
Abstract
Objective:
To examine the association between the frequency of admission for pneumonia and the incidence of in-hospital cardiac arrest.
Methods:
We enrolled 1739 patients with in-hospital cardiac arrest and 6956 randomly selected age- and sex-matched control patients using a longitudinal claims sub-dataset from 1996 to 2011 for 1 million people randomly selected from the population covered by the Taiwan National Health Insurance program. The odds ratio of in-hospital cardiac arrest associated with the number of hospital admissions for pneumonia was calculated.
Results:
During the 15-year study period, the in-hospital cardiac arrest group had a higher frequency (28.4% vs 8.1%, p < 0.0001) of admission for pneumonia compared to the control group. The comorbidities of heart failure, chronic pulmonary disease, diabetes, renal failure, liver disease, lymphoma, alcohol abuse, and drug abuse were higher in the in-hospital cardiac arrest group than in the control group. In addition, the risk of in-hospital cardiac arrest was 3.37 for the patients admitted for pneumonia, and the risk of in-hospital cardiac arrest increased for patients with multiple admissions for pneumonia (once, 3.03; two times, 3.44; and three times, 4.42). In cross-analysis, the more admissions for pneumonia and the greater the number of comorbidities, the higher the risk of in-hospital cardiac arrest (odds ratio = 21.37, 95% confidence interval = 13.6–33.9 for patients with more than three admissions for pneumonia and more than three comorbidities).
Conclusion:
Higher admission frequency for pneumonia was associated with a higher risk of in-hospital cardiac arrest. Awareness of this risk factor may help clinicians provide early prevention or detection for patients with potential in-hospital cardiac arrest risks immediately after admission.
Introduction
Pneumonia has been a common cause of hospital admission for years and still has a significant mortality rate despite improvements in medical knowledge. A previous study found that the inpatient mortality of community acquired pneumonia (CAP) was 8%. 1 In addition, the short- to long-term effects of CAP persist after discharge. In a large, population-based cohort study, patients with CAP had a high risk of adverse events up to 10 years after their pneumonia, compared with a matched control group who had not experienced CAP. 2 Severity assessment tools for pneumonia, and CAP in particular, such as the CURB-65 criteria (confusion; urea > 7 mmol/L; respiratory rate > 30 breaths/min; systolic blood pressure < 90 mm Hg; age ⩾ 65 years) and the pneumonia severity index (PSI), have been developed to stratify the risk and to evaluate the requirement for hospital admission.3,4 However, it is common to over-estimate the severity or stratify admission inadequately in low-risk patients, 5 which may increase the risk of exposure to nosocomial infection or underestimating the amount of care needed.
Over 200,000 adult in-hospital cardiac arrest (IHCA) events occur in the United States annually. 6 One retrospective cohort study in Taiwan found an IHCA incidence rate of 3.25 per 1000 admissions. 7 The outcome for patients with IHCA is poor with a survival discharge rate of 15%–20%.8,9 Several factors may be related to the incidence of IHCA, including pre-arrest vital signs,10–12 race, 13 and variation between hospitals. 14 According to a prospective observational study of IHCA patients, pulmonary problems secondary to cardiac disease were the leading causes for admission, and hypoxia was the second major cause underlying IHCA, with the most common being myocardial infarction. 15 Accordingly, it is expected that the frequency of pneumonia admission may be an exacerbating factor of IHCA. The purpose of this study was to examine the association between the frequency of admission with diagnosis of pneumonia and IHCA using a population-based, case–control study.
Methods
Data source
We used a sub-dataset, established by the National Health Research Institutes, containing longitudinal claims data from 1996 to 2011 for 1 million people randomly selected from the population covered by the Taiwan National Health Insurance (NHI) program. The Taiwan NHI program covers 99.6% of the entire population in Taiwan and 93% of medical institutions are NHI-contracted (https://www.nhi.gov.tw/Content_List.aspx?n=5DF0FC79FE624C8A&topn=23C660CAACAA159D). Information of all registration and medical care data for each subject can be linked through a scrambled patient identification number to ensure personal privacy. The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) was used to identify diagnoses of diseases. A disease diagnosis without valid supporting clinical findings may be considered a medical fraud by NHI with a penalty of 100-fold of the payment claimed by the treating physician or hospital.
