
Abstract
Introduction:
With increased life expectancy, the proportion of elderly trauma admissions has increased. Elderly patients frequently have underlying diseases necessitating anticoagulant/antiplatelet medication, which worsens coagulopathy. We ascertained the relationship between preinjury anticoagulants/antiplatelet medication use and transfusion requirements in patients older than 65 years.
Methods:
This retrospective study enrolled patients admitted to the trauma intensive care unit of Chungbuk National University Hospital during January 2016 to June 2019. Data on medication history, clinical features, and component transfusions were analyzed with the chi-square test, independent t-test, one-way analysis of variance, and analysis of covariance.
Results:
Overall, 142 and 324 (overall 466) patients did and did not receive anticoagulant/antiplatelet medication, respectively. Falls were more frequent (p < 0.001) in the medicated group (n = 36; 25.4% vs n = 25; 7.7%). Head and neck injuries were more frequent among patients in the medicated group (58.5% vs 46.6%, p = 0.02), and they had a lower Injury Severity Score (ISS; 18.2 vs 20.2, p = 0.03), with no difference in serum hemoglobin level and coagulation function. The non-medicated group received more red blood cell transfusions within 4 h of arrival (2.24 vs 1.42 units, p = 0.03). Post hoc analysis revealed differences in red blood cell transfusions within 4 h of arrival between the non-medicated and warfarin groups (2.24 vs 0.33 units). Patients with head and neck injuries received less red blood cells than patients with other injuries (head and neck 1.07; chest and abdomen 2.73; pelvic and extremity 3.34 units, p < 0.001). On linear regression analysis, the Injury Severity Score and Glasgow Coma Scale score influenced the transfusion volume. Multivariate analysis controlled for Injury Severity Score, Glasgow Coma Scale score, and main injury site showed no intergroup differences in transfusion requirements.
Conclusion:
Preinjury anticoagulant/antiplatelet medication use was not significantly associated with transfusion amounts in patients older than 65 years.
Introduction
According to Statistics Korea, there are approximately 7 million people older than 65 years, who account for 13.8% of the national population in 2017; it is estimated that this percentage is expected to increase to 46.5% by 2067. 1 This increase in life expectancy and the consequent increase in geriatric population are being commonly observed in developed countries.2,3 As the population ages, the elderly tend to be more active outdoors, with a resultant increase in the proportion of elderly admissions at trauma centers. 4
Outcomes of trauma treatment are affected by injury mechanism, energy of impact, and physical conditions. 5 The elderly, unfortunately, are more susceptible to trauma-related mortality than the younger population even with the same injury mechanisms owing to their impaired cardiovascular and physiological functions.6,7 Moreover, elderly patients suffer from a higher number of complications than do young people. 8 Up to 40% of trauma, mortality is attributed to hemorrhage, which necessitates early transfusion and aggressive resuscitation. 9 Mador et al. 10 reported that the geriatric trauma population is more likely to receive fresh frozen plasma (FFP) transfusion due to an increased risk of anemia, increased injury severity, and trauma coagulopathy in the elderly.
Trauma coagulopathy is mediated by hemorrhagic shock, hypothermia, tissue injury, underlying diseases, and medication use associated with pre-existing diseases.11,12 The elderly are more likely to be on anticoagulant or antiplatelet medications, which reportedly increase the risk of coagulopathy 13 and may affect the amount of transfusion required for resuscitation of trauma patients who sustain hemorrhages.
Several previous studies have reported differences in treatment outcomes with the preinjury use of anticoagulant or antiplatelet medications.14,15,16 Some studies have been conducted on blood transfusions wherein it has been reported that the use of an anticoagulant or antiplatelet agent increases the risk of massive transfusion,17,18 although studies related to changes in blood transfusion volumes are insufficient. Therefore, this study was conducted to identify whether preinjury anticoagulant or antiplatelet therapy is associated with the amount of transfusion required following trauma in patients older than 65 years.
Methods
Patients and data
This retrospective study was based on a review of data extracted from the medical records in the Korean Trauma Data Bank. We screened the records of 5736 patients who visited the trauma center of Chungbuk National Hospital between January 2016 and June 2019. After excluding patients who were not hospitalized or were younger than 65 years and excluding patients who were transferred to other hospital, we included 466 patients in this study (Appendix 1). Information on their mechanism of injury, the Injury Severity Score (ISS), major injury sites, and laboratory results was extracted and collated for analysis using Excel.
Blood investigations and transfusions
The patient’s initial and 24 h (sample drawn 24 h after admission) serum hemoglobin levels were examined to estimate blood loss. Similarly, the international normalized ratio (INR) and activated partial thromboplastin time (aPTT) at admission and 24 h later were used to determine coagulopathy. The amount of component transfusions (packed red cell (PRC), FFP, and platelet concentrate) was assessed within 4 h, for the next 20 h, and for the overall 24 h since arrival.
Definition
Injury severity was determined with the Injury Severity Score (ISS), and mental status was ascertained from the Glasgow Coma Scale (GCS) score. The medicated group comprised patients who were on any of the following drugs: warfarin, aspirin, clopidogrel, cilostazol, and non-vitamin K antagonist oral anticoagulants (NOACs). Patients who were not on any of the abovementioned drugs were grouped into the non-medicated group. The subgroup with coronary artery diseases included patients who were diagnosed with stable angina, unstable angina, or myocardial infarction, and the cerebrovascular disease subgroup included patients diagnosed with ischemic stroke. Slip down was defined as an injury when slipping or falling on the ground level (fall less than 2 m). Fall down was defined as the case where an injury occurred while falling to the ground from a position higher than the patient’s height (fall more than 2 m).
