
Abstract
Objective:
We aimed to investigate the prevalence and prognostic value of malnutrition assessed by Controlling Nutritional Status score in community-acquired pneumonia patients.
Methods:
All adult patients admitted to our emergency department and hospitalized for community-acquired pneumonia were prospectively followed-up until hospital discharge or death. Nutritional status was assessed with the Controlling Nutritional Status score, which is based on serum albumin levels, total cholesterol levels, and lymphocyte counts. The primary study endpoint was complicated hospital course defined as need for mechanical ventilation, mortality, or intensive care unit admission.
Results:
Three hundred and five patients (mean age 68.6 ± 11.2 years and 51.8% female) were enrolled, and 40 patients (13.1%) had complicated hospitalizations. Older patients, patients with more comorbidities, and patients with higher Controlling Nutritional Status scores on admission were tended to have a higher rate of complications during their hospitalization. Multivariate analysis showed that older age (odds ratio 2.55, 95% confidence interval 1.41–4.64, p < 0.001), presence of diabetes (odds ratio 1.54; 95% confidence interval 1.09–3.65; p = 0.004), pneumonia severity index ⩾ 3 (odds ratio 1.27, 95% confidence interval 0.524–3.725, p = 0.035), and Controlling Nutritional Status score > 4 (odds ratio 2.23, 95% confidence interval 1.129–3.657, p = 0.001) were independent predictors of complicated hospitalizations.
Conclusion:
Malnutrition determined by Controlling Nutritional Status score predicts complications in hospitalized patients with community-acquired pneumonia.
Introduction
Community-acquired pneumonia (CAP) is an important cause of hospitalization, and healthcare expenditure worldwide. 1 Several risk factors such as older age, male gender, and higher burden of comorbid diseases are known to be associated with complications and mortality in CAP patients.1–3 It is also known that the complication and mortality rates are low in CAP patients treated as outpatients, but are higher among patients hospitalized for CAP.1–3 Numerous scoring systems have been developed to predict adverse events in CAP patients.4,5 However, most of these scores have some limitations and therefore new prognostic markers are needed.
Nutritional condition, which reflects patients’ health status, has emerged as a prognostic factor in patients with various diseases like heart failure, 6 diabetes mellitus, 7 and malignant tumors. 8 However, only a few studies have evaluated the significance of malnutrition in patients with CAP.9,10 While several tools for assessing nutritional status have been evaluated in different conditions, most of these tools are difficult to use in daily practice due to their complexity. However, the Controlling Nutritional Status (CONUT) score can be easily calculated with parameters (serum albumin, total cholesterol concentrations, and total lymphocyte count) which may routinely evaluated in laboratory tests during emergency department (ED) evaluation. 11 The CONUT score was first examined for the detection hospital malnutrition in 2005. 11 Following its first definition, the utility of the CONUT score in predicting prognosis have been generally reported in specific types of surgeries and only in a variety of specific surgical populations such as patients with gastric cancer, 12 lung adenocarcinoma, 13 or urinary tract cancer. 14 Although the prognostic value of CONUT score have been investigated in patients other than the surgical populations such as acute ischemic stroke 15 and heart failure 16 in recent studies, there has been no study evaluating the significance of CONUT score in predicting outcomes in patients with CAP. Hence, we aimed to investigate the significance of admission nutritional status evaluated by CONUT score in patients with CAP.
Methods
Study design and patients
In this prospective and single-center study, all consecutive CAP patients requiring hospitalization who were aged 18 years or older, and admitted to ED were included between March 2016 and March 2017 at Muğla University Hospital (Muğla, Turkey). All patients were diagnosed and treated according to the current guidelines for the management of CAP in adults,17,18 and they were followed up during hospitalization or until death. Patients younger than 18 years, patients with healthcare-associated pneumonia, patients with incomplete laboratory or follow-up data, and patients who were not hospitalized were excluded. Patients who have potential factors that affect inflammation-based and nutritional markers such as active tuberculosis, patients undergoing chronic dialysis, pregnant women, and immunocompromised patients were also excluded.