Study subjects
As shown in Figure 1, 2385 IHCA (ICD9 codes: 427.5, 798, 799.1) inpatients from 2000 to 2011 were identified. Patients were excluded from this study as follows: (1) concurrent onset of acute myocardial infarction (AMI), (2) IHCA records at the emergency room within the 3 days before admission, (3) aged under 18, or (4) withdrawal from the insurance program before the index date. In total, 1739 inpatients were included in this study. The date of the IHCA diagnosis was considered the index date. The comparison group was randomly selected from people who had never been admitted for IHCA, frequency matched by age (exact year) and sex based on a 1:4 case–control ratio. The number of admissions for pneumonia (ICD9 codes: 115.05, 115.15, 115.95, 116, 322, 517.1, 551, 480, 481, 482, 483, 484, 485, 486, 487.0, 730, 770.0, V03.82, V06.6) within 5 years before the index date was calculated. Comorbidities including congestive heart failure (ICD9 codes: 398.91, 402.11, 402.91, 404.11, 404.13, 404.91, 404.93, 428), chronic pulmonary disease (ICD9 codes: 490-492, 493.0-493.2, 494-505, 493.90, 493.91, 506.4), diabetes (ICD9 code: 250), renal failure (ICD9 codes: 403.11, 403.91, 404.12, 404.92, 585, 586, V42.0, V45.1, V56.0, V56.8), liver disease (ICD9 codes: 070.32, 070.33, 070.54, 456.0, 456.1, 456.20, 456.21, 571.0, 571.2, 571.3, 571.5, 571.6, 571.8, 571.9, 572.3, 572.8, V42.7, 571.40-571.49), lymphoma (ICD9 codes: 200.00-202.38, 202.50-203.01, 203.8-203.81, 196.0-199.1, 140.0-172.9, 174.0-175.9, 179-195.8, 238.6, 