Statistical analysis
Statistical analysis was conducted in IBM SPSS Statistics V. 23.0 (IBM Corporation, Armonk, NY, USA). The patient’s age, ISS, GCS, laboratory results, and transfusion amounts were analyzed with the independent t-test. The normal distribution test was undertaken using skewness and the kurtosis standard suggested by West et al. 19 The patient’s age, injury mechanism, main injury sites, and clinical features were analyzed using the chi-square test. We used the independent t-test and one-way analysis of variance (ANOVA) to determine the factors that influence transfusion amount. Furthermore, Welch’s F test was performed without assuming homogeneity of variances, and Games–Howell’s post hoc analysis was used. Linear regression analysis was conducted to determine the effect of the patient’s age, ISS, and GCS score on blood transfusion volume. Moreover, an analysis of covariance (ANCOVA) was used for multivariate analysis to analyze the difference in transfusion volume according to the preinjury medication with regard to the influence of the ISS, GCS score, and main injury site. Statistical differences were significant when two-tailed p-values were less than 0.05.
Results
Of the 466 trauma patients older than 65 years who were admitted to the intensive care unit (ICU) of the trauma center at Chungbuk National Hospital, 142 patients were on preinjury medication (medicated group) whereas the other 324 were not on any of the listed medications (non-medicated group). In the medicated group, 72 patients were on aspirin, 25 on clopidogrel, nine on warfarin, 12 on NOACs, and 24 on aspirin with clopidogrel therapy (Appendix 1). The average age of the non-medicated and medicated group was 75.3 and 76.6 years, without any statistically significant difference. Table 1 shows a higher incidence of cardiovascular disease and cerebrovascular disease in the medicated group which was statistically significant (p = 0.01, p < 0.01, respectively). Moreover, we found a statistically significant difference in the injury mechanism between the two groups (p < 0.001). Injury due to slipping was significantly more frequent (p < 0.001) in the medicated group (25.4%, n = 36) than in the non-medicated group (7.7%, n = 25). Head and neck injuries were significantly more frequent (p = 0.02) in the medicated group (58.5%, n = 83) than in the non-medicated group (46.6%, n = 151).
Clinical data of trauma patients admitted to the ICU.
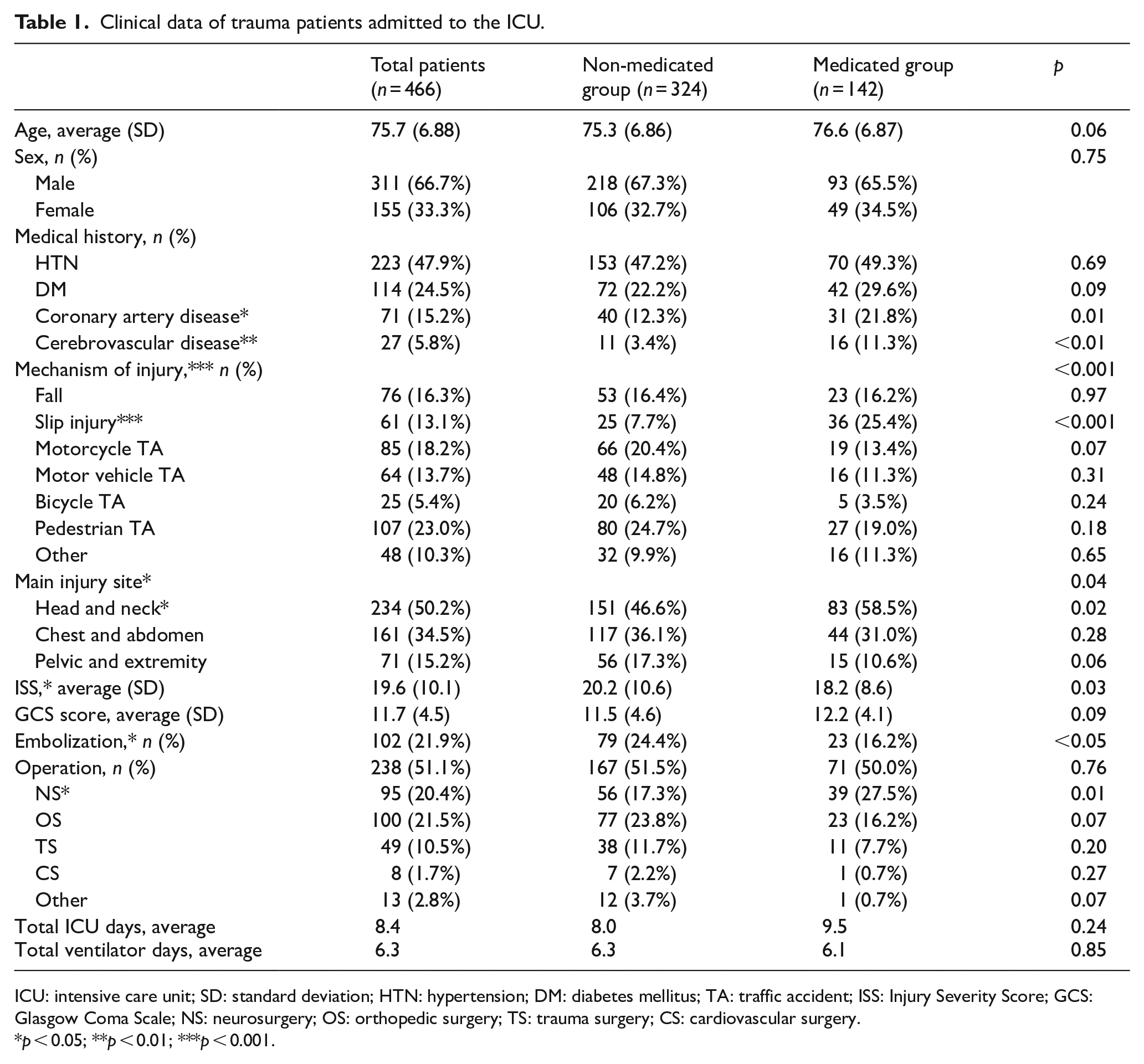
ICU: intensive care unit; SD: standard deviation; HTN: hypertension; DM: diabetes mellitus; TA: traffic accident; ISS: Injury Severity Score; GCS: Glasgow Coma Scale; NS: neurosurgery; OS: orthopedic surgery; TS: trauma surgery; CS: cardiovascular surgery.
