
Abstract
Background:
After failed endotracheal intubation, using direct laryngoscopy, rescued using a supraglottic airway device, the choice of subsequent method to secure a definitive airway is not clearly determined.
Objective:
The aim of this study was to compare the time to intubation using a fibre-optic airway scope, to guide an endotracheal tube through the supraglottic airway device, with a more conventional approach using a hyperangulated video laryngoscope.
Methods:
A single-centre randomised controlled trial was undertaken. The population studied were emergency physicians working in an adult major trauma centre. The intervention was intubation through a supraglottic airway device guided by a fibre-optic airway scope. The comparison was intubation using a hyperangulated video laryngoscope. The primary outcome was time to intubation. The trial was registered with ANZCTR.org.au (ACTRN12621000018819).
Results:
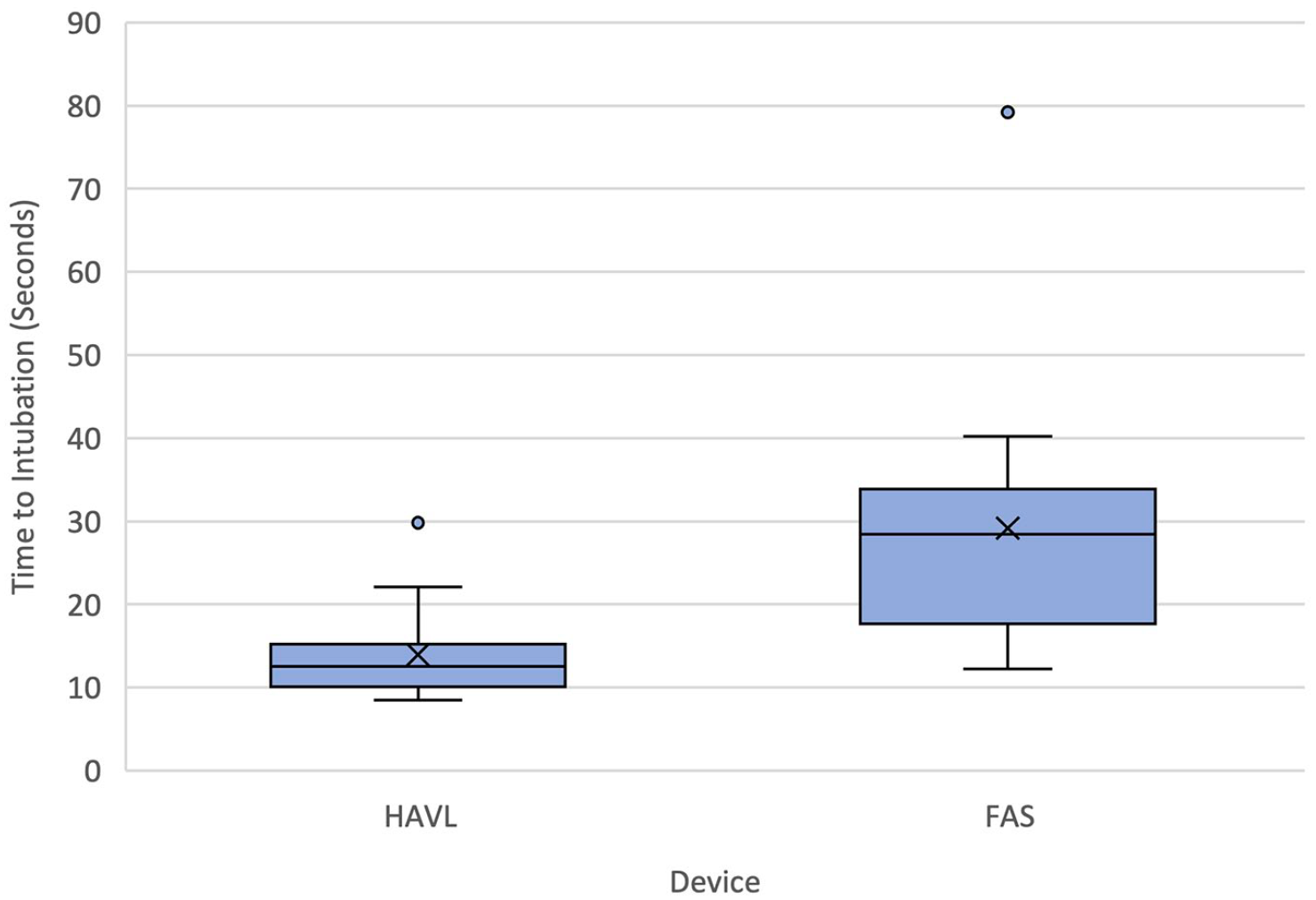
Four emergency physicians completed intubations using both of the two airway devices on four cadavers for a total of 32 experiments. The mean time to intubation was 14.0 s (95% confidence interval = 11.1–16.8) in the hyperangulated video laryngoscope group compared with 29.2 s (95% confidence interval = 20.7–37.7) in the fibre-optic airway scope group; a difference of 15.2 s (95% confidence interval = 8.7–21.7, p < 0.001). All intubations were completed within 2 min, and there were no equipment failures or evidence of airway trauma.
Conclusion:
Successful intubation of the trachea without airway trauma by emergency physicians in cadavers is achievable by either fibre-optic airway scope via a supraglottic airway device or hyperangulated video laryngoscope. Hyperangulated video laryngoscope was statistically but arguably not clinically significantly faster than fibre-optic airway scope via supraglottic airway device.
Introduction
While the majority of fibre-optic endotracheal intubations occur in the operating theatre environment by anaesthetists, the frequency with which any individual anaesthetist performs this technique has reduced, with a recent New Zealand study estimating a current average of three fibre-optic intubations per year. 1 This decline in opportunity for skill maintenance is likely to get worse with the widespread introduction of video laryngoscopes. 