273.3, V10.71, V10.72, V10.79), alcohol abuse (ICD9 codes: 291.1, 291.2, 291.5, 291.8, 291.9, 303.90-303.93, 305.00-305.03, V11.3), and drug abuse (ICD9 codes: 292.0, 292.9, 300.4, 301.12, 309.0, 309.1, 311, 292.82-292.89, 304.00-304.93, 305.20-305.93, 295.00-298.9, 299.10-299.11) before the index date were also identified.
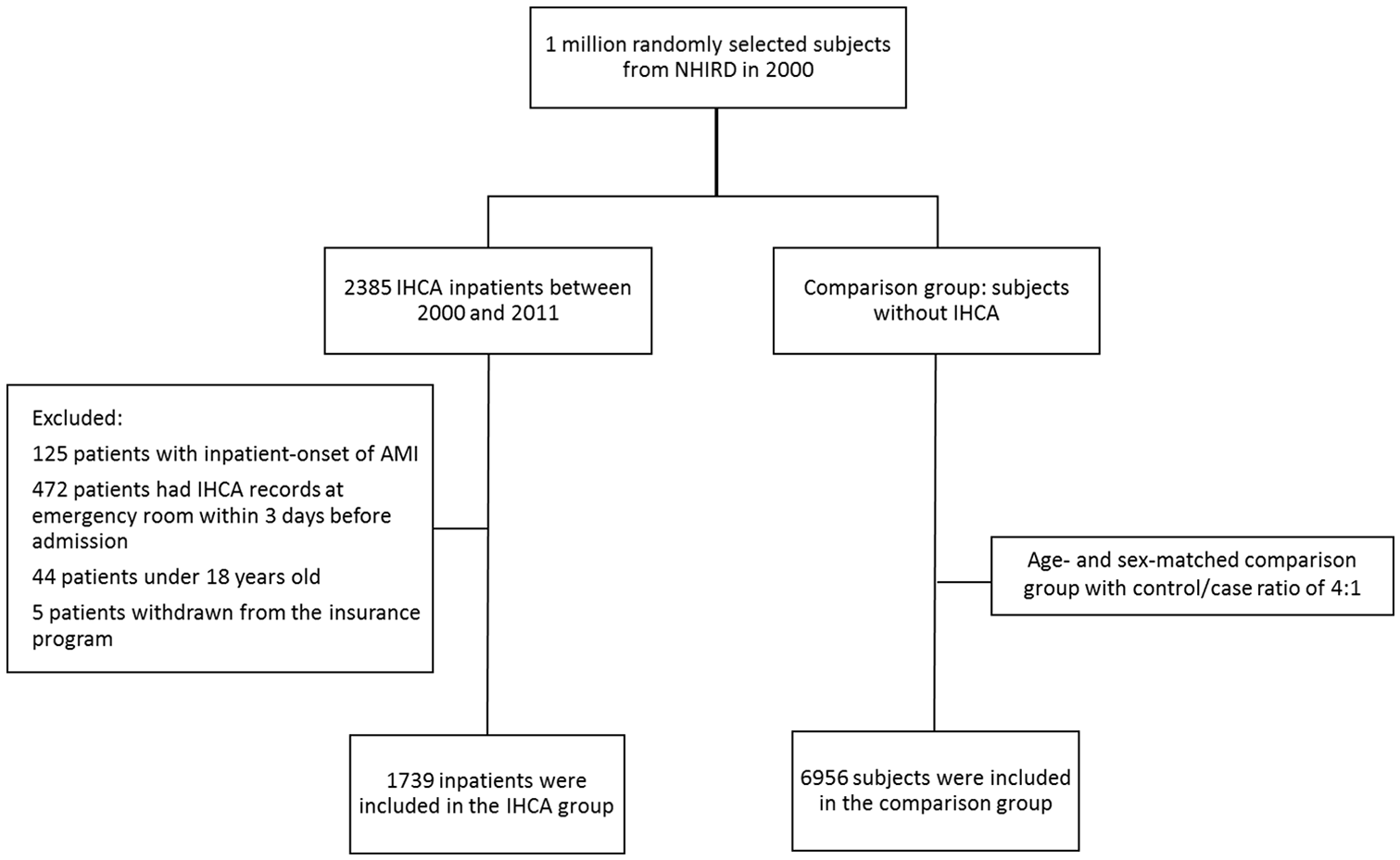
Patient inclusion/exclusion criteria. In total, 1739 patients with IHCA and 6956 randomly selected age- and sex-matched control patients were enrolled.
Statistical analysis
The differences in characteristics between the IHCA and non-IHCA groups were examined by chi-square tests, except for the mean age, which was evaluated by the Wilcoxon rank sum test. The risk of IHCA associated with the number of admissions for pneumonia by age was estimated using logistic regression, as was the risk of IHCA by the number of admissions for pneumonia associated with the number of comorbidities. All statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Carey, NC, USA). A two-tailed p value below 0.05 was considered significant.
Results
Table 1 shows the patient characteristics included the two study groups. The study consisted of 1739 inpatients in the IHCA group and 6956 matched controls. In total, 42.8% were female and the mean age was 69.5 years (SD ± 16.7). The IHCA group had a higher rate (28.4% vs 8.2%, p < 0.0001) of admission for pneumonia within 5 years. The IHCA group had more comorbidities than the control group (Table 1).
Characteristics of study patients.
