
Abstract
Background:
Performing endotracheal intubation by placing patients in a ramped position has been shown to improve the ease of intubation and to reduce complications. The above findings, however, were only established in the operation theatre and intensive care settings.
Objective:
In order to establish the findings in the setting of the emergency department, we attempt to compare the ramped versus supine positions in normal and difficult airway scenarios.
Methods:
Medical doctors practicing at a local Accident and Emergency Department were recruited into a crossover randomised study. They were asked to perform intubations on a manikin in four scenarios. The manikin was put in a ramp or supine position. In addition, the manikin settings were adjusted to normal and difficult airways.
Results:
A total of 39 Accident and Emergency Department doctors were recruited. There was no statistically significant difference in the first-attempt success rates using the ramped position compared to supine position in either airway scenario (100% vs. 97.4%, P = 1 in normal airway, 79.5% vs. 74.4%, P = 0.789 in difficult airway). The mean intubation time in difficult airway setting was shorter when the manikin was put into ramped position (28.3 s vs. 38.4 s, P = 0.134). The ramped position improved the glottic view in the difficult airway setting (P = 0.017). More intubators preferred to place the manikin into a ramped position during difficult airway setting (67%, P = 0.007). Experienced male intubators performed better in normal airway scenarios, whereas Accident and Emergency Department fellows performed better in difficult airway scenarios.
Conclusion:
The ramped position improves glottic view and operator ease when intubating a simulated difficult airway.
Introduction
Airway management is always a challenge when dealing with critically ill patients in the emergency department. Proper positioning of the patient is of paramount importance to facilitate successful orotracheal intubation, such as the traditional supine sniffing position and the more recent ramped position. The objective in all of these approaches is to align the oral, pharyngeal and laryngeal axes so as to afford the laryngoscopist optimal visualisation of the glottis. 1
Studies in the anaesthesia literature have described the benefits of using the ramped position.2–4 Collins et al. have promulgated the idea that placing an obese patient in a ramped position improves laryngoscopic grade. 2 These findings were corroborated by Lebowitz et al., 3 who found equal or better laryngoscopic views for the entire study population of various body mass index values.
The proposed mechanism by which the ramped position results in view improvement is that during neck extension, anterior displacement of the glottis occurs, which moves the larynx away from the line of vision. Neck flexion moves the larynx posteriorly, bringing it into view and allowing easier exposure with little effort. Neck flexion also increases the range of motion at the atlanto-occipital joint, allowing more extension at that joint. Head elevation may also have the advantage of decreasing the amount of force required for the intubator to lift the patient’s tissues out of the way. 4
In addition to potentially affecting intubation difficulty, some have suggested that an upright position might have other clinically important benefits. The ramped position increases functional residual capacity, thereby improving preoxygenation and prolongs safe apnea time. In intensive care unit (ICU) settings, it is associated with lower rates of complications, including aspiration, hypoxemia and oesophageal intubation. 5
Despite the abundance of data in the anaesthesia and intensive care literature, there is little data to support this technique in the emergency department setting. An observational study by Turner et al. 6 only described that emergency medicine residents had a higher first-pass success rate when intubating in the upright position, but did not evaluate other outcomes. In this prospective randomised crossover study, we evaluated the first-attempt success rate, time to intubation, glottic view and intubator preference when performing endotracheal intubation in both the ramped and supine positions in manikins. Furthermore, normal and difficult airway scenarios were simulated in the manikins.
Materials and methods
This prospective randomised crossover manikin study was conducted at the Hong Kong East Cluster (HKEC) Training Centre for Healthcare Management and Clinical Technology located in Pamela Youde Nethersole Eastern Hospital (PYNEH). Written informed consent for voluntary participation was obtained prior to recruitment and participants were allowed to withdraw at any time. No patient data were included in this study.
Medical doctors working in the Department of Accident and Emergency in PYNEH were recruited into this study. Those who were not available during the study period or did not agree to perform the study were excluded. Demographic data of each subject’s gender, experience (basic trainee, higher trainee or fellow) and estimated number of intubations in the past 3 months were recorded.