2 Nasendoscopy is a safe and reliable way to assess the upper airway and the frequency with which this technique is being performed in the emergency department (ED) is increasing with the availability of affordable single-use nasendoscopes. Slightly longer versions of these devices allow both nasendoscopy as well as intubation and will be described in this study as flexible airway scopes (FASs).
Although ED tracheal intubation (ETI) has been shown to have a high first attempt success rate, 3 failure to intubate using a MacIntosh direct or video laryngoscope does occur, and rescue ventilation may be achieved by the placement of a supraglottic airway device (SAD) as per the Difficult Airway Society (DAS) recommendations. 4 The placement of a definitive airway with a cuffed endotracheal tube (ETT) may still be needed, however, and for patients with a difficult airway, the subsequent method of intubation is not clearly established. Video laryngoscopy using a hyperangulated blade may be attempted, but, in the scenario described, requires the removal of the rescue SAD. Should laryngoscopy again be unsuccessful, this may lead to a life threatening ‘can’t intubate can’t ventilate’ situation if the SAD is unable to effect ventilation on reinsertion necessitating an emergency cricothyroidotomy. An alternate approach is tracheal intubation by passage of an ETT through the SAD, which can be left in situ, guided by an FAS. 5 In this study, we have chosen to compare the success rate and time to intubate the trachea of a fresh-frozen cadaver using a more traditional approach to the difficult airway, hyperangulated video laryngoscopy (HAVL), with a novel method where the FAS is guided into the trachea through an SAD. 5
Methods
Study design and participants
This randomised controlled trial was registered before clinician enrolment at Australian New Zealand Clinical Trials Registry (ACTRN12621000018819). Four fresh-frozen cadavers were provided by the University of Melbourne’s Department of Human Anatomy and prepared for the experiment with ethanol irrigation of their upper airways. Four emergency physicians (EPs) were enrolled from the Alfred Hospital Emergency & Trauma Centre, which is one of two level-1 adult major trauma centres (MTCs) in the Victorian Trauma System located in Melbourne, Australia.