p < 0.05; **p < 0.01; ***p < 0.001.
The average ISS of the entire study population (n = 466) was 19.6 (standard deviation (SD): 10.1) whereas the average ISS of the medicated group was 18.2 (SD: 8.63), which was significantly lower (p = 0.03) than the average ISS of 20.2 (SD: 10.6) for the non-medicated group. Although statistical significance of overall surgery was not established, the medicated group underwent more neurosurgeries (p = 0.01), whereas the non-medicated group received a greater number of endovascular embolizations (p < 0.5; Table 1).
There was no statistically significant difference in serum hemoglobin levels and coagulopathy between the two groups in the initial resuscitation phase (Appendix 2). One-way ANOVA was conducted to investigate the differences in blood test parameters according to the type of medication, and the results are shown in Table 2. Statistically significant differences were observed in the initial INR (Welch F = 5.811, p < 0.001) and the INR measured after 24 h (Welch F = 8.062, p < 0.001). In the Games–Howell post hoc analysis, the warfarin group showed higher INR values than the other groups did. During the first 4 h, the non-medicated group received significantly more (p = 0.03) PRC transfusion (average 2.24 units) than the medicated group (average 1.42 units). However, during the first 24 h, the non-medicated group received more PRC transfusions, but the difference was not statistically significant. With regard to other component transfusions, the non-medicated group received more transfusions but without statistically significant differences (Appendix 3). Moreover, as shown in Table 3, no statistically significant difference was observed in blood transfusion requirements between the drug subgroups. In Games–Howell post hoc analysis, the non-medicated group had a higher requirement than the warfarin group did for PRC transfusion (within 4 h, average of 2.24 vs 0.33 units; total units within 24 h, average of 3.47 vs 0.67 units) and a higher requirement than for the aspirin + clopidogrel group as well as the warfarin group for platelet concentrate transfusion within 4 h (mean, 0.45 vs 0 units), although these differences were not statistically significant.
Laboratory data stratified by preinjury medication group (one-way ANOVA and post hoc analysis).
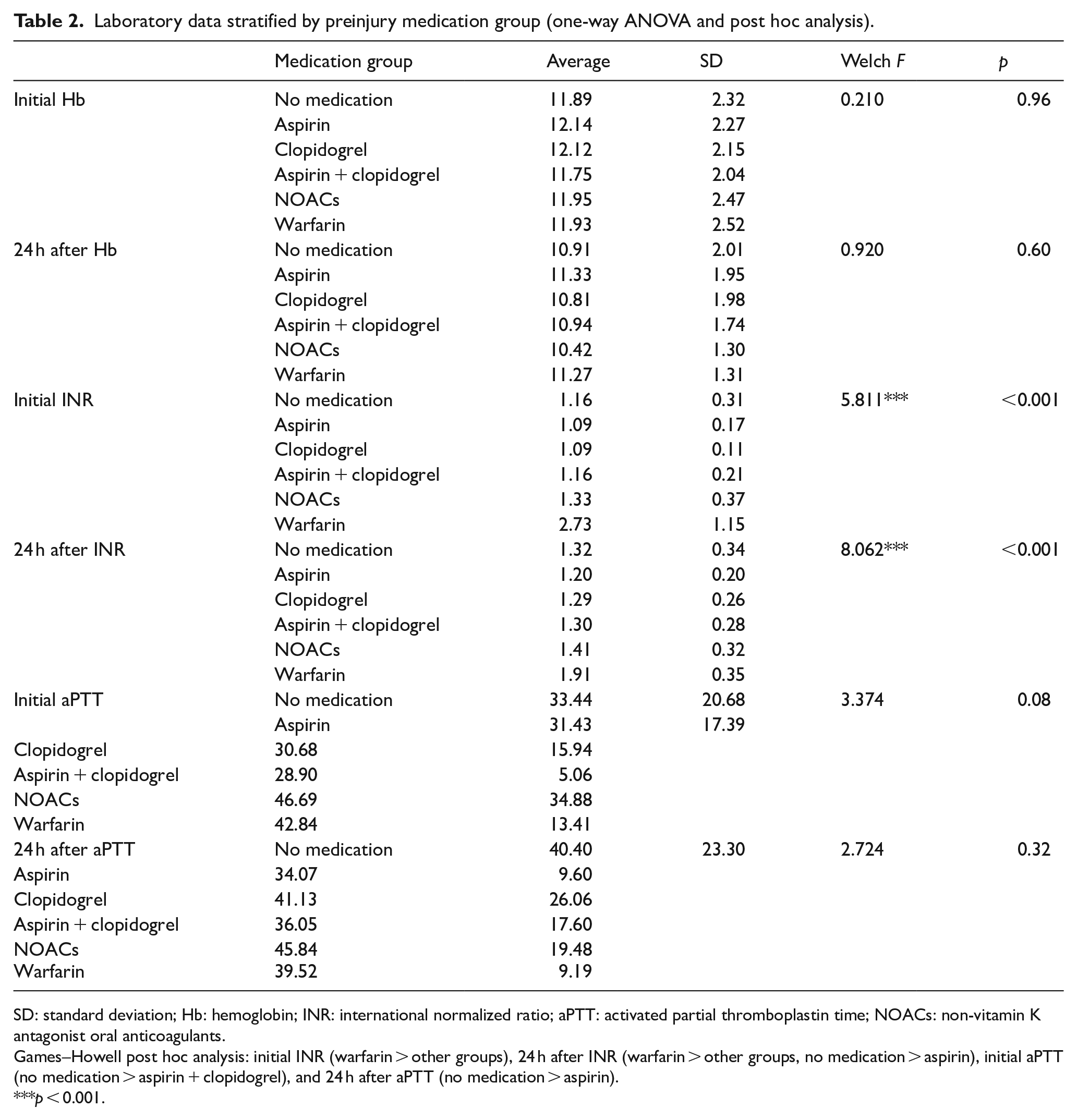
SD: standard deviation; Hb: hemoglobin; INR: international normalized ratio; aPTT: activated partial thromboplastin time; NOACs: non-vitamin K antagonist oral anticoagulants.