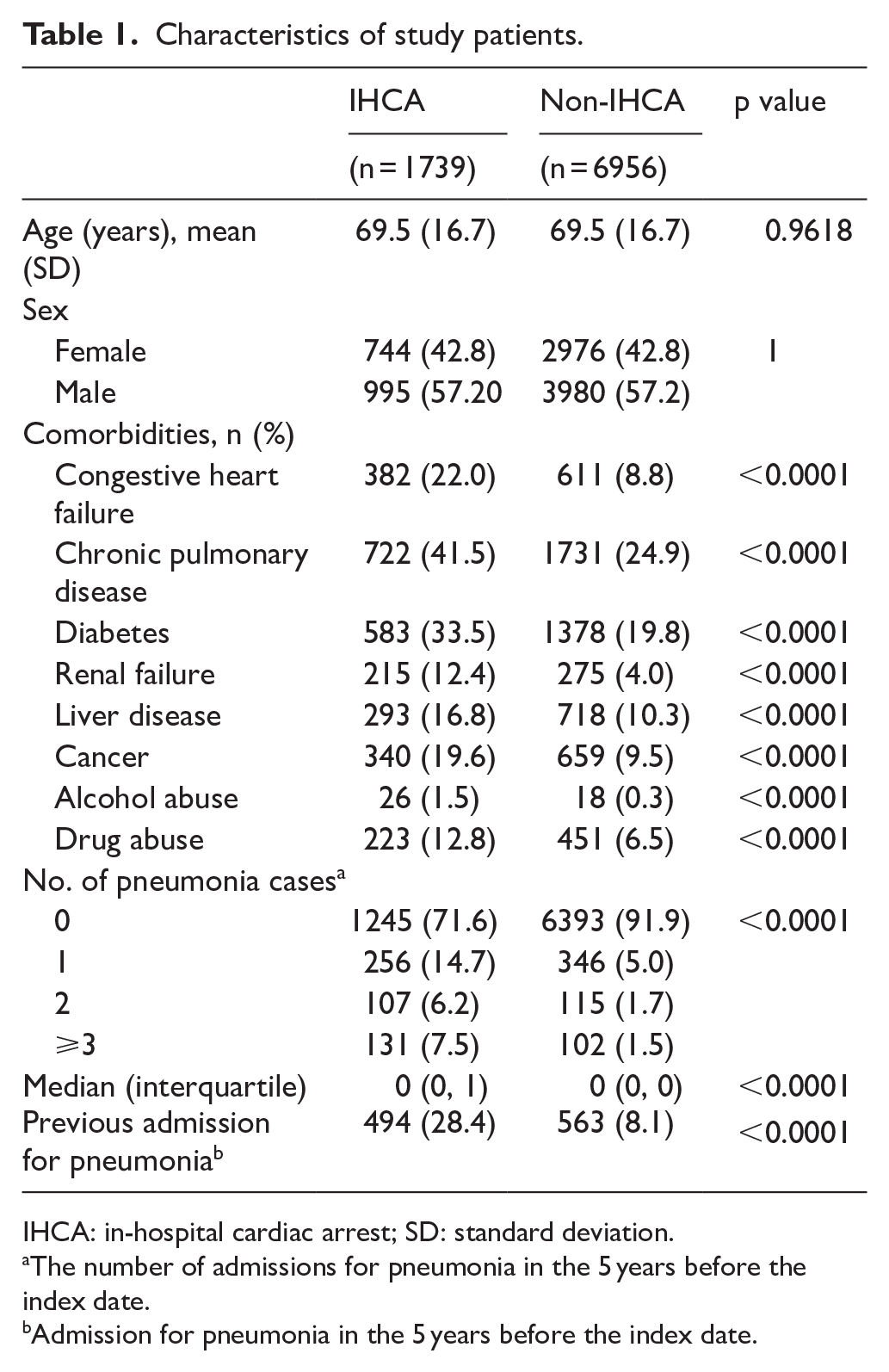
IHCA: in-hospital cardiac arrest; SD: standard deviation.
The number of admissions for pneumonia in the 5 years before the index date.
Admission for pneumonia in the 5 years before the index date.