Intervention
Prior to the experiment, participants received an hour of familiarisation and training with the FAS and hyperangulated video laryngoscopes (Figure 1).
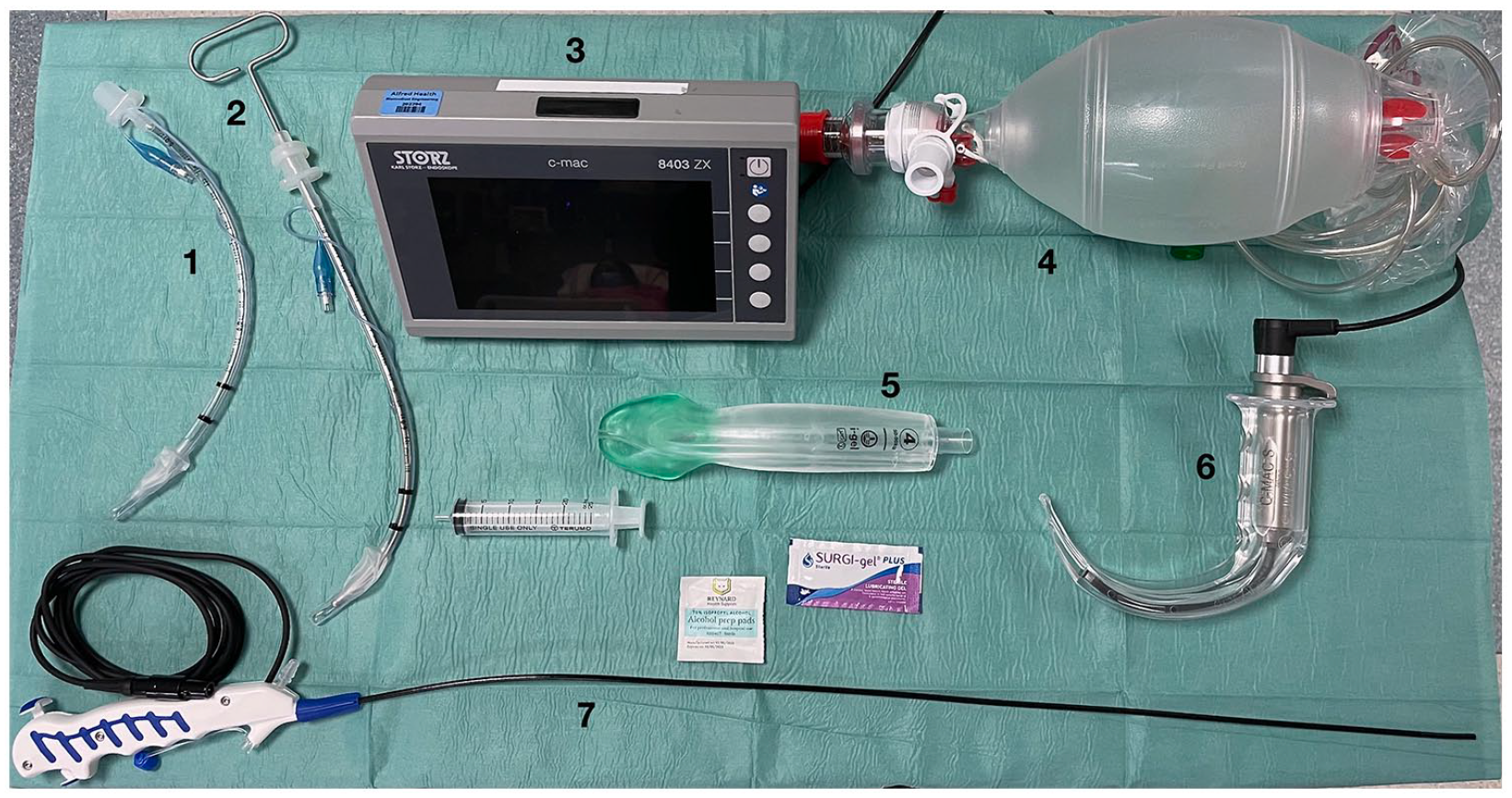
Equipment.