Games–Howell post hoc analysis: initial INR (warfarin > other groups), 24 h after INR (warfarin > other groups, no medication > aspirin), initial aPTT (no medication > aspirin + clopidogrel), and 24 h after aPTT (no medication > aspirin).
p < 0.001.
Transfusion data stratified by preinjury medication groups (one-way ANOVA and post hoc analysis).
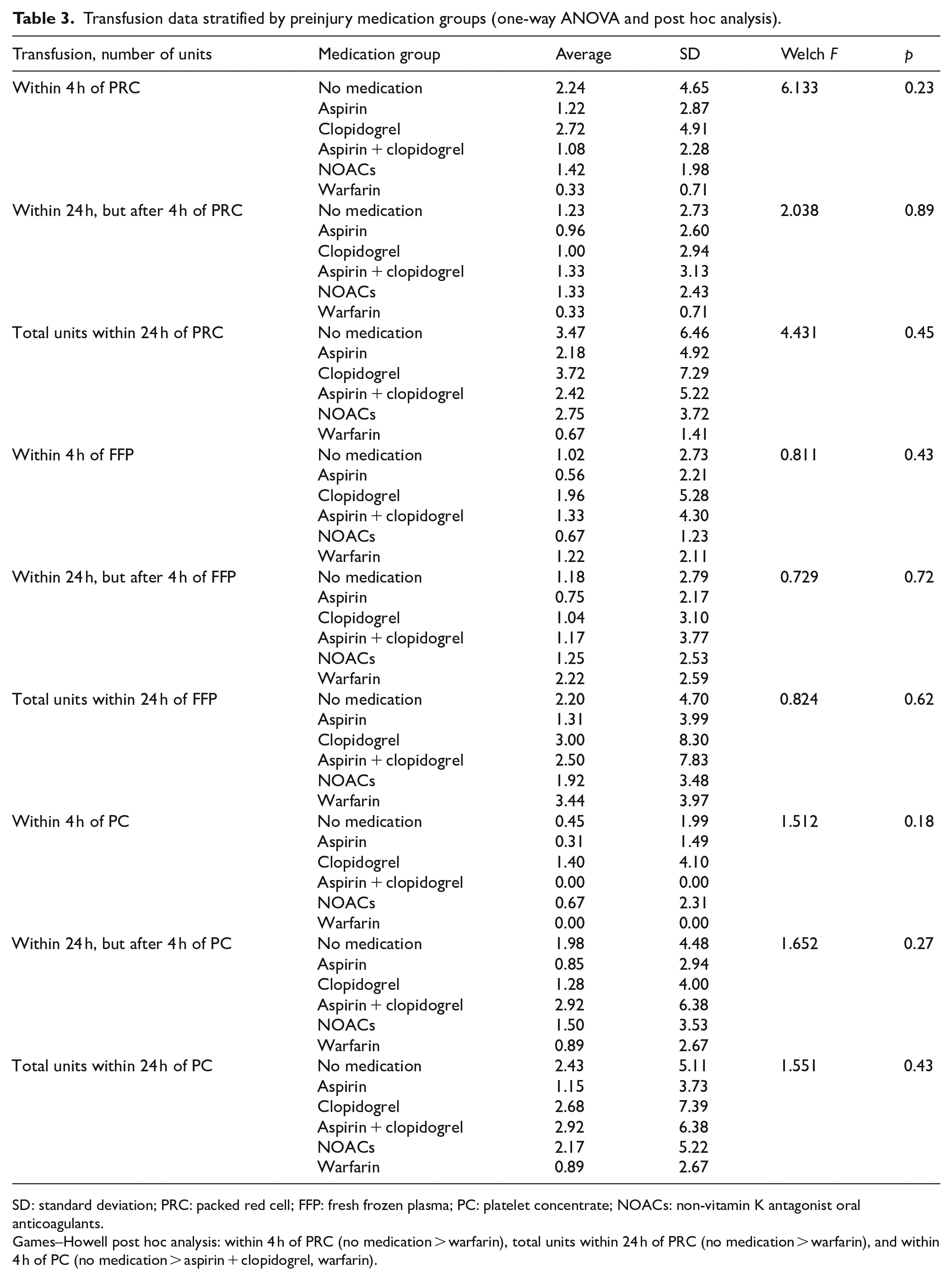
SD: standard deviation; PRC: packed red cell; FFP: fresh frozen plasma; PC: platelet concentrate; NOACs: non-vitamin K antagonist oral anticoagulants.