Two identical manikins (SimMan 3G, Laerdal Medical, Stavanger, Norway) were placed side by side, with one in a supine position and the other in a ramped position. A ramped position was achieved by raising the head of the bed until the external auditory meatus and the sternal notch were in the same horizontal plane. All equipment was set up by the same staff of the Training Centre to ensure consistency, who then draped the manikins with bed sheets so that both participants and investigator were blinded to their positioning (Figure 1). Difficult airway was simulated by electronically changing manikin settings to have trismus, tongue oedema and pharyngeal swelling by Training Centre staff in a separate control room.
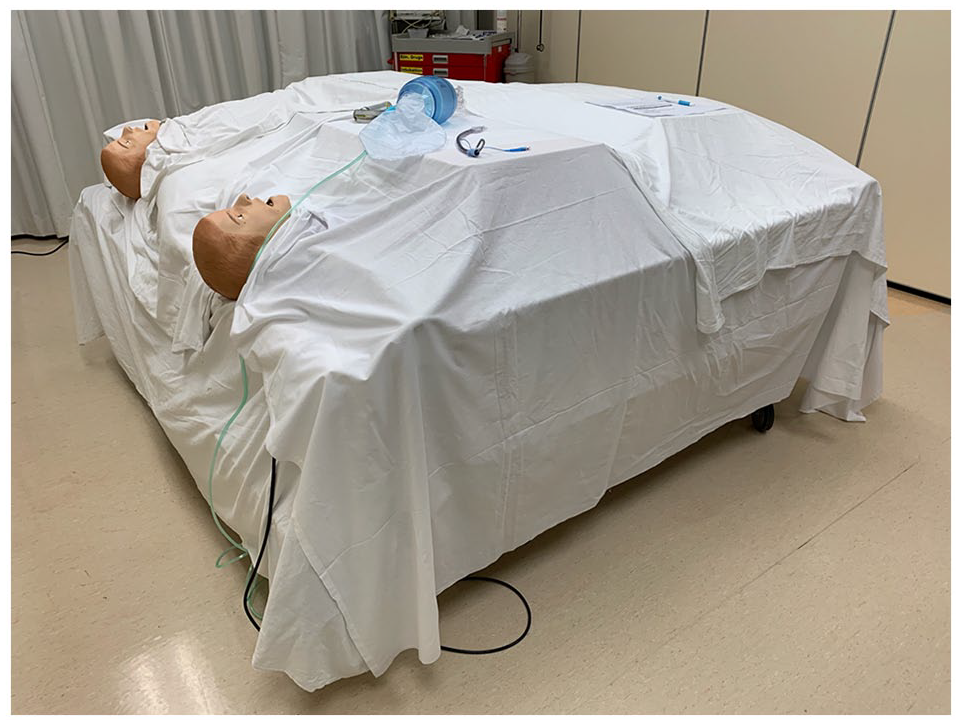
Blinding of manikins placed in the supine and ramped positions.
Upon arrival at the Training Centre, subjects were randomised to the normal airway first or the difficult airway scenario first. They were allowed 30 s of practice on both manikins in each airway setting to familiarise themselves with the equipment. Subjects were then allocated to supine position first or ramped position first. Both subjects and investigator were blinded to the randomisation results.
Participants were instructed to intubate the manikins with a seven French endotracheal tube using a Macintosh size 4 blade. They were timed from the removal of the bag-valve mask from the manikin’s face until the endotracheal tube is released, to the nearest hundredths of a second. The subjects were required to grade the best view obtained during laryngoscopy using the modified Cormack–Lehane classification after each intubation (Figure 2). 7 After completing intubations of both manikins in the same airway scenario, they were asked which manikin was easier to intubate.
