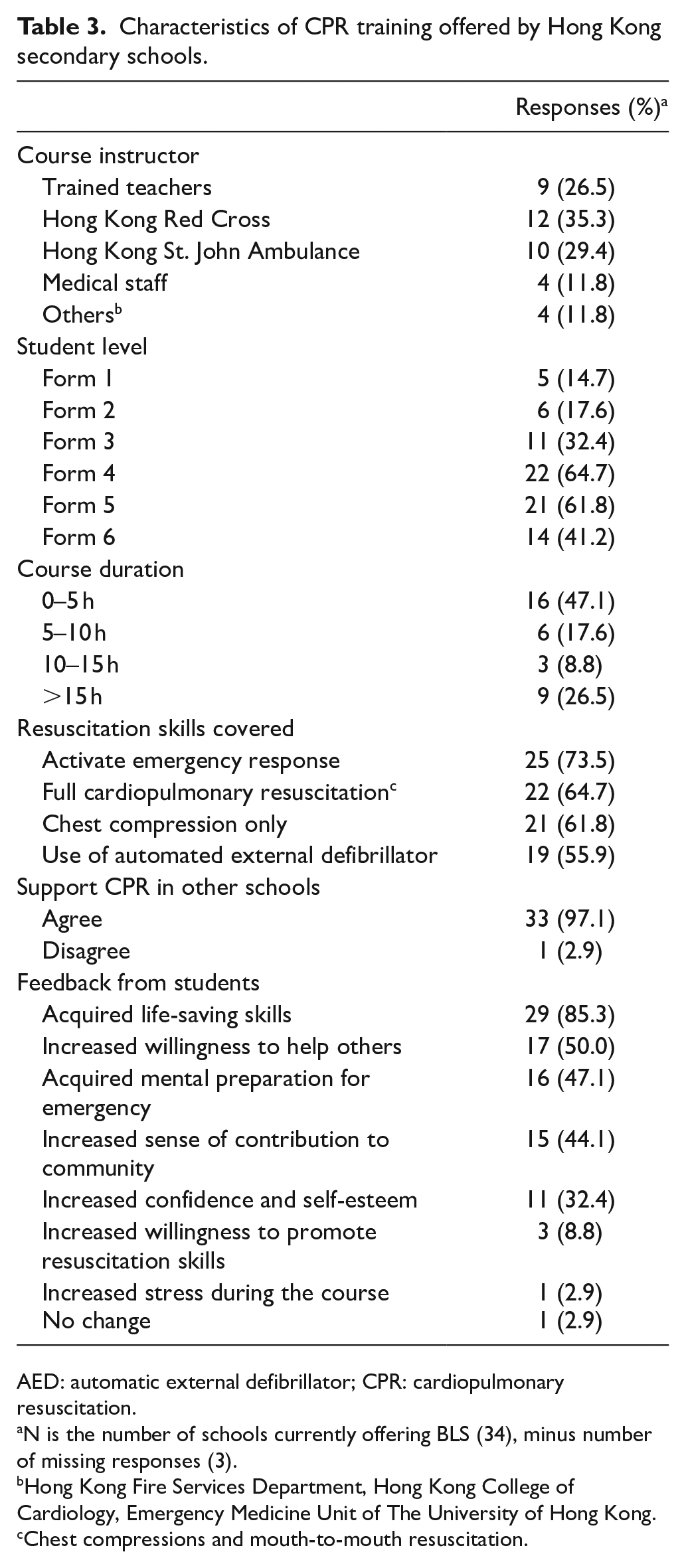
AED: automatic external defibrillator; CPR: cardiopulmonary resuscitation.
N is the number of schools currently offering BLS (34), minus number of missing responses (3).
Hong Kong Fire Services Department, Hong Kong College of Cardiology, Emergency Medicine Unit of The University of Hong Kong.
Chest compressions and mouth-to-mouth resuscitation.
The HKRC provided instructors for 35% of CPR classes in Hong Kong secondary schools surveyed, while 29% came from the Hong Kong St. John’s Ambulance service. In terms of course content, all taught CPR skills and 56% provided training on AED usage. Overall, 97% of schools supported CPR training in secondary schools. Students reportedly had positive feedback for the school CPR courses.
Despite our results showing overwhelming support for CPR teaching in secondary schools, more than 60% of schools in favor of the initiative did not offer any training to their students. The most cited reason for this was because CPR training has not been mandated as a compulsory component of the secondary school curriculum (31%).
In schools currently offering CPR training, perceived difficulties ranked by the number of responses are shown in Figure 2. “Time restrictions” and “challenges finding trainers” were the most common difficulties cited. In terms of strategies to boost support for implementing CPR training in secondary schools (Figure 3), the most frequently mentioned request was to increase funding resources (27.4%). This study found that all schools currently providing resuscitation training but not in fact supporting integration of CPR were unanimous in their support for increased resources.