Games–Howell post hoc analysis: within 4 h of PRC (no medication > warfarin), total units within 24 h of PRC (no medication > warfarin), and within 4 h of PC (no medication > aspirin + clopidogrel, warfarin).
Table 4 shows the amount of transfusion stratified by main injury sites. Less PRC units were transfused to patients with head and neck injuries (1.86 units) compared with patients with chest and abdomen (4.09 units) or pelvis and extremity (5.28 units) injuries, and this difference was statistically significant (Welch F = 13.343, p < 0.001). Less FFP units were transfused to patients with head and neck injuries (1.50 units) compared with those with chest and abdomen (2.71 units) or pelvis and extremity (2.96 units) injuries, which was statistically significant (Welch F = 4.210, p = 0.02). However, there was no statistically significant difference in FFP transfusion requirements between the groups on post hoc analysis. More platelet units were transfused to the patients with pelvis and extremity injuries (1.04 units) than to those with injuries at the head and neck sites (Welch F = 2.025, p = 0.03) within the first 4 h, but the post hoc analysis result was not statistically significant. Furthermore, there was no statistically significant difference in the number of units transfused within the subsequent 20 h or the overall initial 24 h.
Transfusion data stratified by main injury site (one-way ANOVA and post hoc analysis).
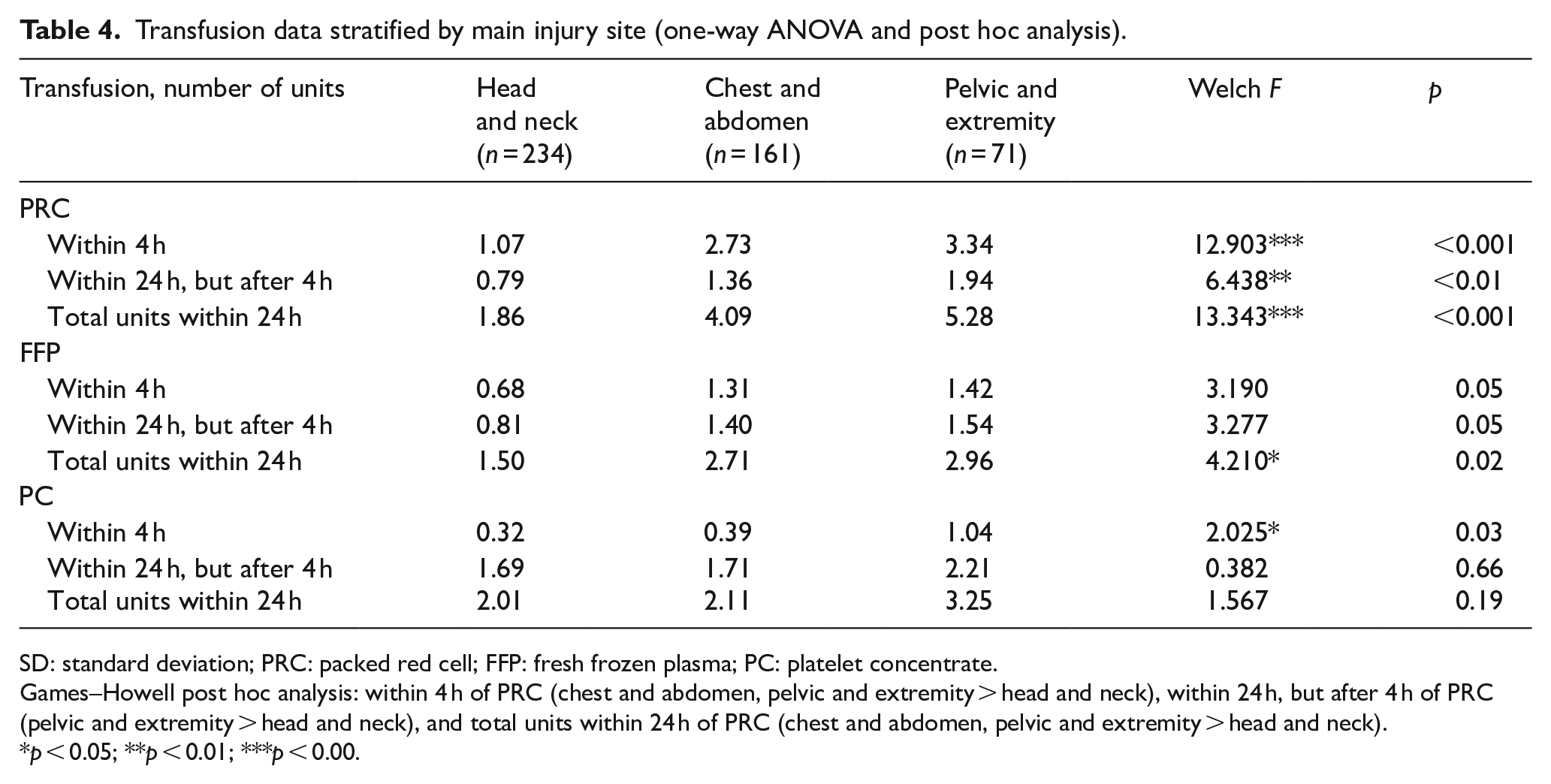
SD: standard deviation; PRC: packed red cell; FFP: fresh frozen plasma; PC: platelet concentrate.