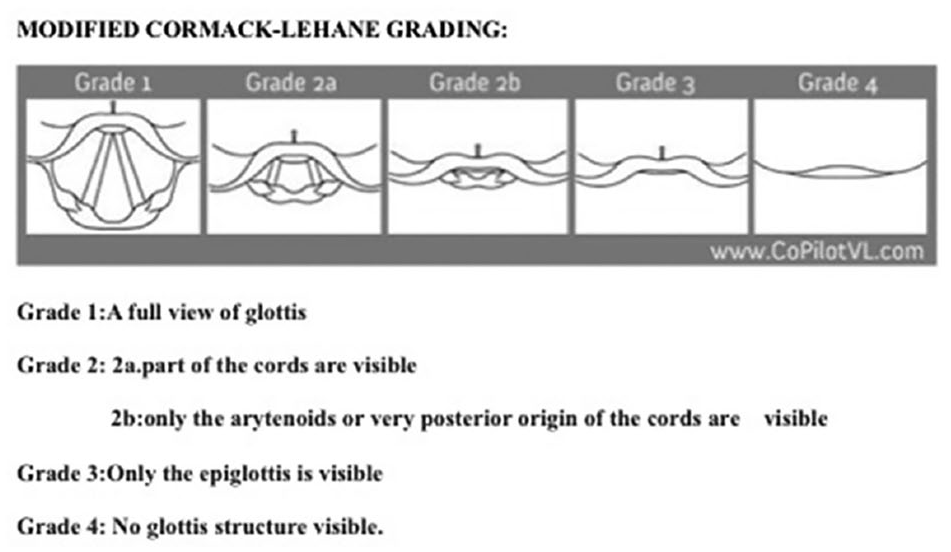
Modified Cormack–Lehane grading. 7
The primary outcome of interest was successful first-attempt endotracheal intubation. One laryngoscopy attempt was defined as the insertion of a laryngoscope into the oral cavity.
Secondary outcomes included time to successful intubation, best glottic view obtained and intubator preference. It has been found that prolonged intubation attempts of more than 3 min were associated with higher rates of aspiration, hypoxia and cardiac arrest. 8 Thus in our study, if the attempt exceeded 3 min, it was considered a failed attempt and the time to intubation would be censored.
The Fischer’s exact test was used to analyse categorical results (glottic view and preference) and the sample t-test for intubation time. Cox 9 proportional hazards model was used to determine whether gender, experience and the number of intubations in the past 3 months were significant covariates of intubation time.
Results
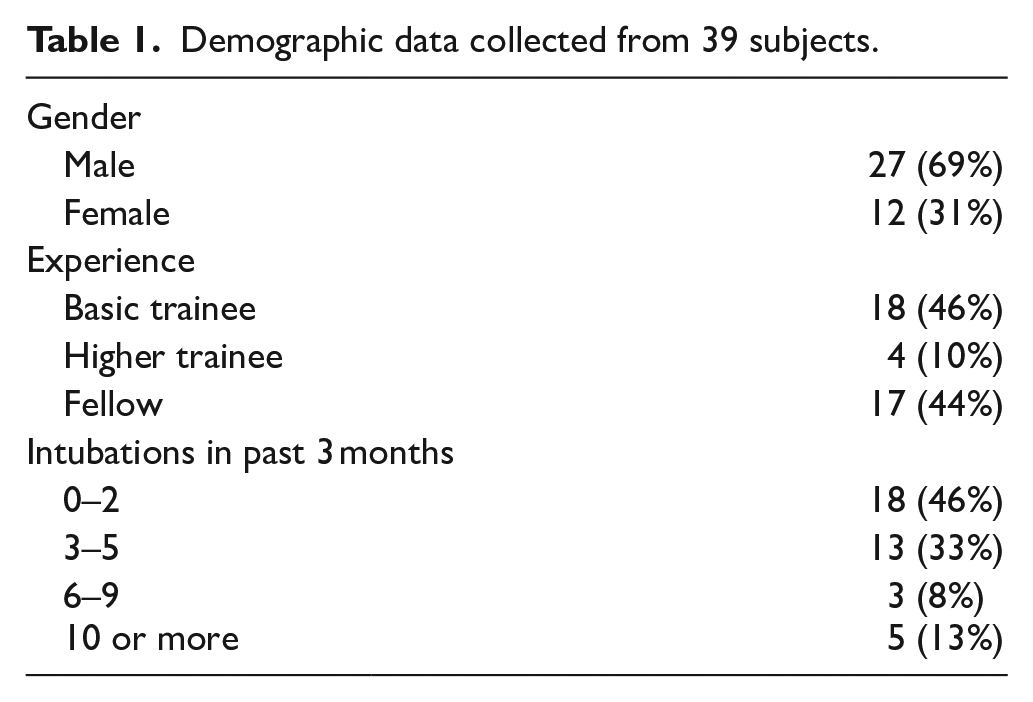
A total of 39 doctors participated in the study. There was more than twice the number of males than females (27 and 12, respectively), with 46% being basic trainees. More than half reported to have intubated three or more patients in the past 3 months. Table 1 depicts the demographic characteristics of the subjects. Tables 2 and 3 and Figures 3 and 4 summarise the primary and secondary outcomes.
Demographic data collected from 39 subjects.
