
Abstract
Background:
Differences between pre-hospital triage by an emergency medical technician and Simple Triage and Rapid Treatment triage (START) by emergency staffs often affect manpower management and aggravate the chaos condition of emergency room.
Objectives:
Under the assistance of instant messaging, the authors aimed to identify ways of improving triage differences between emergency medical technician triage grading and Simple Triage and Rapid Treatment triage grading by emergency staffs.
Methods:
Recorded photographs of all patients were reviewed by a smartphone. We categorized patients according to three triage conditions: group 1, accident scene on-site or instantaneous Simple Triage and Rapid Treatment triage by the emergency medical technician; group 2, triage under Simple Triage and Rapid Treatment grading by emergency staffs; group 3, re-triage with START grading using recorded photographs, Glasgow Coma Scale, and vital signs when these patients were arrived in emergency room. The Wilcoxon Signed-Rank test, Spearman rank correlations, and Kruskal–Wallis test are employed to test differences among the groups. We used risk estimates with odds ratios and the chi-square test to statistically analyze the differences in triage grading.
Results:
Statistical analysis found conflicting results among Wilcoxon Signed-Rank test, Spearman rank correlations, and Kruskal–Wallis test. The difference in triage grading between groups 2 and 1 was greater than that between groups 2 and 3 (odds ratio, 6.473; 95% confidence interval, 1.693–24.470; p-value < 0.05).
Conclusion:
Transferred photographs combined with Glasgow Coma Scale and vital signs can help us to understand the real situations of patients. With instant messaging applications, it is possible to make more precise pre-hospital or instantaneous triage.
Introduction
In the train accidents on Ali Mountain of Taiwan, patient transport is typically very time-consuming. There is often chaos in the emergency room (ER) when patients eventually reach hospital. We have established practice guidelines for emergency medical preparedness to deal with disaster victims following notification by the emergency medicine technician (EMT) and emergency operations center (EOC). Our system is similar to that of Japan’s helicopter emergency medical service system and central Disaster Medical Assistance Team, which controls communications, dispatch centers, and information management concerning patient transport after a disaster. During disaster accidents correct information gathering and unhindered communication are always challenging. 1 Besides, it is necessary to determine accurately the onsite conditions and implement optimal manpower arrangements.
In mass-casualty incidents, in which the number of patients exceeds the allowable medical capacity of hospitals, the designate hospitals have to take care of the casualties as much as possible under the finite man power. The appropriate triage and man power assignment should be essential to achieve this mission.2,3 However, other types of non-medical support, such as establishing command and control, safety, unimpeded communications, and collaboration with other agencies, are also important. 4 Assessment tools have been developed to offer a standardized method for evaluating hospital preparedness and response performance. 5
In this study, we found problems with medical manpower assignment, such as medical physicians, when caring for trauma patients following a high mountain train accident. We examined the medical records of such patients and identified notable differences between Simple Triage and Rapid Treatment (START) triage graded by an EMT of the accident scene and START triage assessment performed by emergency medicine staffs in emergency room. We aimed to determine whether image transmission using instant messaging applications (IM Apps) could improve the situation regarding differences in triage assessment.
The aim of this study is to identify the ways of improving triage differences between EMT instantaneous triage grading of the on-site accident scene and START triage grading by emergency staffs in emergency room under the assistance of instant messaging.