The CAP is defined as pneumonia acquired outside of a healthcare setting. This study was approved by the Muğla University Ethics Committee, and all patients or their relatives gave informed written consent.
Measurements
Patients’ demographic and clinical characteristics, vital signs, laboratory data, and radiological findings at the presentation to the ED were collected. Complete blood count and routine biochemical analyses including cholesterol levels were measured within the first 24 h of admission. Severity of pneumonia was assessed by the pneumonia severity index (PSI) and CURB-65 score as previously described.4,5
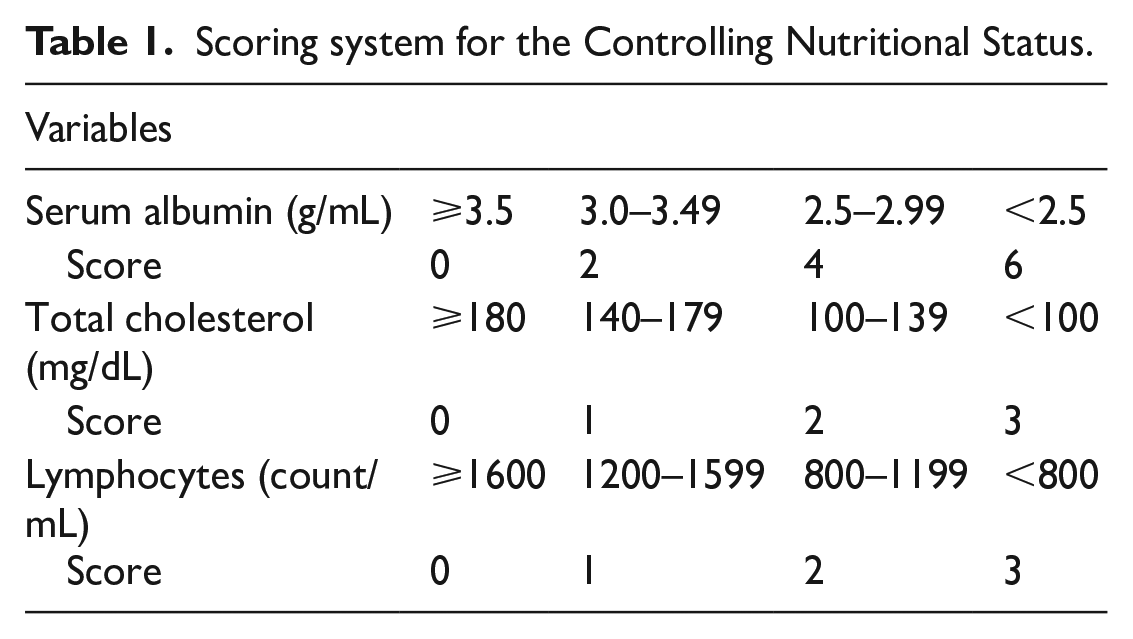
The CONUT score was calculated by serum albumin level, total cholesterol level, and lymphocyte counts (Table 1). Patients were classified according to the CONUT score as normal nutritional status (CONUT 0–1 points), mild malnutrition (CONUT score 2–4 points), and moderate-to-severe malnutrition (CONUT score ⩾ 5 points).
Scoring system for the Controlling Nutritional Status.
Study endpoints
The primary outcome of the study was complicated hospitalization: mortality during hospitalization, need for mechanical ventilation, or need for intensive care unit admission. The secondary outcome of interest was the length of stay in hospital.
Statistical analysis
Data were analyzed using SPSS for Windows (version 24; SPSS Inc., Chicago, IL, USA). Comparison of patients characteristics in two groups (patients with and without complicated hospitalization) was done by chi-square test. Distribution of the analyzed continuous variables for normality was tested with the Kolmogorov–Smirnov test. Univariable and multivariable analyses with Cox proportional hazard regression were used to determine significant predictors of complicated hospitalizations. The variables listed in Table 2 are included in the Cox models except for albumin, cholesterol, and lymphocyte counts, which are included in the CONUT score. The receiver operating characteristic (ROC) curve was used to identify the optimal cut-off point of the CONUT score for the outcome.