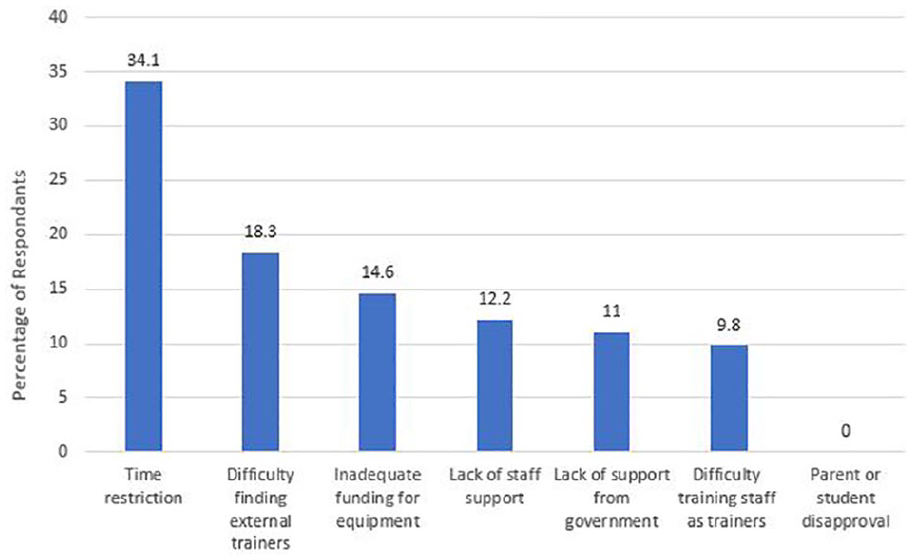
Perceived obstacles to implementation of CPR training.
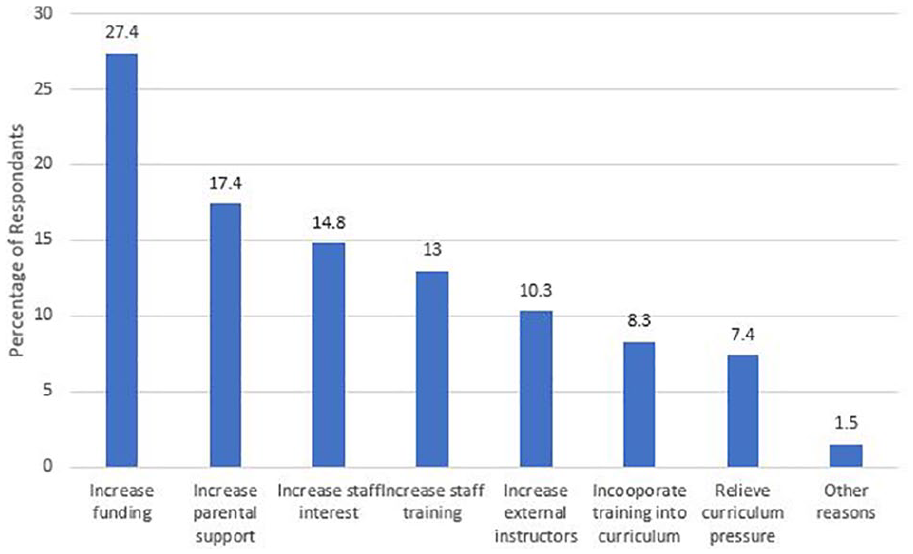
Measures to promote the provision of CPR training.