Each EP performed both techniques on all four cadavers amounting to 32 experiments, the order of which was randomised in advance by computer randomisation to minimise learning effects (https://www.randomizer.org). The FAS was a single-use Karl-Storz C-MAC® Five S flexible intubation video endoscope, 65 cm in length with a 3 mm diameter. The HAVL was a C-MAC® video laryngoscope with a D-blade. The SAD was an Intersurgical i-gel® in either a size 3 or 4 depending on the size of the cadaver. The ETT was a Portex Choice size 6.0 mm cuffed tracheal tube and was preloaded onto the FAS or a C-MAC® Stylet.
For all the experiments, the starting condition was with the supine cadaver being ventilated using an Ambu® SPUR® II disposable resuscitator (BVM) connected to the SAD. This starting condition was chosen to simulate the decision point after a failed intubation where the patient can be ventilated using an SAD.
Outcomes
Time to intubation, the primary outcome, was defined as the time from disconnecting the BVM from the SAD to the inflation of the ETT cuff by the airway assistant. Oesophageal intubation, or exceeding 2 min, was defined as a failed intubation. The final position of the ETT was then confirmed, and the airway assessed for evidence of trauma, by the first author using direct laryngoscopy and the FAS.
Statistical analysis
A sample size of four participants (a minimum of either four cadavers or four clinicians) was determined by power analysis based on an alpha of 0.05, a power of 80% and a small difference in time to successful intubation between procedures (10 s, paired by operator and cadaver, was chosen for the calculation based on consensus of investigators). Symmetrical numerical data have been summarised using the mean value (standard deviation (SD)); skewed numerical data have been summarised using the median (interquartile range (IQR)); and categorical data have been summarised using frequencies (%). The statistical significance of these measures of association was tested using paired statistical testing procedures, that is, paired Student’s t-test, the Wilcoxon signed-rank test or McNemar’s test, respectively, as appropriate. p-values < 0.05 were considered statistically significant.
Results
The planned sample size was achieved with all four clinicians completing the procedure on each of the four cadavers for a total of 32 experiments. Characteristics of the cadavers and participants are presented in Tables 1 and 2, respectively.
Characteristics of cadavers.
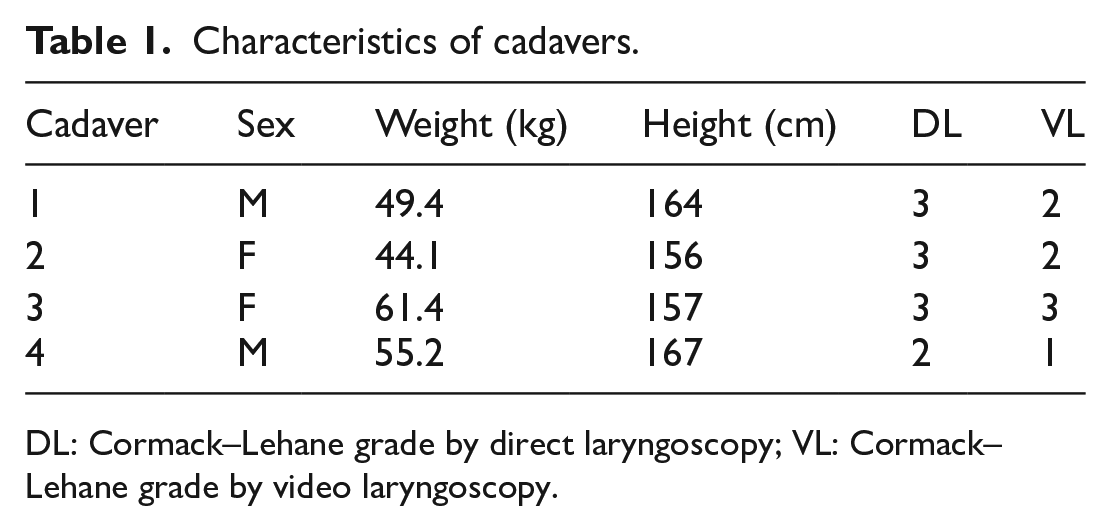
DL: Cormack–Lehane grade by direct laryngoscopy; VL: Cormack–Lehane grade by video laryngoscopy.
