
Abstract
Introduction:
The data on short-term mortality among patients following interhospital transfers remain uncertain in the literature, and particularly in Turkey. The aim of this study was to determine the characteristics of interhospital transfer patients and to investigate the factors associated with 72-h mortality.
Methods:
All interhospital transfer patients aged 16 years and above from a secondary care public hospital were evaluated retrospectively for the period January to December 2018. A total of 34 variables, including age, gender, date of transfer, referring unit, diagnosis, reason for transfer, transfer destination, waiting and transfer time, vitals, the Glasgow Coma Scale, the presence of intubation, cardiopulmonary resuscitation before transfer, and the use of vasopressor medication, were included in the univariate analysis. The factors associated with short-term mortality were identified by multivariate regression analysis.
Results:
During the 1-year study period, 1216 interhospital transfers were performed. A total of 116 (9.5%) patients died within 72 h following interhospital transfer. Among all the transfers, the median age was 62 (interquartile range, 39–76) years. According to the multivariate analysis, vasopressor use (odds ratio, 3.55; 95% confidence interval: 1.32–9.52), age (odds ratio, 1.01; 95% confidence interval: 1.00–1.03), pulse (odds ratio, 1.01; 95% confidence interval: 1.00–1.02), and diastolic blood pressure (odds ratio, 0.97; 95% confidence interval: 0.95–0.99) were predictive of 72-h mortality following interhospital transfer.
Conclusion:
Nearly 10% of all the transfers from the secondary care public hospital resulted in mortality within 72 h. Vasopressor use, advanced age, lower diastolic blood pressure, and tachycardia were the most important factors associated with short-term mortality.
Introduction
Interhospital transfer (IHT) patients are one of the most vulnerable groups with fatal outcomes occurring frequently among critically ill patients. IHTs can become necessary for several reasons, including the absence of the relevant specialty or department, a lack of suitable beds, or the need for further treatment. In such cases, the treatment given at the first hospital may be inadequate or the patient follow-up may be provided under inappropriate conditions.
IHT status is independently associated with in-hospital mortality, and the incidence of mortality is higher among IHT patients compared with non-transferred patients.1,2 However, the prognostic factors for mortality vary among IHT patients. Male gender, admitting service, major diagnostic category, hypoxia on intensive care unit (ICU) arrival, and cardiac arrest prior to transfer have been reported as prognostic factors for patients transferred to the ICU.3,4 Furthermore, age, triage scale level, access block, and circulatory disease have been identified as factors influencing mortality in patients transferred from emergency department (ED) to ED. 5 Notwithstanding, there is insufficient literature, particularly in Turkey, on the predictors of short-term mortality among all IHT patients, not only those transferred to the ICU or ED.
This study therefore aimed to identify the prognostic factors for mortality occurring within 72 h following IHT among all transferred patients from a secondary care public hospital in Turkey.
Methods
Study design and settings
This retrospective cohort study was conducted between January 1 and December 31, 2018, in a secondary care public hospital in Turkey. The hospital is the largest facility in Nevşehir province with 180,850 ED visits and 21,663 hospital admissions (6297 from the ED) among patients aged 16 years and above in 2018.
When there is a need for an IHT, the responsible physician will give the necessary information to the general practitioner in charge of transfer in the emergency medical service (EMS) in the same province. The task of the practitioners is to locate the most appropriate hospital for the patient’s status in the province and, if unsuccessful, out-of-province hospitals. They perform this by checking the appropriate hospital beds via the electronic system, if appropriate, or by calling the relevant hospital units. When an appropriate hospital is found, the ambulance team from the referring hospital or EMS will undertake the patient transfer together with two emergency medical technicians or paramedics without any other medical staff (physicians or nurses).
All the transfers carried out from the secondary care public hospital have been recorded electronically and controlled monthly by a committee comprising physicians from different specialties in the hospital. Unnecessary transfers have been officially reported to the committee to reduce medical errors. These electronic transfer records used in this study included the patient ID, age, gender, date of transfer, referring unit, diagnosis, reason for transfer, transfer destination, waiting time in the first hospital, transfer time between hospitals, last vitals before the transfer process, the presence of intubation, and the Glasgow Coma Scale (GCS). The reasons for the transfer were the lack of beds in the ICU, the lack of relevant specialty, the lack of beds in the neonatal ICU, and further evaluation and treatment. Lack of relevant specialty was often seen in transfers caused by trauma. Thoracic, cardiovascular, and plastic surgeries were among these specialties.