Comparison of patients with and without complicated hospitalizations.
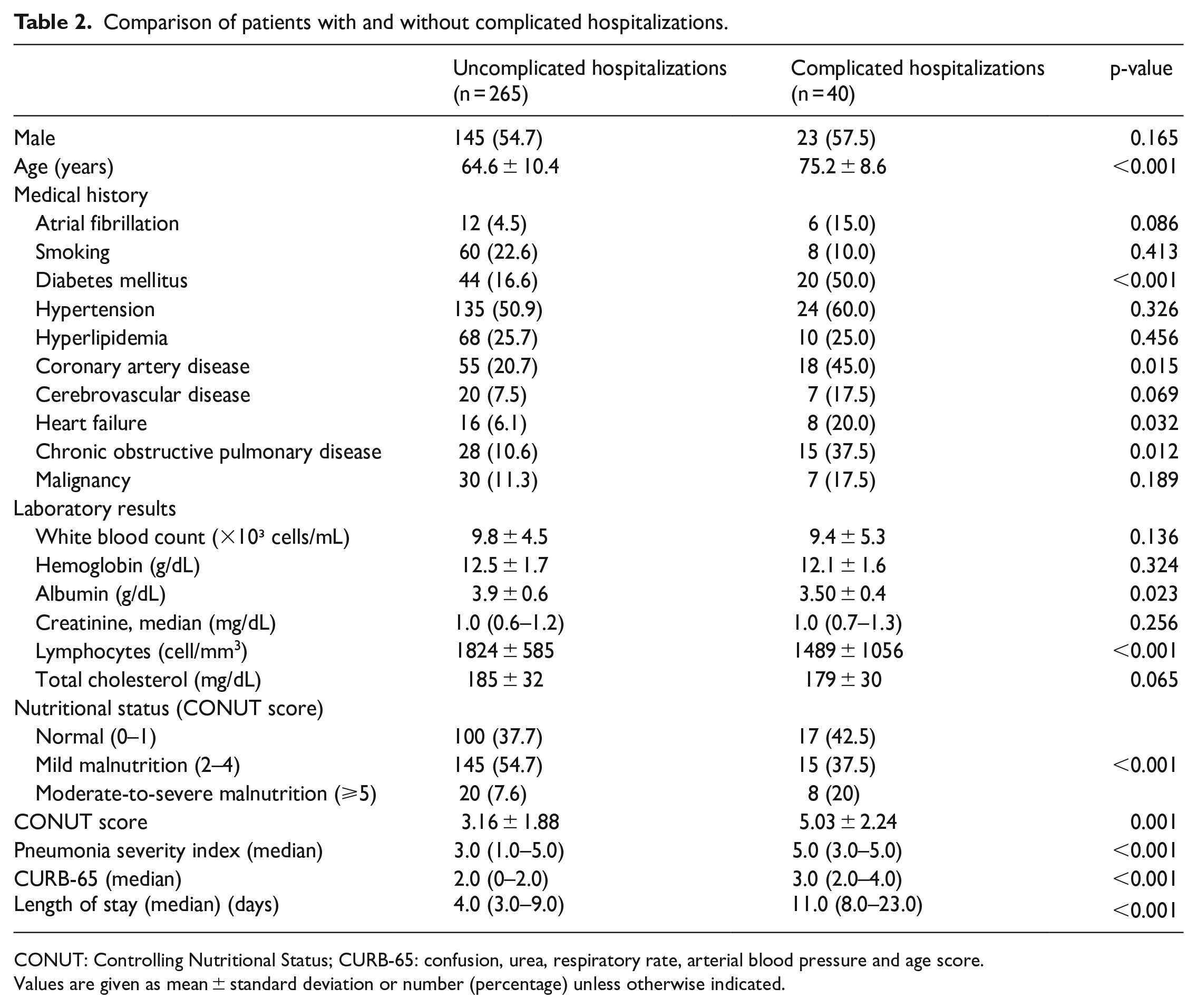
CONUT: Controlling Nutritional Status; CURB-65: confusion, urea, respiratory rate, arterial blood pressure and age score.