Games–Howell post hoc analysis: within 4 h of PRC (chest and abdomen, pelvic and extremity > head and neck), within 24 h, but after 4 h of PRC (pelvic and extremity > head and neck), and total units within 24 h of PRC (chest and abdomen, pelvic and extremity > head and neck).
p < 0.05; **p < 0.01; ***p < 0.00.
Figure 1 presents a graph of the differences in transfusion amounts depending on main injury sites in the medicated and non-medicated groups. As shown in the graph for patients with head and neck injury, there was no increase in blood transfusion requirement in the preinjury medicated group for the PRC, FFP, and platelet units. Patients with chest and abdomen injury showed a higher number of transfusion units in the non-medicated group than in the preinjury medicated group for the PRC, FFP, and platelet transfusions; however, a statistically significant difference was observed only for platelet transfusion. Moreover, patients with pelvic and extremity injury showed fewer transfusions in the preinjury medicated group than in the non-medicated group, but a statistically significant difference was observed only for platelet transfusion.
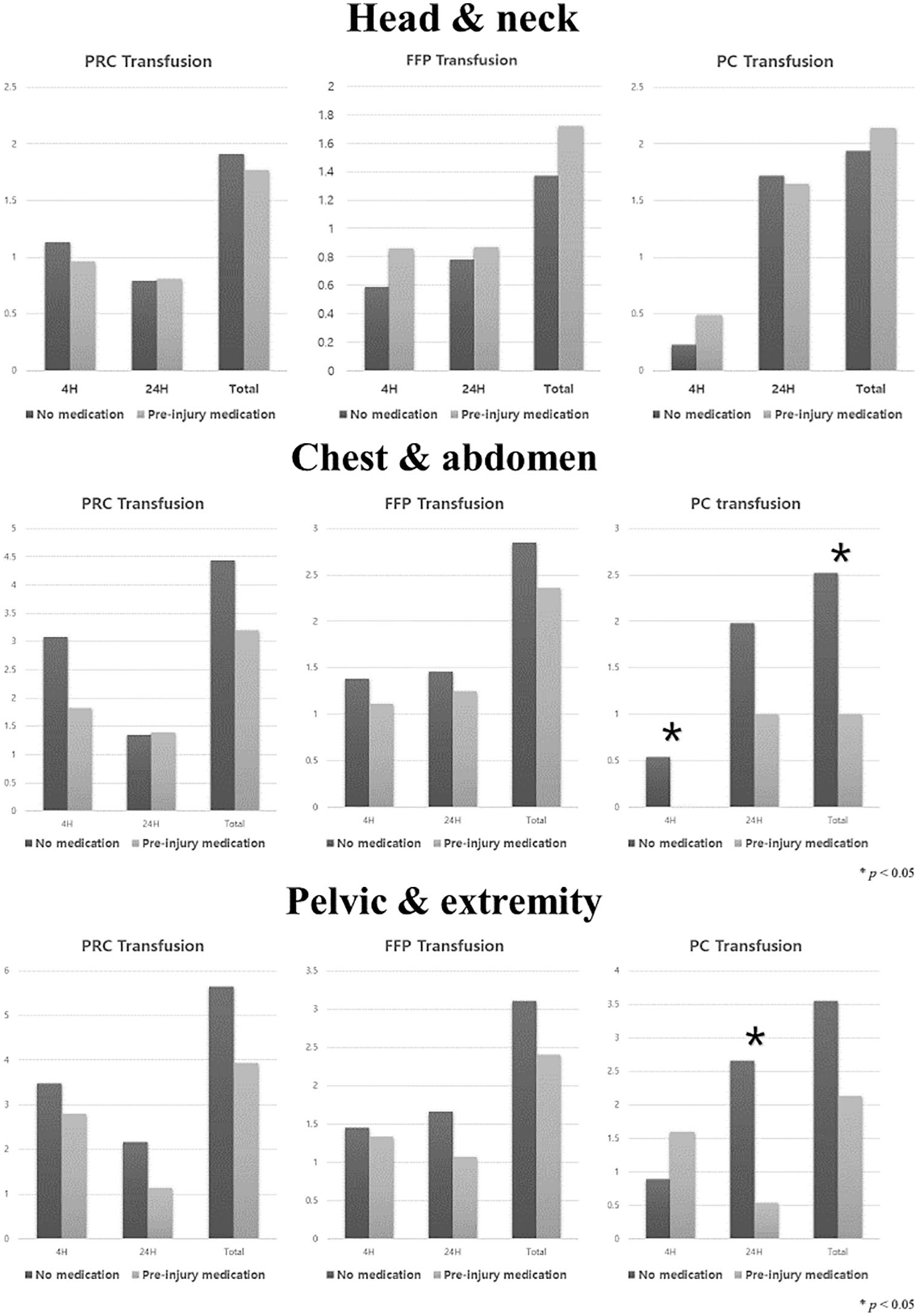
Two-way ANOVA including preinjury medication and main injury site.
Multiple linear regression analysis was performed to determine whether the patient’s age, ISS, and GCS score affected the transfusion volume (Appendix 4). All regression models showed statistically significant (p < 0.01) values, and the PRC, FFP, and PC transfusion volume was shown to increase with an increase in the ISS (p < 0.01). Furthermore, a decrease in the GCS score was associated with a significantly increased PRC and FFP transfusion volume (p < 0.05), although the differences in the PC transfusion volume were not statistically significant.