Discussion
This study found that approximately one-third of secondary schools in Hong Kong offer CPR training to staff and students. A large majority (69.1%) of secondary school principals were supportive of integrating CPR training into the school curriculum. Our results show that both local and international schools alike provided resuscitation training and garnered positive feedback from participating students. When asked about the challenges facing the initiation of CPR training in secondary schools, respondents cited financial barriers, similar to their overseas counterparts.17,18
First introduced in Norway in 1960, the implementation of school-based CPR training has taken many shapes and forms around the world. 19 A Danish cross-sectional study by Hansen et al. looked at school-based CPR training over the course of 8 years. 11 Hansen’s study summarized what was needed for schools to launch such an initiative: a course instructor with an appropriate CPR-proficiency level, access to training materials, a target student population, and course duration, content and organization. A scientific statement from the American Heart Association offered additional recommendations on the implementation of CPR/AED training which may add a framework for such secondary school implementations. 8
Although there is still no global consensus about the best educational strategy for resuscitation training, 20 the existing literature generally agrees that prior training at any interval increases the likelihood of bystander intervention and that skill retention decreases with time.8,20,21,22 It should be acknowledged that for most laypeople responding appropriately to a medical scenario that requires CPR or AED-use requires a complicated, anxiety-inducing decision-making process. Early, repeated training can help providers recognize the need for immediate intervention, thus increasing the likelihood of administering effective indirect (e.g. summoning help) or direct (BLS CPR) actions to help. 8 Determining the optimal frequency of refresher training without compromising motivation requires further longitudinal studies for school children.8,21
The question of whether external instructors or teachers from the involved schools are more effective in the provision of resuscitation training is controversial. This study showed that the availability of staff with resuscitation knowledge was a factor that significantly influences principals’ support for mandatory school-based CPR training. A recent German study found no significant difference between a group of students trained by school teachers compared with those trained by emergency physicians.21,23 The attitude of Hong Kong secondary school teachers toward teaching CPR is not known owing to the lack of local studies on the subject matter, although overseas studies have found that many teachers lack confidence when training their own students.23,17
One recent Hong Kong study reported a low level of enthusiasm with only 25% of teachers supporting CPR training in schools, and 32% willing to teach such a course. 14 Nearly 80% of local secondary school teachers expressed concerns over legal liability in the absence of “Good Samaritan” laws in Hong Kong. 14 However, this study only found 12% of secondary school principals considered the lack of staff support an obstacle to the provision of training. This apparent disconnect between principals and teachers is concerning that any initiatives pushed by principals may not have sufficient “buy-in” from teachers to succeed. Teachers, with their existing student-teacher rapport, are uniquely placed in the educational system to teach, monitor performance, and carry out standard assessments. 23 In-house teachers acting as CPR instructors could teach successive student groups. 22 Having teachers be part of any planning seems important to encourage full participation. Finally, “Good Samaritan” legislation should be considered for Hong Kong to ease fears of liability.
We did find a puzzle in the perceived obstacles to implementing CPR training in Hong Kong secondary schools. The most significant cited obstacle was time restrictions (34.1%), but more school principals suggested increasing funding (27.4%) rather than a curriculum reprieve (7.4%). Perhaps increasing funding was perceived as a simpler and more practical way to boost support for CPR training than changing the existing curriculum? Further research will be needed to better elucidate this divergence.
This study has several limitations. In total, 21.7% (110/506) of Hong Kong secondary schools participated in this survey. Unfortunately, we were unable to obtain the characteristics of non-responders for analysis, but it is possible that non-respondents were likely not interested in incorporating CPR into school curricula. This introduced a primary response bias. There are also issues of representation within the study sample. The Hong Kong education system classifies schools as either international or local schools, with further subdivisions within the local category. In this study, government, aided and direct-subsidy schools were underrepresented and constituted only 19.8% (94/473) of all local secondary schools in Hong Kong. Meanwhile, approximately half (48.4%, 16/33) of all international schools in Hong Kong responded to our survey, which may have skewed overall prevalence and support for CPR teaching in school. Finally, while the expertise and opinions of school principals are invaluable, they may not be representative of other school staff opinions.
Conclusion
This is the first study of its kind to investigate the prevalence of CPR training among Hong Kong secondary schools. While just over 30% of respondents reported active CPR training programs, two-thirds of secondary schools still have no CPR training. Overcoming obstacles to more widespread CPR training will require concerted effort, including additional funding for CPR courses in secondary schools.
Supplemental Material
CPR_training_HK_schools_20200804_HKJEM_APPENDIX_DEIDENTIFIED – Supplemental material for Cardiopulmonary resuscitation training in secondary education: A prospective cross-sectional survey of 110 Hong Kong secondary schools
Supplemental material, CPR_training_HK_schools_20200804_HKJEM_APPENDIX_DEIDENTIFIED for Cardiopulmonary resuscitation training in secondary education: A prospective cross-sectional survey of 110 Hong Kong secondary schools by Vivian Wan Cheong Yim, Crystal Ming-Lai Ip, Axel Yuet Chung Siu, Ling Yan Leung, Kevin Kei Ching Hung, Colin Alexander Graham, Priscilla P Song and Joseph Harold Walline in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors thank all the secondary school principals who completed the surveys for this study, and Mr LEUNG Yiu Wah, Master Trainer for the Hong Kong Red Cross, for his constructive recommendations.
Author contributions
All the authors made substantial contribution to the concept or design of the work; acquisition, analysis, or interpretation of data; drafted the article or revised it critically for important intellectual content; and approved the version to be published. Each author participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The corresponding author (J.H.W.) and one of the co-authors (K.K.C.H.) are editors with the Hong Kong Journal of Emergency Medicine.
Availability of data and materials
Data are available from the corresponding author upon reasonable request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent,Ethical approval,and Human rights
The authors affirm that the study was approved by the ethical review board. The name and date approval granted by the ethical board are included in the manuscript. Written or verbal informed consent was obtained from each patient included in the study. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.