Values are given as mean ± standard deviation or number (percentage) unless otherwise indicated.
The sample size was estimated at 200 patients, with a power of 80%, and a two-tailed alpha error of 0.05. For all tests, a p-value < 0.05 was considered statistically significant.
Results
During the study period, a total of 720 adult patients admitted to our ED with a diagnosis of CAP. However, 30 patients were excluded because of incomplete data; 64 patients were excluded due to immunocompromised diseases, hospital-acquired pneumonia, or active tuberculosis; 26 patients were excluded due to chronic dialysis; and 295 patients were excluded due to ambulatory treatment (Figure 1). Therefore, a total of 305 patients (mean age 68.6 ± 11.2 years, and 51.8% female) were finally analyzed in the study.
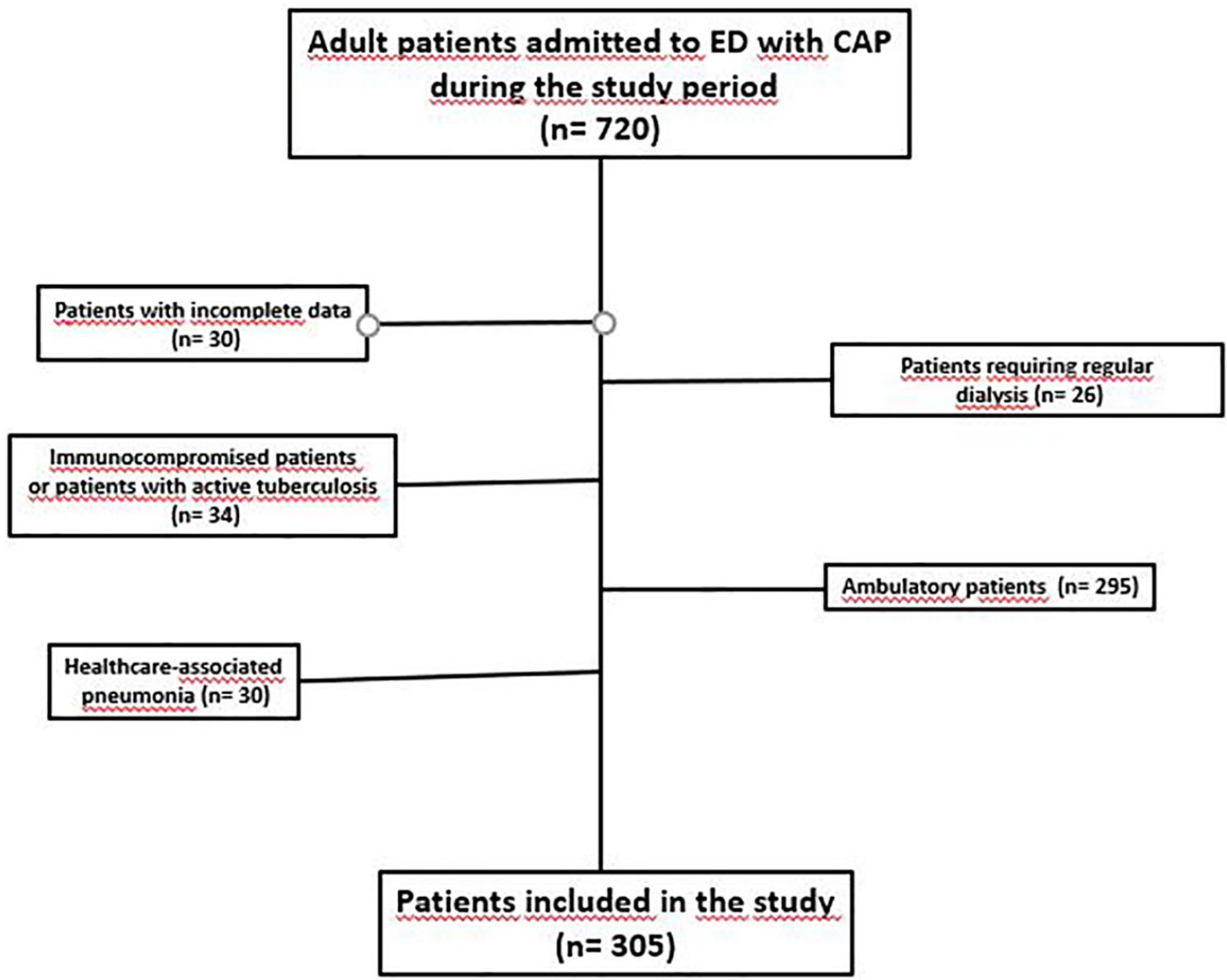
Flowchart of patients including exclusion criteria.