The relative risk of IHCA was 3.37 for patients admitted for pneumonia compared to patients who never admitted for pneumonia within 5 years before the index date, and there was an increasing risk of IHCA for patients with multiple hospital admissions for pneumonia (once, 3.03; two times, 3.44; and three times, 4.42; Table 2). Moreover, the patient’s age was a significant risk factor for poor prognosis of pneumonia. 2 – 4 The association between pneumonia and IHCA was also evaluated by age. The odds ratio (OR) increased with the number of admissions for pneumonia within 5 years before the index date to 20.53 (95% confidence interval (CI) = 5.7–73.5) for patients under the age of 65 and to 3.6 (95% CI = 2.7–4.9) for patients over 65 years (Table 2).
Adjusted odds ratios of IHCA by age and association with pneumonia.
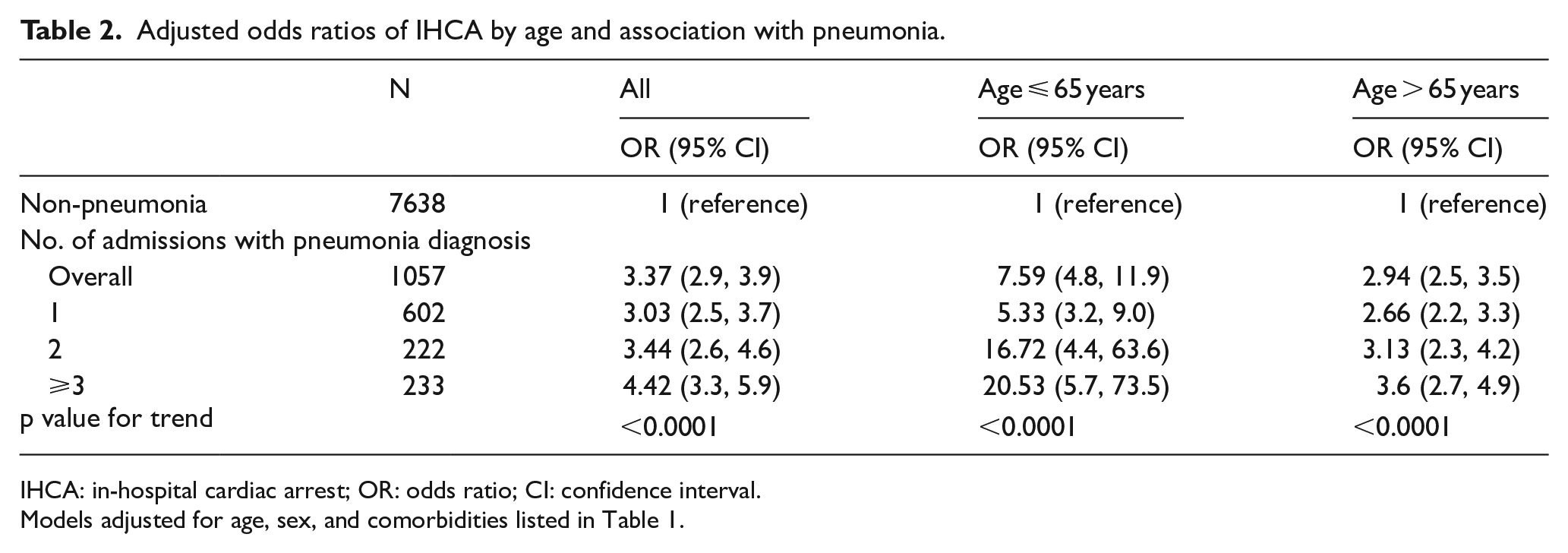
IHCA: in-hospital cardiac arrest; OR: odds ratio; CI: confidence interval.
Models adjusted for age, sex, and comorbidities listed in Table 1.
Furthermore, we combined the number of admissions for pneumonia within 5 years before the index date and the number of comorbidities and stratified into 16 levels to estimate the risk of IHCA among the different levels. There was a significantly higher risk in each level compared to subjects without admissions for pneumonia and with no comorbidities (Table 3). The more admissions for pneumonia and the greater the number of comorbidities, the higher the risk of IHCA (OR = 21.37, 95% CI = 13.6–33.9 for patients with more than three admissions for pneumonia and more than three comorbidities).