In addition to these data, the application of cardiopulmonary resuscitation (CPR) before transfer and the use of vasopressor medication (dopamine and/or noradrenaline) before and during transfer were obtained from the hospital electronic records. Mortality information was tracked through the Central Civil Registration System.
All the transfer patients aged 16 years and above were included in the study; however, foreign patients were excluded because mortality information could not be followed. Ethical committee approval was obtained for the study.
Data analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 15 (IBM Corporation, Armonk, NY) and MedCalc® version 15.8 (MedCalc Software bvba, Ostend, Belgium). The continuous variables were presented as median values and interquartile ranges (IQRs), and the categorical variables were summarized as frequencies and percentages. The normality of the continuous variables was evaluated using the Kolmogorov–Smirnov test. The differences between the two groups of continuous variables were determined by the Mann–Whitney U test. The categorical variables were compared using Pearson’s χ2 or Fisher’s exact test. The odds ratios (ORs) were presented with 95% confidence intervals (95% CIs). A critical α value of 0.05 was accepted as statistically significant.
A binary logistic regression model was constructed to define the factors predicting short-term mortality within 72 h. The univariate model considered the patients’ demographic data, including age, GCS, vitals, waiting and transfer time, referring unit, diagnosis, reason for transfer, procedures, and the status of the out-of-province variables. Each variable was tested in the univariate model, and those comparisons that had a loose p-value of less than 0.1 were then tested in the multivariate model. Where there were less than 20 patients in a group and small groups overlapping with each other, these were not included in the analysis.
Results
During the year-long study period, 1216 transfers (96% of all transfers) were eligible for the study. Among these patients, 116 (9.5%) died within 72 h following IHT. The median age was 62 (interquartile range (IQR), 39–76) years, and 54% of the patients were males. The median transfer waiting time in the first hospital was 65 (IQR, 35–110) min, and the median transfer time between hospitals was 80 (IQR, 60–105) min. The referring unit rates were 82.6% for the ED, 15.6% for the wards, and 1.7% for the ICU. The most common transfer reason was a lack of beds in the ICU (56.3%) (Table 1).