Methods
In this case control study, the participants were 44 victims of the Ali mountain train accident in 2011. One patient had been expired at accident scene and was sent to ER for legal certification. The study was approved by the Institutional Review Board (IRB) at St. Martin De Porres Hospital in Taiwan (IRB No: 18B-004). Photographs were taken from patients when they arrived in the emergency room. One senior staff – who is the assistant head nurse of emergency room and took in charge of the triage duty in the accident – reviewed the recorded photographs by means of a smartphone. The START triage guideline shows the red status is first and assigned as grade I, yellow or orange status is second and assigned as grade II, green status is third and assigned as grade III, and black status is last and assigned as grade 0. A total of 43 patients have undergone all three groups of triage conditions: group 1, accident scene on-site or instantaneous START triage by an EMT; group 2, START triage grading by emergency staffs after patients arrived in ER; and group 3, re-triage with START grading using recorded photographs, Glasgow Coma Scale (GCS), and vital signs when these patients were arrived in emergency room. For statistical analysis, we employed the Wilcoxon Signed-Rank test, Spearman rank correlations, and Kruskal–Wallis test, and assessed risk using the odds ratio and chi-square test. We used the Statistical Package for the Social Sciences (SPSS) for Windows (version 23, IBM corporation Armonk, New York, USA) to perform statistical analysis.
Results
In this trauma disaster, most of the train accident victims were older individuals: 22 (51.1%) patients were aged between 51 and 60 years and 9 (20.9%) patients aged between 61 and 70 years. The mean patient transfer time by the EMT was 78.5 min. Under faulted assignment, medical physicians were responsible for 17 (38.6%) cases, which were categorized as START grades 2 and 3 upon admittance to the emergency room. We noted the mean grading discrepancies between the different triage methods. The lowest was with group 1 (2.40 ± 0.760) and highest with group 2 (2.74 ± 0.492). In the Wilcoxon Signed-Rank test, we identified the differences between groups 1 and 2 as well as between groups 1 and 3: significant statistical differences were evident (p = 0.001, 0.005, respectively). However, no significant statistical difference was observed between groups 2 and 3 (p > 0.05), as seen in Table 1.
Wilcoxon signed ranks test between different triage conditions.
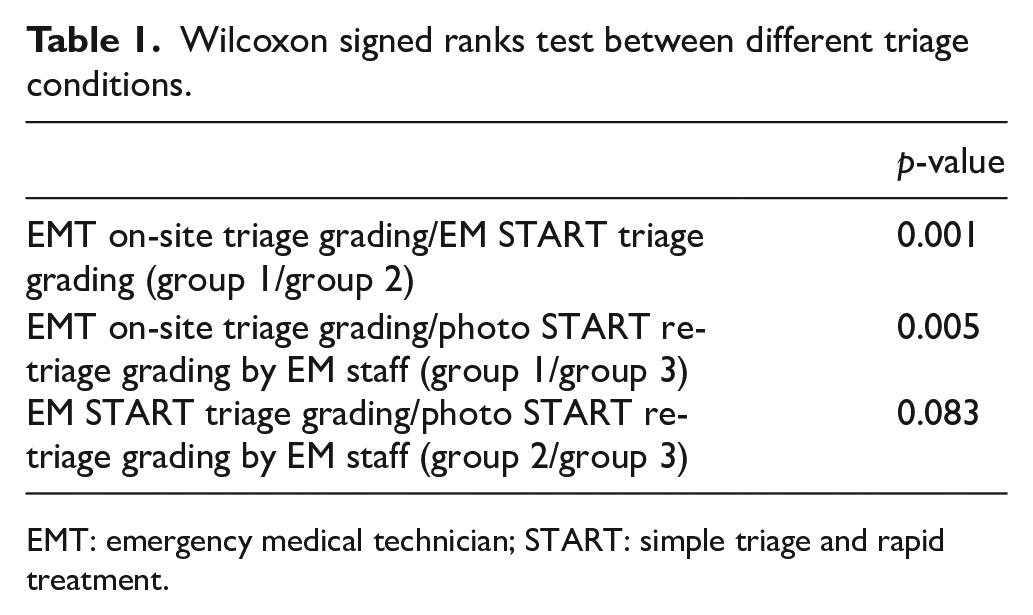
EMT: emergency medical technician; START: simple triage and rapid treatment.