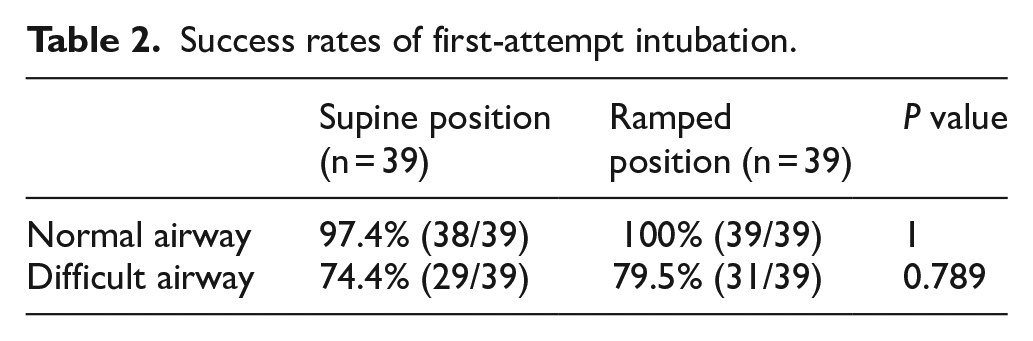
Success rates of first-attempt intubation.
Time to successful intubation.
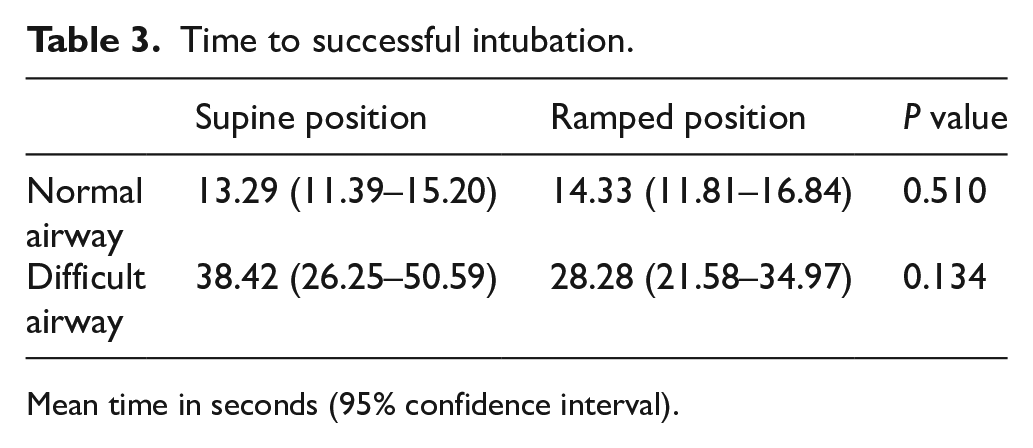
Mean time in seconds (95% confidence interval).
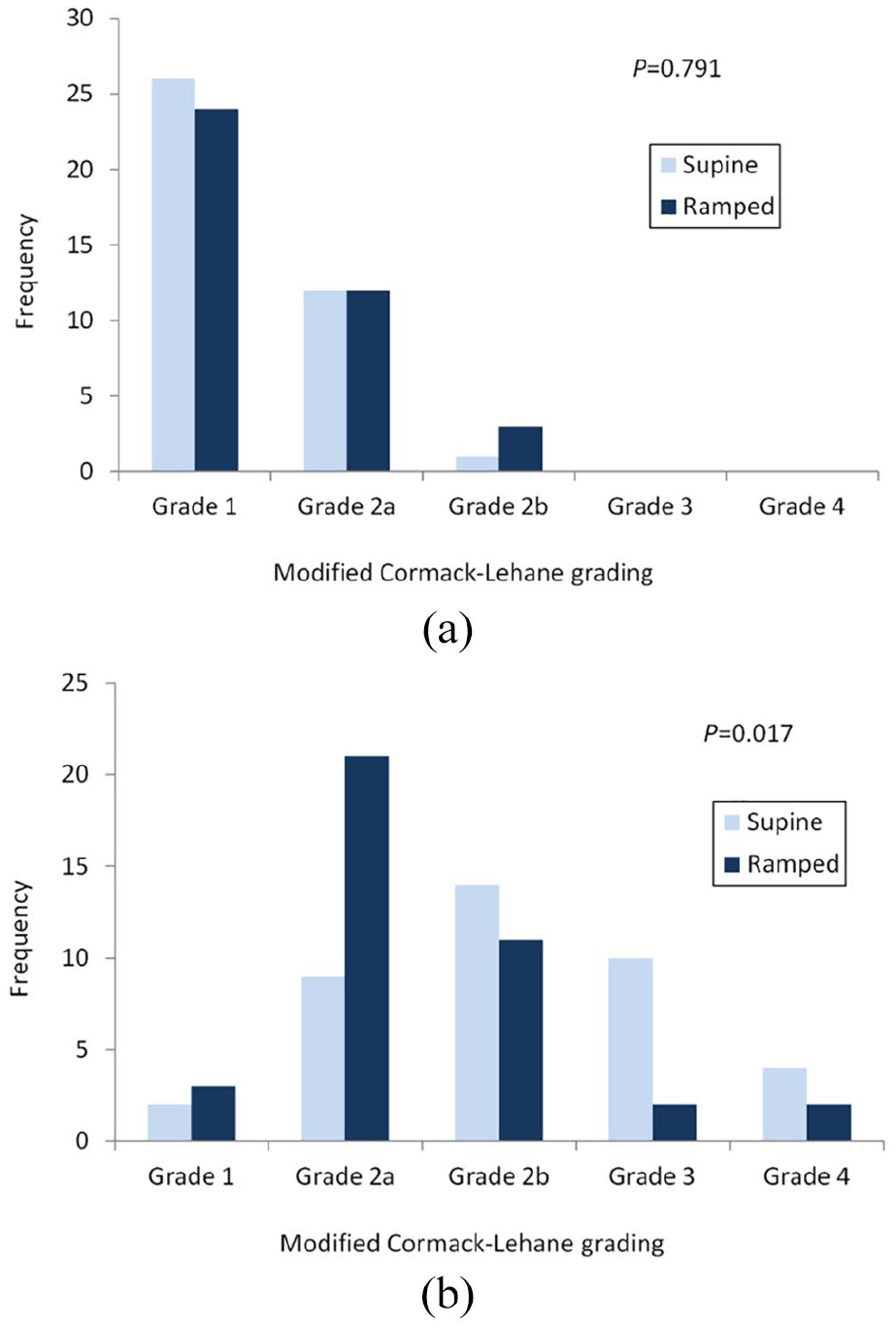
(a) Comparing the best glottic views obtained in the normal airway scenario and (b) comparing the best glottic views obtained in the difficult airway scenario.
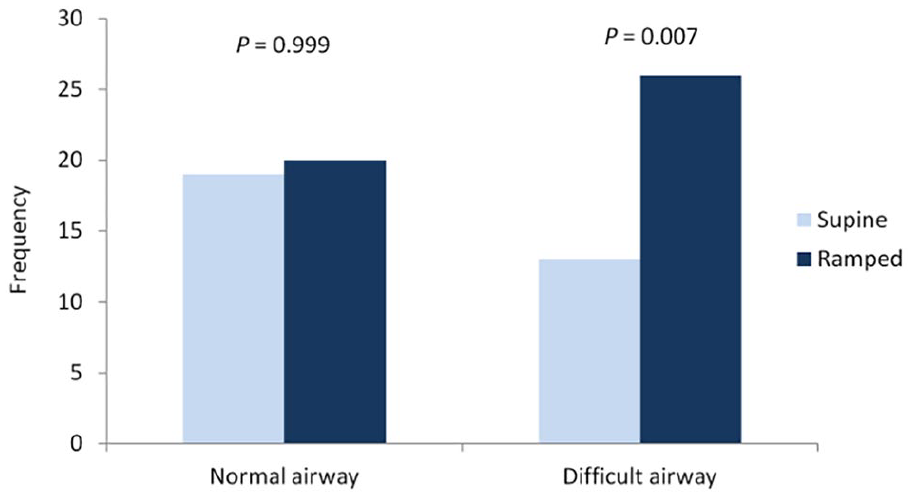
Operator preference in each airway scenario.
Normal airway scenario
The first-attempt success rates in both positions were similar – 100% in ramped and 97.4% in supine positions. The mean times to intubation were also comparable, with supine position being 1 s faster, but it was not statistically significant (P = 0.510). The best glottic view achieved did not differ significantly between the supine and ramped positions, with 97% and 92% obtaining grade 2a or better views, respectively (P = 0.791). Operators did not favour one position significantly more than the other, with 49% picking supine position and 51% picking ramped position (P = 0.999).