Univariate analysis of the patients transferred to another hospital.
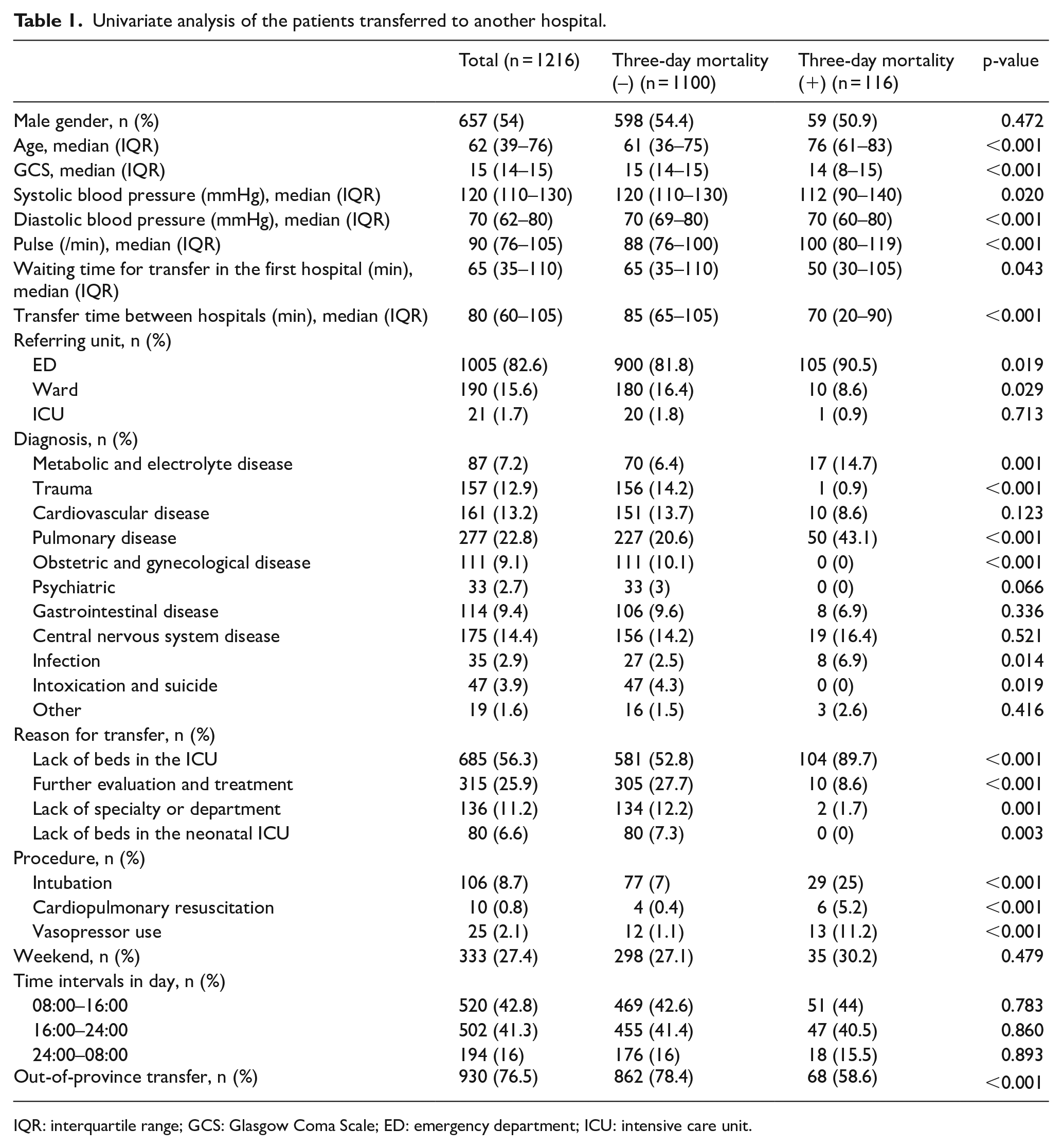
IQR: interquartile range; GCS: Glasgow Coma Scale; ED: emergency department; ICU: intensive care unit.
The short-term mortality group had a higher median age and lower median GCS value compared with the non-mortality group (median age and GCS: 76 years and 14 vs 61 years and 15, respectively, p < 0.001). The median systolic and diastolic blood pressures were lower and the median pulse higher in the mortality group than those in the non-mortality group (p < 0.05). The median transfer waiting time in the first hospital and the median transfer time between hospitals were higher in the non-mortality group compared with those of the mortality group (65 min and 85 min vs 50 min and 70 min, respectively, p < 0.05, Table 1).
The rate of transfer from the ED was higher in the mortality group than in the non-mortality group (90.5% vs 81.8%, respectively, p = 0.019), while the ward transfer rate was higher in the non-mortality group than in the mortality group (16.4% vs 8.6%, respectively, p = 0.029). The diagnostic rates of metabolic and electrolyte, pulmonary, and infectious diseases were higher in the mortality group, while the diagnostic rates of trauma, obstetric and gynecological diseases, and intoxication and suicide were higher in the non-mortality group (p < 0.05). The rates of intubation, CPR, and vasopressor procedures were higher in the mortality group than those in the non-mortality group (p < 0.001) (Table 1).
The multivariate regression analysis (Hosmer–Lemeshow test, p = 0.910) showed that vasopressor use (OR, 3.55; 95% CI: 1.32–9.52), advanced age (OR, 1.01; 95% CI: 1.00–1.03), tachycardia (OR, 1.01; 95% CI: 1.00–1.02), and lower diastolic blood pressure (OR, 0.97; 95% CI: 0.95–0.99) were predictive of mortality within 72 h following IHT (Table 2).
Multivariate analysis of patients with 3-day mortality after transfer.