In the Kruskal–Wallis test (Table 2), no statistically significant differences were found: p > 0.05; Spearman rank correlations demonstrated a good correlation between groups 2 and 1, groups 2 and 3, and groups 1 and 3 (p < 0.01; Table 2). We performed a risk estimate with odds ratios and the chi-square test to determine the differences with respect to triage grading changes under the different triage conditions (groups 1–3). The difference in triage grading change between groups 1 and 2 was greater than that between groups 2 and 3 (Table 3). The odds ratio for that difference was 6.473 (95% CI, 1.693–24.470; p < 0.05).
Kruskal–Wallis test and Spearman rank correlations for different triage conditions.
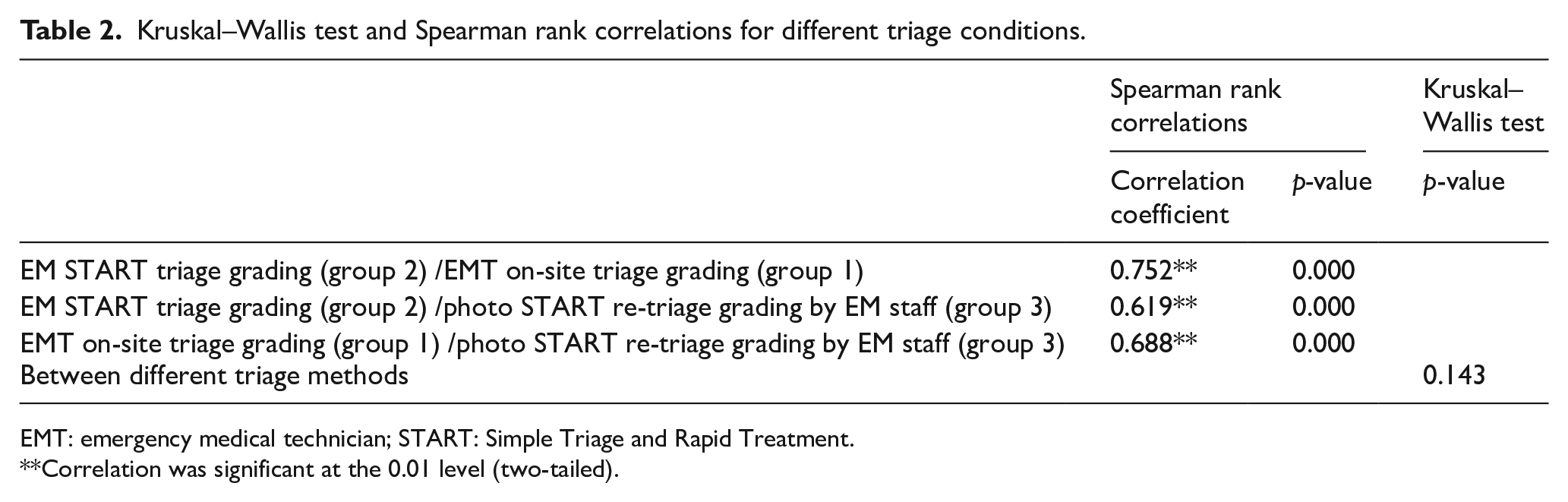
EMT: emergency medical technician; START: Simple Triage and Rapid Treatment.
Correlation was significant at the 0.01 level (two-tailed).
Triage grading differences compared with EM START triage grading (group 2) between EMT on-site or instantaneous triage grading (group 1) and photo START re-triage grading by EM staff (group 3).