Adjusted odds ratios of IHCA by the number of admissions for pneumonia in association with the number of comorbidities.
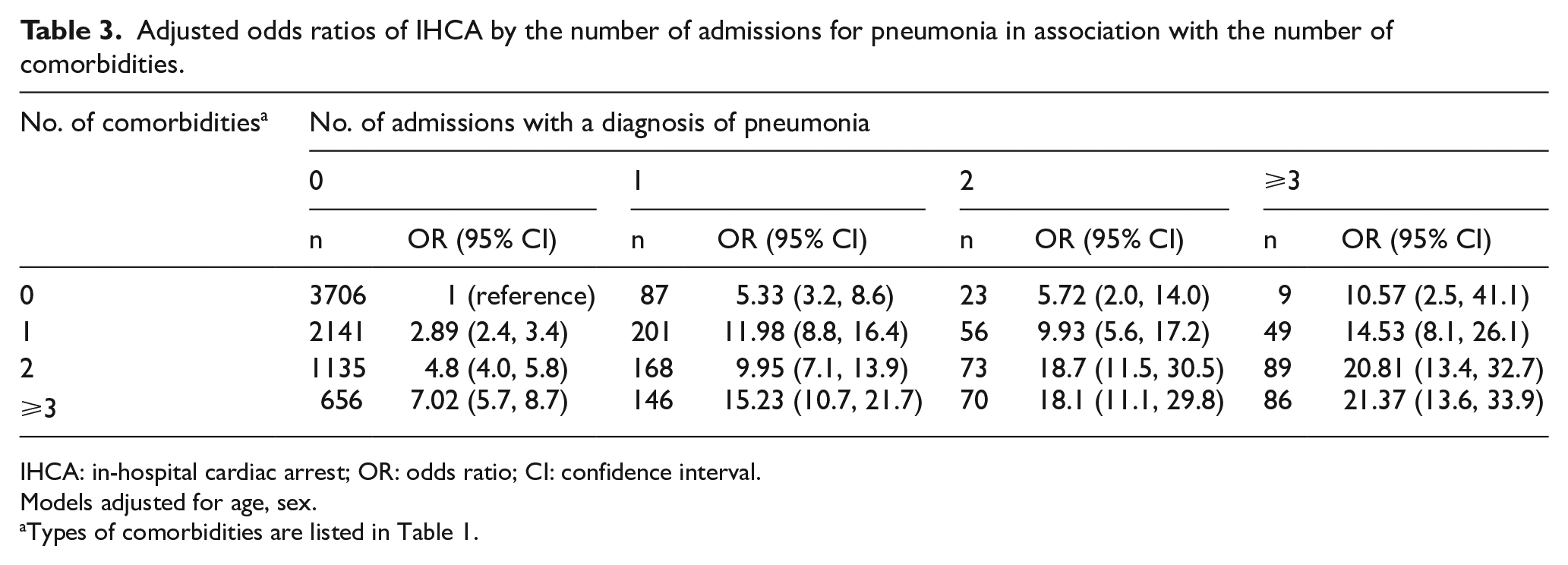
IHCA: in-hospital cardiac arrest; OR: odds ratio; CI: confidence interval.
Models adjusted for age, sex.
Types of comorbidities are listed in Table 1.
Figure 2 shows the duration between the last admission for pneumonia before an IHCA event among patients with a history of pneumonia in the IHCA group (n = 494). Approximately 30% of the patients had an IHCA within 1 month after admission for pneumonia (n = 494). Approximately 57% of the patients had an IHCA within 6 months after admission for pneumonia (n = 284). There was no significant difference in age (76.1 vs 73.6, p = 0.0488) for patients who experienced an IHCA more than 6 months after admission for pneumonia compared to patients who had an IHCA within 6 months.