Characteristics of participants.
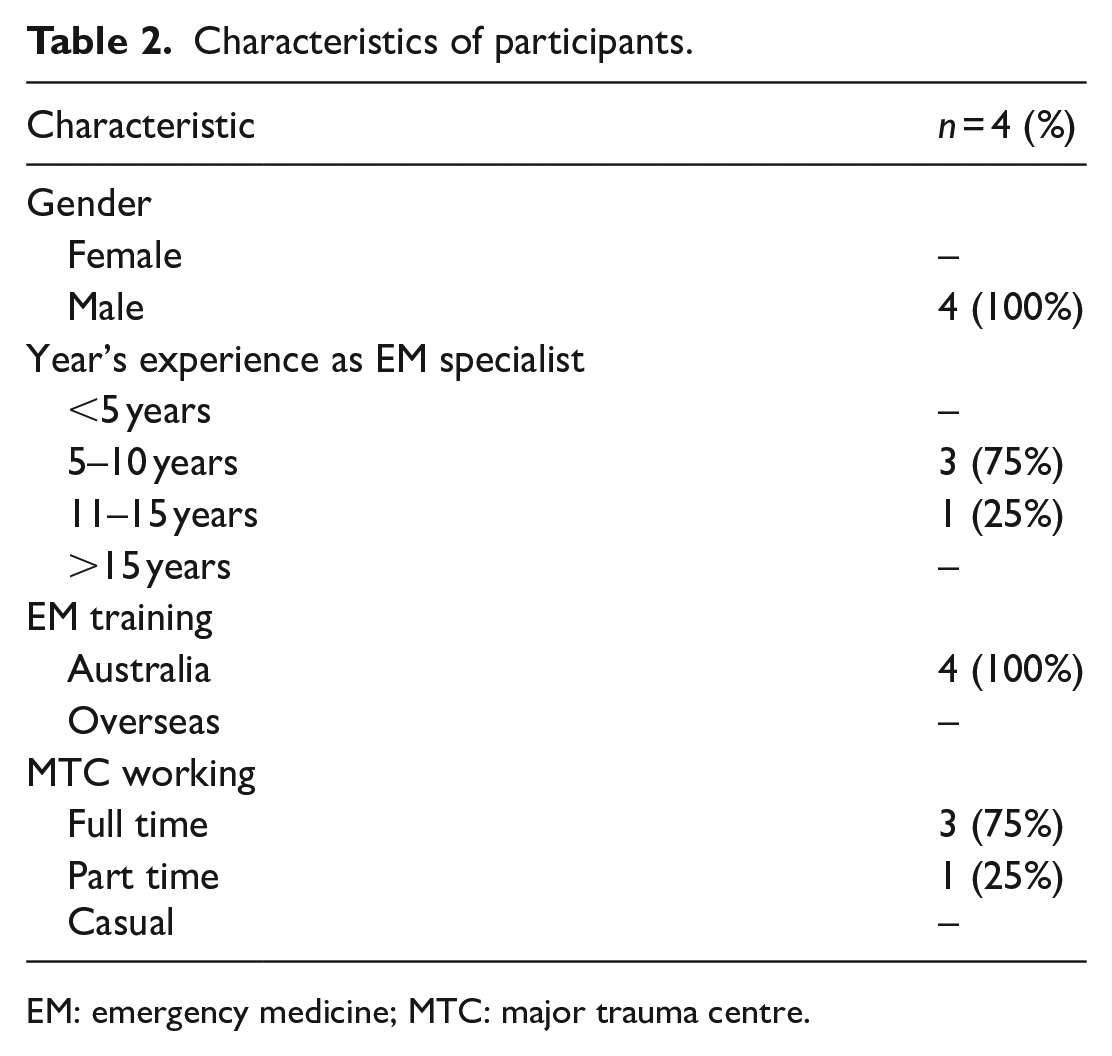
EM: emergency medicine; MTC: major trauma centre.