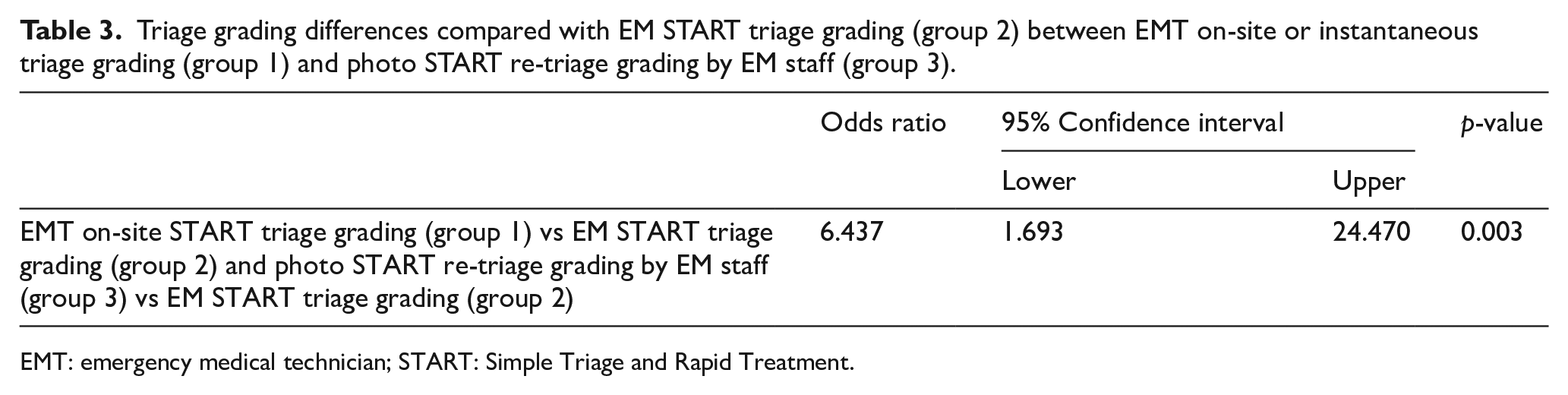
EMT: emergency medical technician; START: Simple Triage and Rapid Treatment.
Discussion
The first step toward improving the chaotic conditions that are common to disaster management is attempting to change manpower arrangements. The use of telemedicine in disaster situations has yet to become accepted. One study about the diagnostic accuracy of rapidly implemented telemedicine found that 31.5% of telemedicine patient encounters may not need additional orders to make a disposition decision. 6 However, another investigation about the use of physician tele-presence technology found no clinically significant differences in terms of time, triage scores, errors, and parent satisfaction; it concluded that using such technology can present an effective alternative to traditional nurse triage. 7
Following any disaster, appropriate management demands hospital preparedness and resource availability. 5 Reviewing previous experience in such cases, adjusting plans as appropriate, and conducting repeated staff training in implementing those plans could enhance the response speed and coordination. 8 To cope with disaster emergencies, we have introduced emergency manpower arrangements based on the advice of our EMT and EOC at our institution. However, despite such steps, the conditions in the emergency room are still chaotic. It is necessary to improve pre-hospital triage differences and make the EMT onsite or instantaneous triage more reliable.
With the Kruskal–Wallis test, no statistically significant difference was evident between the triage methods; the Spearman rank correlations analysis showed that the triage grading between triage methods. However, the impact on the emergency room and inappropriate arrangement of man power were evident. It could be due to the changes in the vital signs over time after prolonged transfer. With the Wilcoxon Signed-Rank test, we observed no significant difference between groups 2 and 3; however, there were clear differences between groups 1 and 2 and between groups 1 and 3. At our institution, previously used communication methods among disaster personnel were insufficient for current disaster manpower management. The pre-hospital triage by the EMT was unreliable in disaster conditions, and other methods should be developed to deal with that.
Instant messaging technology offers the possibility of improving triage differences between accident scene on-site or instantaneous START triage grading by an EMT and triage under START grading by emergency staff. It could help decrease manpower assignment problems. We questioned whether triage using photographic transmission with IM Apps could be useful and reliable. In this regard, we undertook a further analysis to determine the difference in triage grading between groups 1 and 2 and between groups 2 and 3. We found the odds ratio to be 6.473 and p-value = 0.003. The difference between the triage changes was more conspicuous between groups 1 and 2 than between groups 2 and 3.