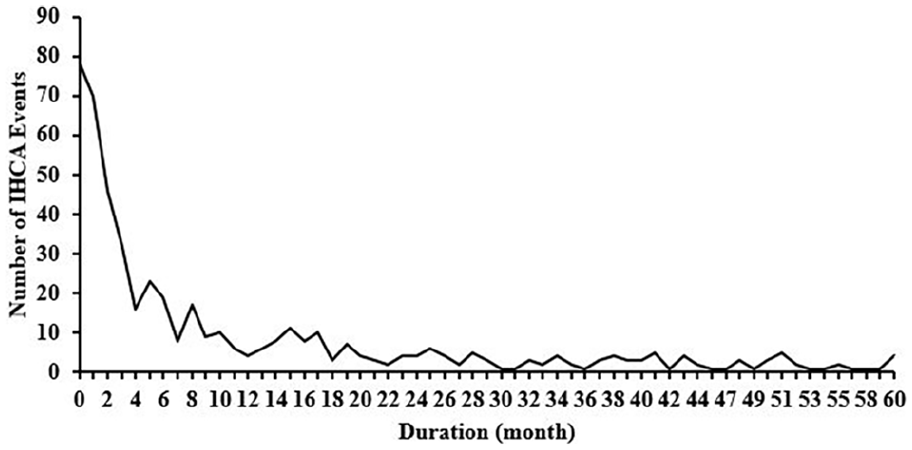
Distribution of the duration between the latest admission for pneumonia and an IHCA among patients with a history of pneumonia in the IHCA group (n = 494).
Discussion
The main finding in this study is that increased frequency of admission for pneumonia is associated with IHCA incidence. Although many factors affect the incidence of IHCA, most of them were discussed about the warning sign in hospitalization. The increased incidence of IHCA associated with increased frequency of admission for pneumonia should put hospital staff on alert at the beginning of hospitalization. The IHCA group revealed a higher frequency of admission for pneumonia overall. Each comorbidity selected in this study showed meaningful proportions in the IHCA group, which indicates that we can successfully search for hidden high-risk patients having numerous pneumonia admissions by examining the frequency of hospitalization. This is important if our goal is the detection, prevention, or early treatment of IHCA.
The number of comorbidities had a significant impact in this study. The OR was higher in patients admitted for pneumonia and even higher still for patients admitted for pneumonia with more than three comorbidities. The most powerful implication of this finding is in the risk classification made at the time of the initial admission. A previous study showed that up to 80% of patients with IHCA show signs of significant physiological deterioration 24 or even 4 h prior to cardiac arrest. 11 Several assessment tools for predicting critical events were assessed and the most popular tool is the Modified Early Warning System (MEWS). However, the efficiency of the prediction ability is still doubtful. An increasing MEWS only occurred in 46.8% of patients and approximately half the patients were still in the low MEWS group 8 h prior to cardiac arrest. 16 Furthermore, recent data showed that the occurrence of adverse events in patients with pneumonia had no substantive improvement. 17 The finding of the associated risk between the frequency of pneumonia admission and comorbidity impacts may provide clinicians with another assessment tool to accompany the current warning system for a more accurate prediction. Moreover, a greater impact from admission for pneumonia was seen in non-elderly patients (⩽65 years old) as that there were even higher OR of IHCA for the non-elderly age group compared with patients over 65 years (7.59–2.94). This finding may be due to the elderly patients approaching the end of the average lifespan and it highlights the importance of the effect of comorbidities on non-elderly patients.
In the brief report from the Agency for Healthcare Research and Quality, patients residing in low-income communities had a higher rate of hospitalization, a longer length of stay, and lower average hospital costs compared with patients in higher income communities. 18 According to a retrospective cohort study, 19 the length of hospital stay impacts the etiology and variations in the timing of IHCA events. In our study, the higher rate of hospitalization was associated with the higher incidence of IHCA, which implied that the quality and efficiency of the hospital were linked with reducing IHCA. Research into the national registry indicated that there was a negative correlation between a hospital’s incidence rate and case-survival rate for cardiac arrest. 20 Therefore, the more the hospital is committed to reducing the incidence of IHCA, the lower the IHCA mortality.