As there were significant differences in transfusion requirements based on the ISS, GCS score, and main injury site, multivariable ANCOVA was performed to control this effect and to determine the difference in transfusion volume according to the preinjury medication use. As shown in Table 5, there was no statistically significant difference in the blood transfusion volume based on the use or absence of preinjury medication.
Multivariate analysis of ANCOVA of transfusion data.
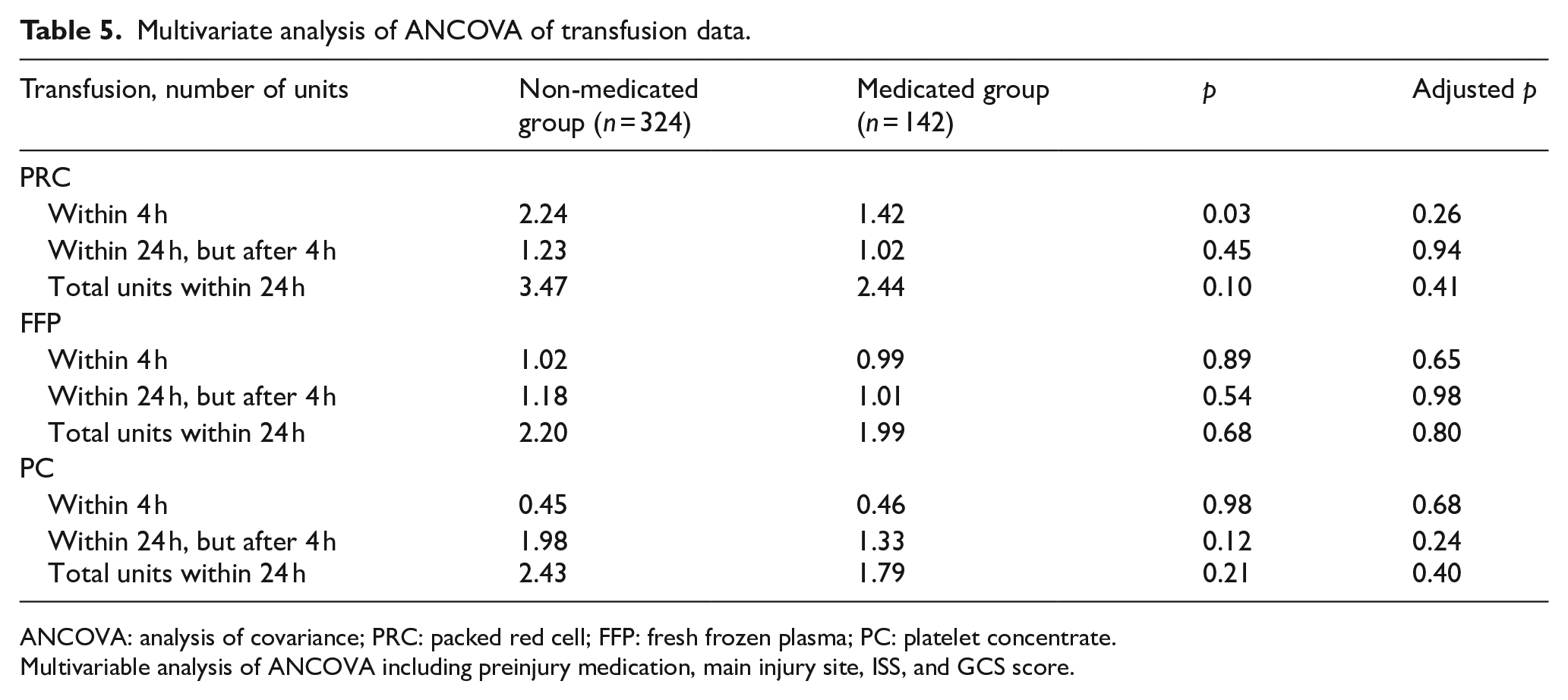
ANCOVA: analysis of covariance; PRC: packed red cell; FFP: fresh frozen plasma; PC: platelet concentrate.
Multivariable analysis of ANCOVA including preinjury medication, main injury site, ISS, and GCS score.
Discussion
This study demonstrated a significantly higher proportion of cardiovascular and cerebrovascular diseases in the medicated group than in the non-medicated group. This difference was mostly attributable to drugs such as warfarin, aspirin, and clopidogrel that are not only used to prevent cardiovascular and cerebrovascular disease but also to reduce complications from these diseases.8,13 Table 1 shows that the medicated group had more instances of slip injury. Slip injury occurs with less energy than motor vehicle accidents or falls, and is more frequent in elderly individuals.8,20,21 Bhattacharya et al. reported that the older the patients are, the harder they fall due to their impaired physical responses. 22 Nevertheless, high-energy trauma, such as motor vehicle accidents, in the elderly is also increasing due to the increased outdoor activities of the elderly population. 23 The average age of patients in the two study groups is similar in this study; thus, instead of the older age, the lower activity of the medication group due to underlying diseases would have resulted in an increased incidence of low-energy trauma. In addition, it seems that elderly patients who were administered with anticoagulants and/or antiplatelet medications were prone to slip and fall due to cerebrovascular diseases such as stroke. The ISS was lower in the medicated group (Table 1).
This study found that the medicated group sustained more head and neck injuries. Bhattacharya et al. 22 reported a higher risk of cranial hemorrhage in patients on aspirin who suffered a ground-level fall injury. Conversely, Boltz et al. 24 reported that anticoagulants increased the risk of complications from intra-abdominal injury after slipping. This study found similar results as that reported by Bhattacharya et al., wherein there were more incidents of low-energy injury in the medicated group, with a resultant higher proportion of head and neck injuries.