Complicated hospitalizations
Forty patients (13.1%) experienced 61 episodes of complicated hospitalizations. Nine patients (2.9%) died, 20 patients (6.6%) required mechanical ventilation, and 32 patients (10.5%) treated in intensive care units during the study period.
Compared to patients without complications, patients with complicated hospital course were older, were more likely to have comorbid diseases, had significantly lower albumin levels, and lymphocyte counts on admission (Table 2).
Of the study population, 117 (38.3%) patients had normal nutritional status, 160 (52.5%) patients had mild malnutrition, and 28 (9.2%) patients had moderate/severe malnutrition according to their CONUT scores. Patients with complicated hospitalization had higher CONUT scores on admission than the patients without complications (5.03 ± 2.24 vs 3.16 ± 1.88, respectively; p = 0.001).
Length of stay
Patients with complicated hospitalization had longer length of stay compared to uncomplicated patients (median values of 11 vs 4 days, respectively; p < 0.001). Compared to patients with CONUT score ⩽ 4, length of hospital stay was longer for patients who had CONUT score > 4 (median value of 6 vs 10 days, respectively; p = 0.01).
Predictors of outcomes in CAP
Multivariate analysis showed that older age (odds ratio (OR) 2.55, 95% confidence interval (CI) 1.41–4.64, p < 0.001), presence of diabetes (OR 1.54; 95% CI 1.09–3.65; p = 0.004), PSI ⩾ 3 (OR 1.27, 95% CI 0.524–3.725, p = 0.035), and CONUT score > 4 (OR 2.23, 95% CI 1.129–3.657, p = 0.001) were independent predictors of complicated hospitalizations (Table 3). In the ROC curve analysis, when complicated hospitalizations was used as an endpoint, the area under the curve of the CONUT score was 0.8476 (95% CI 0.725–0912, p < 0.001) (Figure 2).
Multivariate analysis for the prediction of complicated hospitalizations.