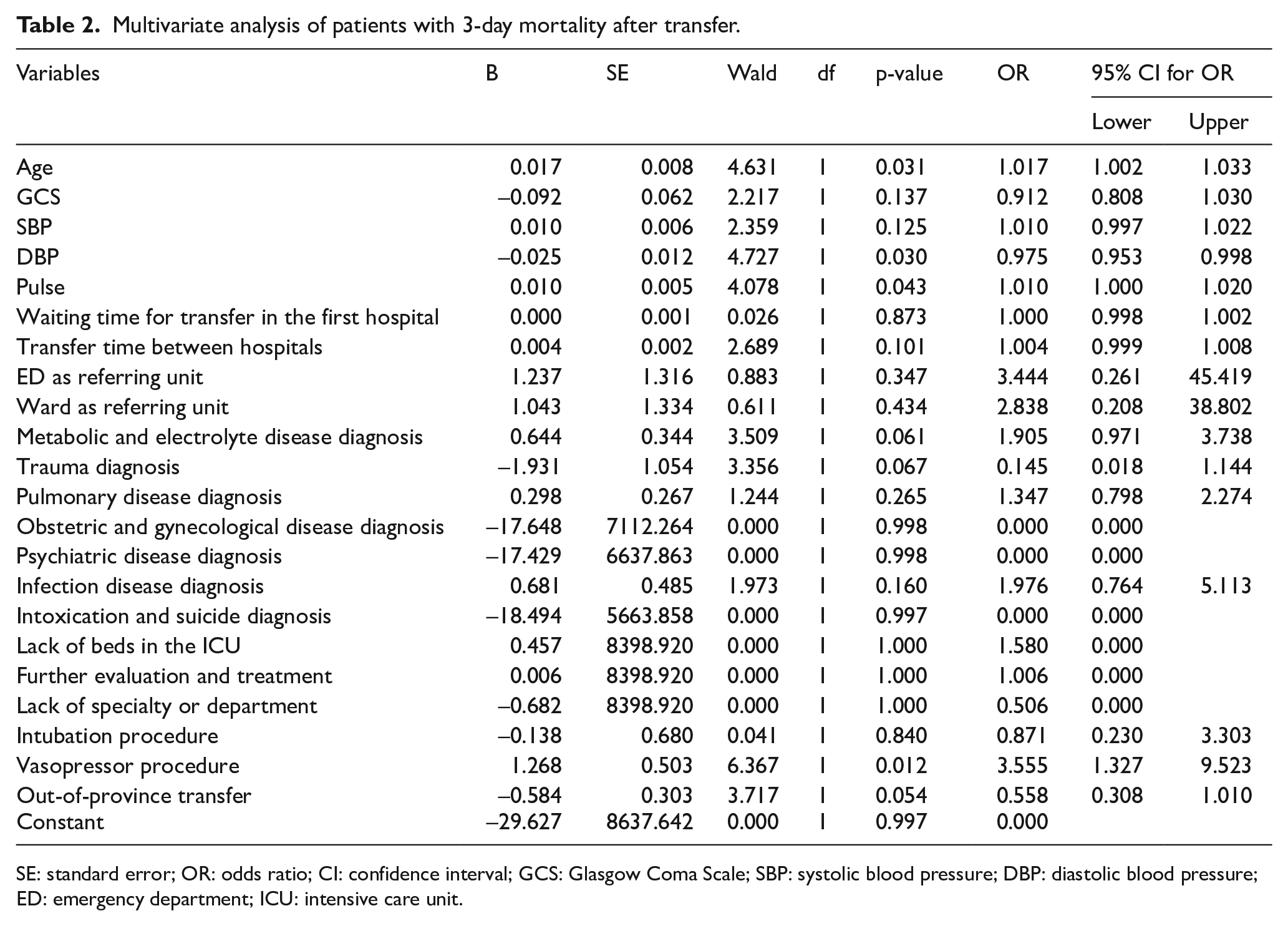
SE: standard error; OR: odds ratio; CI: confidence interval; GCS: Glasgow Coma Scale; SBP: systolic blood pressure; DBP: diastolic blood pressure; ED: emergency department; ICU: intensive care unit.
Discussion
The findings of this study revealed that 9.5% of all the transfer patients from a secondary care public hospital in Turkey died within 72 h of IHT. A study conducted in the Netherlands reported that the rate of 24-h mortality was 4.1% after IHT for intensive care patients transported using a mobile ICU. 6 On the contrary, the 24-h mortality rate in Korea was 1.5% for ED patients transported from other hospitals by ambulance, 7 while in Australia, 0.7% of ED-to-ED IHT patients died within 24 h. 5 In Saudi Arabia, the rate of in-hospital mortality was 30.4% among patients who had been transferred by paramedics, 8 and 3% of adult patients in the United States transferred to a tertiary care medical ICU died within 24 h after IHT. 4 The mortality rates between studies thus vary, and there are insufficient data in the literature for a comparison with the mortality rates found in this study.