Anticoagulant and antiplatelet medications are known to cause coagulopathy, 13 whereas other studies report coagulopathy only in trauma patients with hemorrhage who are on anticoagulants.25,26 This study did not identify a difference between the medicated and non-medicated groups with respect to coagulopathy. However, when classified according to drug type, as shown in Table 2, the warfarin group showed a higher INR than the other groups. This result is similar to that of previous studies, although this study is hampered by the limitation that the sample size of the warfarin group was very small. Further research with a larger study cohort over a longer duration could generate more valuable results.
Several studies have reported a negative effect of preinjury anticoagulant or antiplatelet medication use on the morbidity and mortality of trauma patients, although there were no differences in blood loss or transfusion amount based on the medication.8,14,15 A study in 2012 reported that preinjury antiplatelet medication use did not influence blood loss or transfusion amount, 16 whereas another study in 2016 reported that only preinjury warfarin use increased the risk of hemorrhage. 17 Ohmori et al. reported that preinjury anticoagulant and antiplatelet medication use were major risk factors for massive transfusion in patients with severe trauma. 18 They theorized that there would be a negative effect of preinjury medication use on the transfusion requirement, which was apparently contradicted by the results of our study (Appendix 3). The non-medicated group received significantly more red blood cell transfusions within 4 h of hospital arrival. In addition, in the one-way ANOVA based on the drug type, there was no statistically significant difference in transfusion volume based on whether preinjury medication was used. This result is rationalized by the transfusion amount based on the main injury site, as shown in Table 4. This study demonstrated a higher proportion of head and neck injuries in the medicated group, whereas patients with injuries on the chest, abdomen, pelvis, and extremities received more red blood cell transfusions. Similar to our study, a study reported that more than 70% of hemorrhage cases requiring transfusion occurred in patients with injuries of the chest, abdomen, and pelvis. 27 In 2017, another study reported that positive findings on Focused Assessment with Sonography for Trauma (FAST) and long-bone open fracture of lower limbs as major risk factors of massive transfusion in trauma patients. 18
As mentioned above, injuries in the chest, abdomen, and pelvis result from high-energy trauma, such as motor vehicle accidents and falls. High-energy trauma is known to cause a higher ISS and more severe coagulopathy from extensive tissue damage,10,12 and increase the transfusion demand. 28 Therefore, we conducted multivariate analysis by controlling for ISS and main injury sites, which did not demonstrate statistically significant effects with respect to preinjury medication use on the transfusion amount (Table 5). These results are probably attributable to the limitations of this study, although traumatic hemorrhage is mostly influenced by the energy applied, main injury sites, and injury severity; this needs to be validated in further studies.
There are several limitations to this study. First, this was a single-center study with a small number of medicated patients of a total study sample of 466 patients; an even smaller number of patients were on anticoagulant medications. More valuable results are expected with larger patient samples from multi-center studies. Second, this was a retrospective study based on data extracted from medical records. Most patients’ medical histories were based on reports by the patients and their guardians, which makes the data somewhat unreliable. Third, although most patients arriving at the trauma center were resuscitated and transfused on the basis of trauma transfusion protocols, the actual transfusion requirement is decided by the attending trauma surgeon. As the trauma surgeons undergo rotational posting, the amount of transfusion may not be consistent for similar injuries when managed by different surgeons. More thorough and standardized protocols will allow more consistent data collection. Finally, we did not include the data of patients who died in the emergency room or were admitted to the general ward; thus, our data may not be generalizable to the entire elderly population older than 65 years.
Conclusion
This study did not demonstrate a significant effect of preinjury anticoagulant or antiplatelet medication use on the amount of transfusions required in trauma patients older than 65 years. The main injury site and injury severity were more significantly associated with the amount of transfusion in the early phase of resuscitation. Given the limitations of this study, we can expect more valuable results from larger studies that involve multiple institutes.
Supplemental Material
Supplementary_material – Supplemental material for History of anticoagulant and antiplatelet therapy as a predictive factor for transfusion requirement in elderly trauma patients in intensive care: A retrospective registry–based cohort analysis
Supplemental material, Supplementary_material for History of anticoagulant and antiplatelet therapy as a predictive factor for transfusion requirement in elderly trauma patients in intensive care: A retrospective registry–based cohort analysis by Se Heon Kim, Young Hoon Sul, Jin Young Lee, Jin Bong Ye, Jin Suk Lee, Hong Rye Kim, Soo Young Yoon and Joong Suck Kim in Hong Kong Journal of Emergency Medicine
Footnotes
Author contributions
S.H.K. contributed to the acquisition of data, analysis and interpretation of the data, and drafting of the manuscript; Y.H.S. contributed to study conception and design, acquisition of data, and critical revision of the manuscript; J.Y.L. contributed to the acquisition of data; J.B.Y. contributed to the acquisition of data; J.S.L. contributed to the acquisition of data; H.R.K. contributed to the acquisition of data; S.Y.Y. contributed to the acquisition of data; J.S.K. contributed to the critical revision of the manuscript. All authors reviewed and approved the final submitted manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data sets and analysis during this study are available from the corresponding author on reasonable request.
Informed consent
This study was approved by the Institutional Review Board of the Chungbuk National University Hospital (approval no. 2020-02-004), in compliance with the Informed Consent, Ethical Approval, and Human Rights clauses set forth by the Hong Kong Journal of Emergency Medicine publishing guidelines. Individual consent was waived due to anonymized nature of patient data.
Ethical approval
This study was approved by the Institutional Review Board of the Chungbuk National University Hospital (approval no. 2020-02-004).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.