Difficult airway scenario
The first-attempt success rate was 5% higher in the ramped position, but it was not statistically significant (P = 0.789). The mean time to successful intubation was 10 s shorter in the ramped position, but again not statistically significant (P = 0.134). More operators achieved a grade 2a or better view in the ramped position than in the supine position (62% vs. 28%, P = 0.017). Twice the number of operators preferred the manikin lying in a ramped position over the supine position when asked which was easier to intubate (P = 0.007).
Hazard ratios for the effects of various covariates on the time of intubation were obtained from Cox proportional hazard models. In the normal airway scenario, it appears that male intubators and those who performed more intubations in the past 3 months were associated with a shorter intubation time (Figure 5(a)). However, only fellows demonstrated shorter intubation times in the difficult airway scenario (Figure 5(b)).
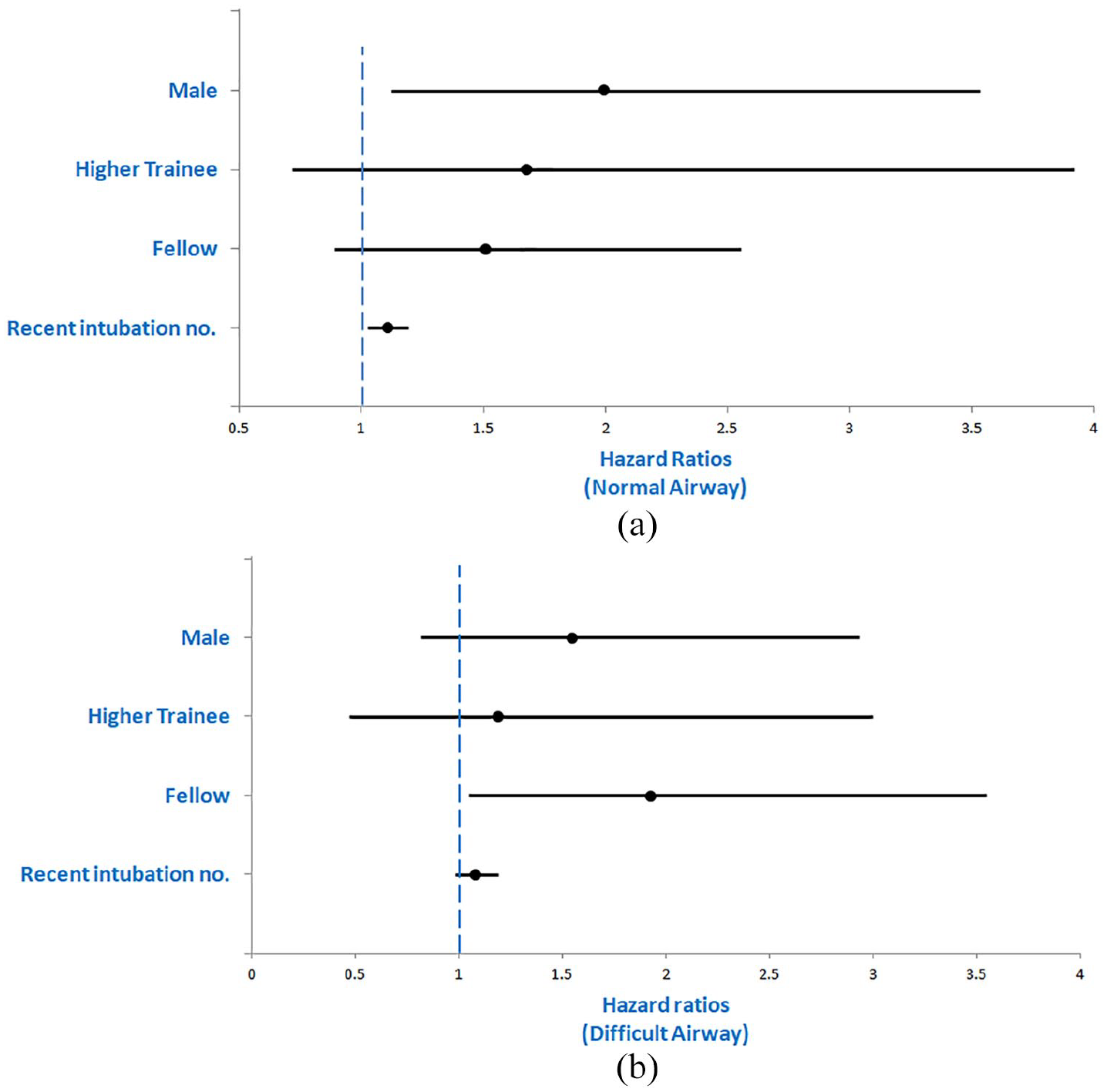
(a) Effects of covariates on intubation time in the normal airway setting and (b) effects of covariates on intubation time in the difficult airway setting.