Time to intubation (Figure 2), success rates and airway trauma findings are reported in Table 3.
Time to intubation.
Technique performance outcomes.
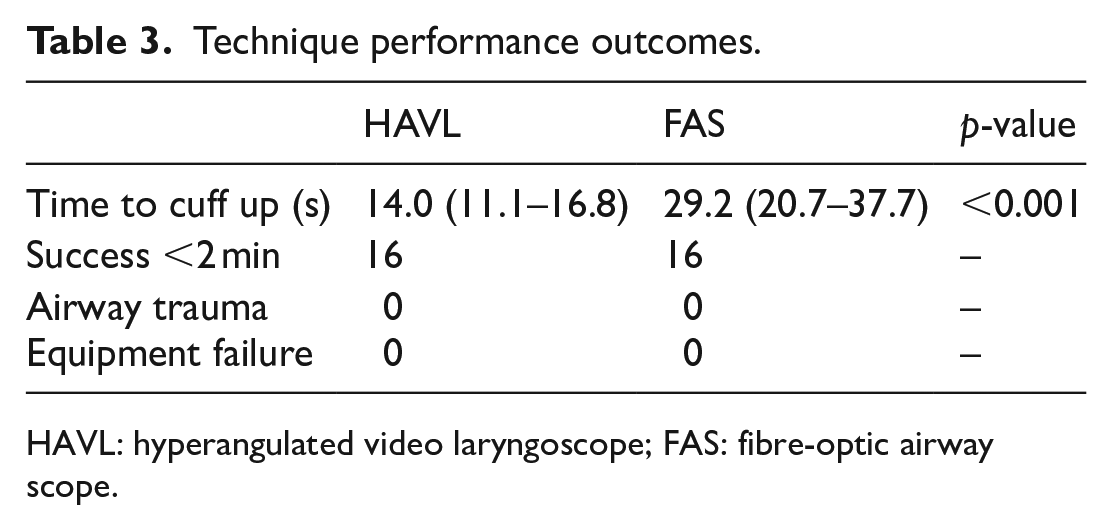
HAVL: hyperangulated video laryngoscope; FAS: fibre-optic airway scope.
The difference in mean time to cuff inflation for the two procedures was 15.2 s (95% confidence interval (CI) = 8.7–1.7, p < 0.001). All intubations were completed within 2 min, and there were no equipment failures or evidence of airway trauma.
Discussion
This randomised controlled trial compared the time taken for intubation between HAVL and FAS-guided intubation through an SAD. The investigators chose to define the primary outcome as time from disconnection of BVM, from in situ SAD, to ETT cuff inflation, to reflect the envisaged clinical scenario relevant to this research. The time to ETT cuff inflation was chosen as the first consistent moment of successful intubation between the two techniques.
This study determined that the time to cuff inflation was shorter with the HAVL than the FAS, but there was no difference in success rates between the groups. Participants involved in the study routinely use video laryngoscopes in their clinical practice, and this may partly explain the faster time achieved with these devices. In addition, whereas for HAVL intubations, the stylet-mounted ETT is passed directly towards the larynx through the mouth, for FAS intubations, the ETT must be navigated through the, relatively snug, lumen of the SAD device which may also increase the time to cuff inflation.