To manage unstable inpatients on general wards, the in-hospital rapid response system was established to prevent further deterioration resulting in unexpected cardiac arrest or unplanned intensive care unit (ICU) transfers. The rapid response team (RRT) and medical emergency team (MET) were implemented to manage conditions that fit the warning score or codes. The implementation of the RRT system not only reduced hospital mortality but also reduced the incidence of cardiopulmonary arrests in adults. 21 Although the theory and ideal of the RRT system is established, the effectiveness of the RRT is still being discussed and assessed due to different measurement methods.22,23 In a comparative study, hospitals with a mature rapid response system had a better performance than similar hospitals where RRT had just been set up. 24 According to the results of this study, clinicians could receive some risk stratification data proactively at the beginning of a hospital course in addition to passively pending unstable warning signs. The additional information may result in more accurate predictions and could model a more effective rapid response system.
This study found that more than half of the patients experienced IHCA within 6 months after admission for pneumonia, while 30% of the IHCA occurred within 1 month. This finding can be clarified by a study that revealed the readmission rate of pneumonia equaled 20%. 25 A recent prospective cohort study indicated that an episode of CAP was associated with a higher risk of long-term adverse events compared with the general population. 2 According to the cross-analysis of this study, more admissions for pneumonia with a greater number of comorbidities implied a higher risk of IHCA. Clinicians should pay greater attention to patients who are readmitted within a short interval or who have frequent admissions.
Limitations
There are several limitations in the study. First, we included patients based on the diagnosis of pneumonia via the discharged ICD code. It is difficult to distinguish pneumonia classifications of CAP, hospital-associated pneumonia, or ventilator-acquired pneumonia. The differences among different etiologies of pneumonia were not elucidated. In addition, the definition of IHCA may not have been precise, because of the lack of recorded personal pre-established orders in the database. This makes it hard to differ patients with “Do Not Attempt Resuscitation” orders from expected or unexpected IHCA. Moreover, the patient’s clinical condition, laboratory data, images, and the severities of pneumonia are not available in the database, neither are the severities of the comorbidities. Finally, we excluded patients with inpatient-onset of AMI to preclude the interference of cardiogenic cardiac arrest; however, the causes of cardiac arrest still could not clearly be defined (arrhythmia, hypoxia, etc.).
Conclusion
There are significant correlations between the frequency of admission for pneumonia and IHCA, and the number of comorbidities significantly impacts the incidence. From these results, we can better determine the IHCA risk before a patient is hospitalized. An initial IHCA risk assessment accompanied by ongoing MEWS detection may make RRT more efficient by collecting information proactively. The next step is to further analyze major admission causes beyond pneumonia, summarized into a comprehensive pre-hospitalization IHCA risk stratification.
Research Data
Research_data_source – for Association between the frequency of admission for pneumonia and the incidence of in-hospital cardiac arrest: A population-based case–control study
Research_data_source for Association between the frequency of admission for pneumonia and the incidence of in-hospital cardiac arrest: A population-based case–control study by Yu-Rung Hsu, I-Ju Tsai, Wei-Kung Chen and Kuan-Ho Lin in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors acknowledge the Management Office for Health Data assistance in collecting data and facilitating the completion of this paper.
Authorship
Y-R.H.: 60% contribution, paper finishing, and writing; I-J.T.: 20% contribution, data analysis, and table completion; W-K.C.: 10% contribution, article research directions; K-H.L.: 10% contribution, synthesis, and paper submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported in part by Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW106-TDU-B-212-113004), China Medical University Hospital, Academia Sinica Taiwan Biobank Stroke Biosignature Project (BM10501010037), NRPB Stroke Clinical Trial Consortium (MOST 105-2325-B-039-003), Tseng-Lien Lin Foundation, Taichung, Taiwan, Taiwan Brain Disease Foundation, Taipei, Taiwan, and Katsuzo and Kiyo AoshimaMemorial Funds, Japan.
Availability of data and materials
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.