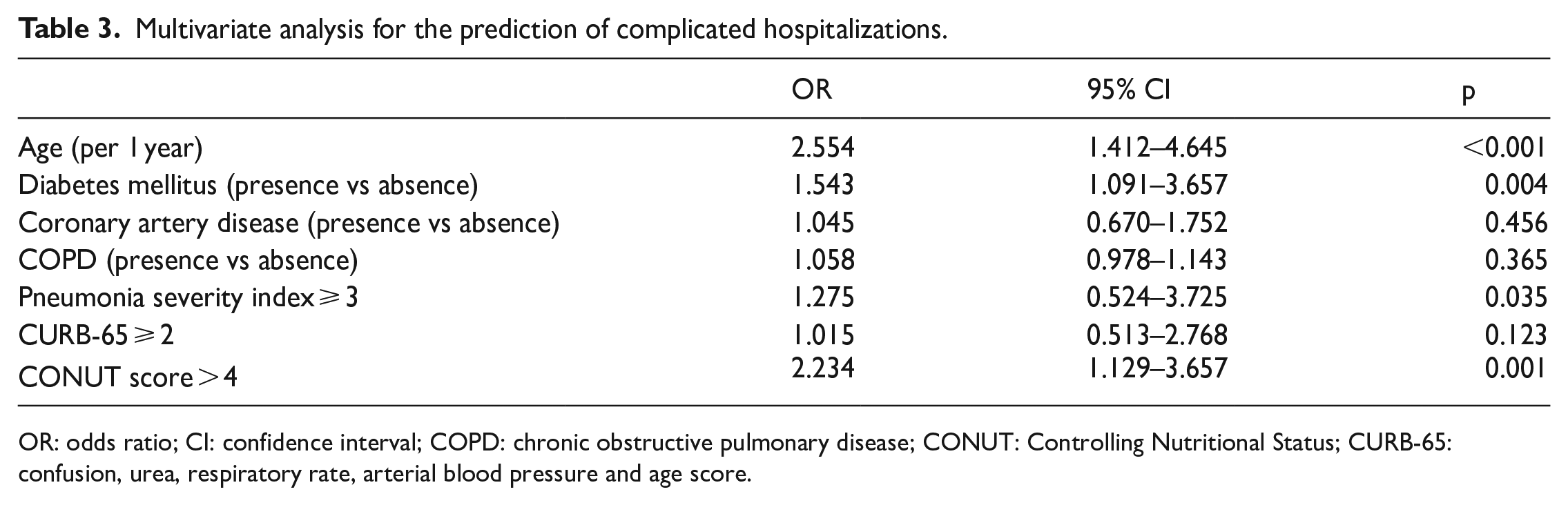
OR: odds ratio; CI: confidence interval; COPD: chronic obstructive pulmonary disease; CONUT: Controlling Nutritional Status; CURB-65: confusion, urea, respiratory rate, arterial blood pressure and age score.
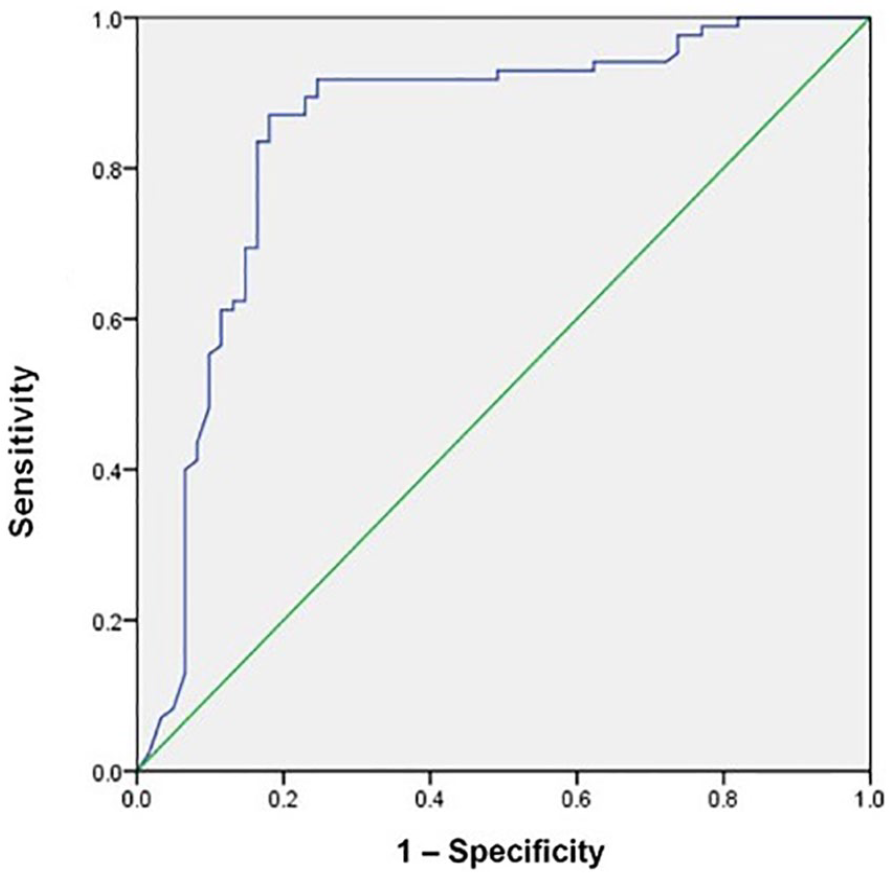
Receiver operating characteristic curve for CONUT score. The area under the receiver operating characteristic curve (AUC) was 0.8476.