With regard to disaster management, different kinds of multidisciplinary management should be examined in terms of compatibility through joint planning, training, and exercises. 4 The Disaster Medical Assistance Team of Taiwan provides front-line primary medical work that can quickly response to disasters, support medical work in disaster areas, waiting for more medical support and help to reduce the medical load in the disaster area. At one time, the first professionals dispatched to emergency areas used to be surgeons, anesthesiologists, intensivists, and senior nurses; in subsequent phases of the disaster response, their onsite members would be adjusted according to the changing needs of victims. From the experience of the Foreign Medical Team of disaster, the demand in medical salvage could change. A response in which the provided assistance is both appropriate to the expected epidemiological profile of the disaster and health profile of the affected community as well as being consistent with the actual health care required by the affected community. 9 However, we believe that in critical patient management, appropriate pre-hospital triage could allow a preliminary appraisal to be made concerning manpower management, such as the availability of surgeons and operating room capacity.
In this study, we aimed to determine the cause of the triage differences between the EMT and emergency medicine staff. We used images transmitted with IM Apps to minimize those differences. In case of our institution, we believe that additional training courses about pre-hospital triage are required. In this regard, a criteria-directed protocol in-hospital triage of trauma patients has been developed in Sweden. The protocol is succinct and has been found to be beneficial within the hospital trauma team. We intend to adopt this approach in training our EMT to conduct appropriate onsite triage. 10 A pre-hospital triage application could also offer benefits in standard training and duty processes.
Within 2 weeks following the 2010 Haiti earthquake, a transition from trauma to non-trauma cases was observed. 11 Transport problems are always the first main issue when dealing with mountain disasters; with time, the medical demands usually change. The EMT man can take real-time transmission of images at transportation and would be helpful in making manpower arrangements in disaster.
In disaster, the pre-hospital emergency medical system plays multiple functions such as taking care of patients on site, making proper medical triage, and transporting these patients for further health care. When treating disaster victims, the swift and expert actions of these skilled physicians can make a difference in medical intervention and improve the chaotic conditions of ER. Our study has some limitations. The long-term transportation of patients is not usual in Taiwan and mass-casualty incidents usually are unexpected and difficult to reproduce. Developing a common evaluation methodology in these incidents is extremely complex. 12 The purpose of this study was to find methods to improve triage differences utilized by EMT, which are one origin of ER chaos. Besides under the transmission function of IM App, the real-time report system can be set up to help us to monitor the changes of patients’ conditions.
Conclusion
When comparing with START triage grading by emergency staffs the results of START grading using transferred photographs, GCS, and vital signs have little differences than START grading of EMT man. Transferred photographs combined with GCS and vital signs can help us to understand the real situations of patients. Toward preventing chaotic conditions and handling large numbers of disaster victims, efficiently utilizing man power is necessary to implement disaster patient management. The triage made by the EMT differed from that made by the emergency medicine staff; the former appeared unreliable. The results of this study suggest that using IM Apps, it is possible to assess an accident scene and undertake accurate and instantaneous pre-hospital triage. Triage conducted using onsite or instantaneous images of patients in the context of pre-hospital telemedicine should be promoted. That would avoid ineffective man power use when dealing with disasters.
Footnotes
Acknowledgements
Author contributions
C.-H.C., T.-Y.W., H.-C.C., and C.-J.W. researched literature and conceived the study. J.-F.H. was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. C.-H.C. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.-H.C., T.-Y.W., H.-C.C., J.-F.H., and C.-J.W. are employees of St. Martin De Porres Hospital. The authors have not received grants from any institutions. There is no conflict of interest to be declared.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board (IRB) at St. Martin De Porres Hospital in Taiwan (IRB No: 18B-004).
Data statement
Due to the sensitive nature of the raw data included in this study, survey respondents were assured raw data would remain confidential and would not be shared. The research protocols used in this research were approved by the ethics committee of St. Martin De Porres Hospital in Taiwan (IRB No: 18B-004)