In this study, the waiting time for transfer in the first hospital and the transfer time between hospitals were higher in the non-mortality group. This can be explained by the faster transfer of critically ill patients and a higher number of out-of-province transfers among the non-mortality group. The multivariate analysis showed that waiting and transfer times and out-of-province destinations were not associated with mortality within 72 h. Similarly, Durairaj et al. 3 reported that longer distance traveled (>60 miles) was an independent prognostic factor for overall mortality but not early mortality (<72 h).
Of all the transfers that resulted in mortality in this study, 90% were from the ED. The transfer rate from the ICU accounted for only 1.7% of all the transfers. In terms of diagnoses, metabolic and electrolyte, pulmonary, and infectious diseases were higher in the mortality group, while the diagnostic rates of trauma, obstetric and gynecological disease, and intoxication and suicide were higher in the non-mortality group. However, neither the referring unit nor the diagnoses were associated with mortality after the multivariate analysis. Durairaj et al. 3 showed that only neurological disease was an independent prognostic factor for early mortality in patients transferred to the medical ICU, while Mueller et al. reported their finding that the odds of 3-day mortality were significantly lower in transferred versus non-transferred patients aged 65 and above with stroke, acute myocardial infarction, sepsis, and respiratory diseases. On the contrary, transferred patients with gastrointestinal disease had significantly higher odds of 3-day mortality. 1 These divergent results may be due to the use of different study methodologies.
In this study, the multivariate regression analysis showed that only vasopressor use, advanced age, higher pulse, and lower diastolic blood pressure were predictive of mortality within 72 h following IHT. Alabdali et al. reported that higher age and a higher risk score for hemodynamics, arrhythmias, electrocardiogram monitoring, intravenous line, respiration, airway, respiratory support, GCS, and medication were associated with in-hospital mortality for patients transferred to the ICU. 8 Conversely, Durairaj et al. 3 showed that the independent prognostic factors for short-term mortality (<72 h) among patients transferred to the ICU included the highest diagnostic-related risk level, Charlson comorbidity score >3, insurance type, admitting service, and neurological disease. Meanwhile, Patel et al. identified a sequential organ failure assessment score of 12–16 on the day of IHT, an FiO2 level of 0.8–1.0 on ICU arrival, and cardiac arrest prior to transfer were associated with an increased risk for 24-h mortality after IHT in patients transferred to ICU. However, they did not establish any relationship between vasoactive drug use and mortality. 4 Gillman et al. 5 found that age, clinical change in Australasian triage scale level, access block, and circulatory disease were predictive for early death within 24 h of transfer among patients transferred from ED to ED. Finally, Visser et al. 9 reported that advanced age, cardiac problems as the principal reason for transfer, lower mean arterial blood pressure, and tachycardia on arrival at the destination hospital were associated with ICU mortality.
Most of the IHT studies in the literature addressed ED or ICU transfers, and no studies focused on short-term mortality following IHT in Turkey.10–12 It is clear that all the aforementioned studies focused on different variables because of the various risk scores used, referring unit settings, and local problems encountered. Nevertheless, the most common predictors for short-term mortality in these studies were poor hemodynamic status–vitals, and advanced age.
This study showed that 10% of all transfers from a secondary care public hospital in Turkey resulted in mortality within 72 h. Advanced age, lower diastolic blood pressure, tachycardia, and vasopressor use were identified as predictors for short-term mortality following IHT among all the transfer patients in this study. Both referring and receiving healthcare professionals should therefore pay attention to these mortality markers before, during, and after the transfer of patients.
Footnotes
Author contributions
N.B. and M.A.A. researched literature and conceived the study. N.B. was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. M.A.A. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
Data sharing is not applicable to this article as no data sets were generated or analyzed during the current study.
Informed consent
Written informed consent was obtained from all subjects before the study.
Ethical approval
Ethical approval for this study was waived by Nevşehir Hacı Bektaş Veli Üniversitesi Ethics Committee (Approval Number: 2018.15.180). This study was completed in accordance with the Helsinki Declaration.
Trial registration
This clinical trial was not registered because registration failed yet.