Despite the FAS method being slower, by more than the 10 s deemed clinically important for the sample size calculation, in hindsight, a period of 15 s difference, where both procedures took less than, on average, 30 s to complete, is of dubious clinical significance. In the scenario of a failed intubation by the MacIntosh-geometry direct, or video, laryngoscopy, oxygenation is possible to some degree using the SAD. Removal of the SAD to attempt HAVL is not without risk and may lead to a life-threatening can’t intubate can’t ventilate situation necessitating a surgical airway. 4 Furthermore, should HAVL not be successful, intubation can still be attempted using an FAS via the rescue SAD.
Prior studies have reported on the outcomes of FAS-assisted intubations in the ED. Analysing the National Emergency Airway Registry (NEAR) data, Hayden and colleagues 6 reported that approximately 1% of the airway encounters involved an FAS as a primary or rescue airway technique. Moreover, of the 180 intubations where FAS was used as the primary airway technique, 53% were performed by emergency medicine doctors. 6
We have demonstrated that EPs with a brief familiarisation and training intervention are able to successfully utilise an FAS to intubate the trachea via an SAD without causing airway trauma. The use of FAS by EPs is likely to increase over time as the cost of disposable scopes decreases and additional indications for their use are established, facilitating skill acquisition and maintenance. A recent study by Finnegan and colleagues 7 demonstrated the effectiveness of an FAS to achieve optimal positioning of an intercostal catheter in the thoracic cavity. Assessment of the airway by EPs may also be indicated for patients with burns, 8 foreign body management 9 and laryngeal dyskinesis. 10
There are limitations to this study. First, it used cadavers rather than anaesthetised ED patients and so the results cannot be automatically extrapolated to this patient group, nor does the study allow us to assess any physiological consequences of the techniques. Moreover, the cadavers used did not have anatomically difficult airways, which is the scenario under consideration in this study, and no modifications were made to increase the difficulty of intubation, for example, application of cervical collar to mimic neck immobility. Fresh-frozen cadavers represent the best existing alternative model for this type of research, however, particularly when compared with manikin models. Second, the study’s participants were a relatively homogeneous group of experienced EPs from a single high volume trauma centre, undertaking the procedure immediately after familiarisation with the techniques, and this may also limit the generalisability of the findings.
This randomised controlled trial had a secondary benefit of demonstrating feasibility and safety in the use, under experimental conditions using cadavers, of the FAS technique. Subsequent studies would ideally assess the technique in real patients in the ED. However, from our ongoing airway registry data, 3 patients who require SAD insertion following failed intubation are rare, occurring in less than 0.2% of intubations (unpublished data). Based on these numbers, a Phase 2 study would need to include multiple centres over an extended period of time. Regarding the broader use indications for FAS, in EDs that adopt this technology, future studies could look at how often, and for what indications, individual EPs use the device per year. In addition, as the technique becomes more commonplace, FAS intubation through SAD could be added to airway registries to allow analysis of their real-world performance over time.
Conclusion
Successful intubation of the trachea without airway trauma by EPs in fresh-frozen cadavers is equally achievable by either FAS via an SAD or HAVL. HAVL was statistically but arguably not clinically significantly faster than FAS via an SAD.
Footnotes
Acknowledgements
The authors thank Karl-Storz for the loan of equipment to undertake the experiments.
Authors contributions
All authors made substantial contributions. C.J.G., A.M. and G.O. did the conception and design of the study. C.J.G., P.F. and J.M. did the data acquisition. C.J.G., G.O. and M.F. did data analysis and interpretation of data. C.J.G., A.M., Y.K. and D.V.S. drafted the article. All authors revised it critically for intellectual content. All authors have given the final approval of the version submitted.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: C.J.G. and A.M. run a cadaveric airway skills workshop to teach emergency airway management to critical care clinicians.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data
The anonymised data sets generated and/or analysed during this study are available from the corresponding author.
Informed consent
Written consent was obtained from all the participants.
Ethical approval
Ethical approval for this study was obtained from the University of Melbourne research ethics committee (approval no. 2058001, dated 1 October 2020).