Discussion
In the majority of previous reported trials, intubations were performed by experienced anaesthetists or intensivists.2–6 However, several manikin studies were solely aimed at novice intubators.10,11 This pilot study involving emergency physicians of various experience may better reflect the effects of altering patient positioning on intubation performance in the emergency department.
In the normal airway scenario, the ramped position was neither significantly superior nor inferior to the supine position in any of the outcome measures. It could be argued that proper head positioning may not be needed when the patient has a grade 1 larynx, because there could be no further improvement in an already perfect view. The effect of proper positioning might be instrumental, however, when a difficult airway is anticipated.
In the difficult airway scenario, there was a statistically significant improvement in glottic view. This concurs with previous studies in the anaesthesia literature. This improvement in glottic view may in turn be the reason why two-thirds of the subjects found the manikin in the ramped position easier to intubate. In spite of this, the first-attempt success rates in both positions were not statistically different. Moreover, upon reviewing the raw data, the apparent 10 s difference in mean intubation time was a result of an outlier prolonging the mean intubation time in the supine position. The median times to intubation in the ramped and supine positions were more comparable at 21.49 and 23.19 s, respectively.
Baseline characteristics of the subjects may have an impact on their performance. Male intubators demonstrated an advantage in speed over their female counterparts in the normal airway scenario. One could presume it may be due to males applying more force during laryngoscopy when lifting the manikin’s soft tissues out of the way. However, this apparent edge did not prevail in the difficult airway scenario. Fellows markedly outperformed basic trainees in the difficult airway scenario, reflecting that skill and experience rather than force may be the key to manoeuvre through a difficult airway.
Our study had multiple limitations. First and foremost, a manikin can never fully imitate a real patient. The main advantage of using manikins is it allows for controlled and reproducible normal and difficult airway scenarios, which could never be attained in real patients. Given the paucity of data regarding the use of ramped position in the emergency medicine literature, it may not be ethically sound to recruit real patients. The ramped position may not be feasible in all circumstances, such as during cardiopulmonary resuscitation, or in patients with spinal injuries, severely arthritic or degenerative spines.
As with all crossover trials, the statistical pitfalls of crossover, sequence and period effects exist. The major carryover effect in our case would be the learning curve. One way of dealing with this would be introducing a washout period, but there is no definition of how long it should be nor is it practical to perform. Our solution was to allocate a set time for practice, to allow for adequate familiarisation with equipment in order to minimise the effect of learning on our data. We randomised the order of intubation in attempt to nullify the sequence effect. Further analysis was performed to see whether the intubation sequence had an effect on the time to intubation, and the results were all statistically not significant. As all four intubations were carried out in the same setting, period effect was negligible as there was no change in subject baseline characteristics throughout the study.
In summary, this study has shown that the ramped position performed better or equivalent to supine position in all outcome measures in both airway scenarios, with significantly improved glottic view and intubator ease in the difficult airway scenario. We believe that placing patients in the ramped position is a relatively easy manoeuvre to perform, has no associated cost, is easily understood and executed by staff, and requires no advanced technology or power source other than the bed. We believe that more studies need to be carried out using larger sample sizes across multiple centres before trials on real patients.
Conclusion
In our study, endotracheal intubation in the ramped position improved glottic view and operator ease in a simulated difficult airway.
Footnotes
Acknowledgements
The authors express sincere gratitude to the staff of the Hong Kong East Cluster Training Centre for Healthcare Management and Clinical Technology for their kind assistance.
Authorship
Dr Carolyn Cheuk Lam Hung and Dr Anthony Wong contributed to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
Manikin study was conducted in Hong Kong East Cluster Training Centre for Healthcare Management and Clinical Technology of Pamela Youde Nethersole Eastern Hospital.