Discussion
In this study, 61.7% of the hospitalized adult patients with CAP were determined to have malnutrition (52.5% mild malnutrition, and 9.2% moderate-to-severe malnutrition) according to their CONUT scores. Our results also demonstrated that nutritional status assessed by CONUT score predicts complications in hospitalized CAP patients.
Malnutrition is frequently determined and is associated with adverse events and prolonged length of stay in hospitalized patients with various diseases.19,20 Malnutrition has been identified with several screening tools in the previous studies,20–22 but no nutritional screening tool has been validated in CAP patients. Therefore, the prevalence and importance of malnutrition are not clear for this population. In a Korean study, Yeo et al. 10 retrospectively examined 198 CAP patients aged ⩾ 18 years. The prevalence of malnutrition was 39.4%, and the presence of malnutrition was associated with long-term mortality in patients with CAP. 10 In another study, malnutrition was assessed by subjective global assessment tool and mini-nutritional screening score among elderly (aged ⩾ 60 years) CAP patients. 23 This study showed that malnutrition was associated a higher risk for a more severe disease. 23 Akuzawa and Naito 24 enrolled 57 pneumococcal CAP patients in a retrospective study to investigate the association between markers of malnutrition and the severity of CAP. This study revealed a negative correlation between the serum albumin and cholinesterase levels and the length of stay. 24
Hypoalbuminemia has been used as a marker of malnutrition in CAP patients. 25 However, the evidence from previous studies is controversial, as some studies have suggested that malnutrition would be underdiagnosed when using hypoalbuminemia as the sole criterion.26,27 The CONUT score is a simple marker of malnutrition; however, it is not only a marker of nutritional status but also reflective of immunologic status as it contains lymphocyte and albumin levels in the same formula.
The CONUT score is a simple marker of malnutrition; however, it is not only a marker of nutritional status but also reflective of immunologic status as it contains lymphocyte and albumin levels in the same formula.
Usage of the total lymphocyte count, serum albumin, and total cholesterol concentration enables CONUT score to evaluate the immunologic status, the protein reserves, and the calorie depletion, respectively. However, the prognostic impact of CONUT score has been evaluated mostly among surgical patients,12–14 and to our knowledge, its relation to adverse events have never been described in patients with CAP.
Our results suggest that the impaired immuno-nutritional status, determined by higher CONUT score, may result in prolonged length of stay and poorer prognosis in adult patients with CAP.
Study limitations
The follow-up studies were not performed after hospital discharge in our study. We also lack information about detailed dietary intake during hospitalization. We included only adult hospitalized patients in this single-center study. Therefore, further studies are needed to elucidate the value of CONUT score in patients with CAP.
Conclusion
This is the first study examining the applicability of CONUT score in assessing malnutrition among CAP patients. Our results showed that 61.7% of the CAP patients had moderate-to-severe malnutrition on admission. We also showed that CAP patients with higher CONUT scores were more likely to exhibit higher rates of complications and more likely to have longer length of stay.
Footnotes
Authorship
Birdal Yıldırım, MD, Associate Professor, Faculty of Medicine, Department of Emergency Medicine, Muğla Sıtkı Koçman University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
305 cases, present.
Ethical approval
Ethical approval received.
Informed consent
Permission for informed consent was obtained from all cases.
Human rights
Respectful to human rights.