
Abstract
A 60-year-old hypertensive lady experienced painless sudden visual loss in the right eye when resting at home. There was no traumatic injury, no eye pain, or flashes or floaters, or nausea, but mild right-sided headache for few days. She was not lifting heavy objects, nor straining. She managed to attend the emergency department within 1 h of onset of symptoms by herself walking into the consultation room unaided. Examination showed visual acuity with pinhole of hand movement over the right eye, right relative afferent pupillary defect and normal intraocular pressure of 15 mmHg. Extraocular movement was full without diplopia or pain. Eyes were not injected, and slit lamp examination was normal with clear cornea. Acute management of vascular causes of acute blindness and the role of hyperbaric oxygen therapy in ophthalmological disease in Hong Kong will be discussed.
Keywords
Questions
What were the fundoscopy (Figure 1) findings?
What types of acute management could you offer?
What further clinical history, physical examinations and blood test would you perform in this case?
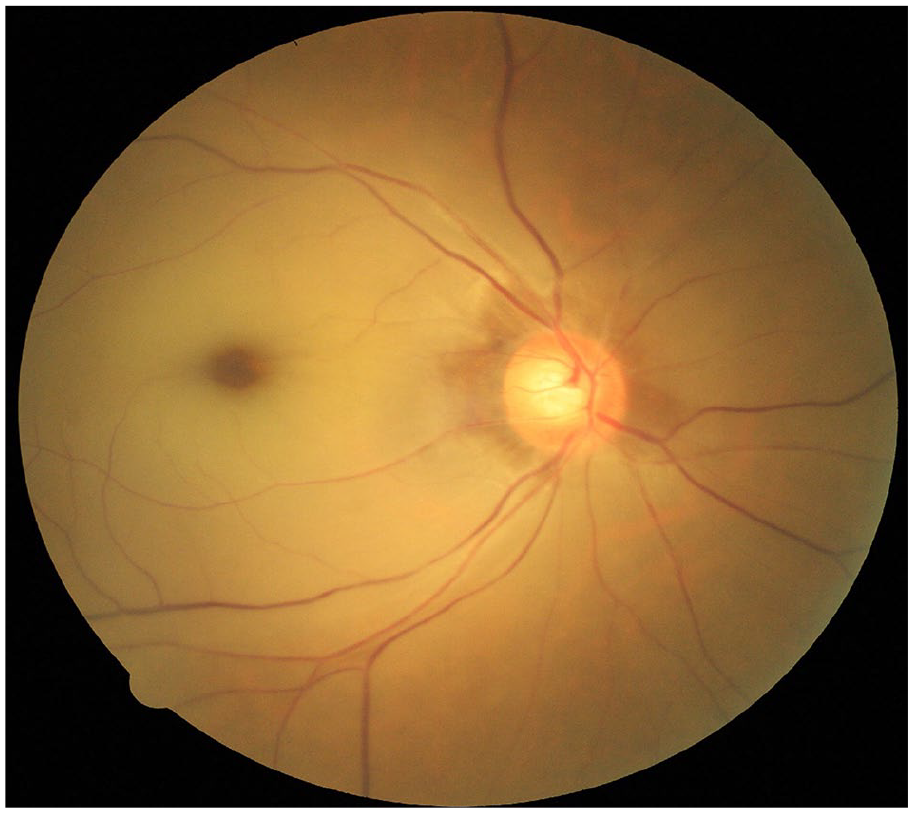
Right eye fundus photo showing generalized pallor from retinal oedema, with a typical cherry-red spot over the fovea. Retinal arterioles were attenuated.
Answers
The right retina showed generalized pallor, with a typical cherry-red spot over the fovea. Retinal arterioles were attenuated, and there were no emboli identified along the arteriole. Optic disc was not swollen, and there were no retinal haemorrhages seen. The clinical diagnosis was right eye central retinal artery occlusion (CRAO). (Remarks: With a relative afferent pupillary defect, direct ophthalmoscope examination of the right eye was easier than normal cases even without mydriatic eye drop.)
The patient should be instructed to breathe over a paper bag or inhale carbogen if available. Ocular massage should be done by repeatedly pressing and releasing pressure over the right eyeball. Topical anti-glaucoma medications should be given despite normal intraocular pressure, and intravenous acetazolamide could also be given.
The differential diagnosis was CRAO alone, or occlusion at a more proximal level at ophthalmic artery or internal carotid artery. Aetiology was thromboembolic causes, internal carotid artery dissection, space-occupying lesion or vasculitis. Giant cell arteritis (GCA), despite being uncommon in Chinese, is one of the differential diagnosis, given the patient was aged >50 years with new-onset headache. History of recent neck massage, neck trauma, previous minor stroke episode, amaurosis fugax, palpitation or vasculitis elsewhere in the body should be explored, as they are possible risk factors. Jaw claudication and scalp tenderness, being criteria for diagnosis of GCA, should be asked. Temporal artery should be palpated for the presence of pulsation or tenderness. Pulse should be checked for any arrhythmia, and neck should be auscultated for any carotid bruit. Blood for erythrocyte sedimentation rate (ESR) could be ordered if GCA is suspected, but should not preclude the high-dose systemic steroid salvage treatment.
Discussion
This patient suffered from right eye CRAO, and giant cell arteritis diagnostic criteria were not met. Her home was well ventilated, and there was no fire at home to suggest carbon monoxide poisoning. She was not a drinker and did not consume methanol, quinine or dapsone before the incident. There was no history of recent neck massage or sprain injury. Temporal pulse was strong and of normal rhythm, and there was no carotid bruit. Limbs, jerks and gait were normal, and physical examinations did not illicit any focal neurological signs to suggest cerebral stroke. Ocular massage was done for 15 min, and intraocular pressure (IOP) lowering drugs (topical beta-blocker, timolol eye drop 1 drop every 5 min; and systemic carbonic anhydrase inhibitor, oral 500 mg acetazolamide tablet stat once) were given. However, both were not successful to reverse the situation. The patient was then referred to our hospital’s Hyperbaric Oxygen Therapy (HBOT) centre for further treatment.
CRAO is an ocular emergency diagnosed clinically by history and ophthalmoscopy. Typical cherry-red spot over the central macula is a result of retinal ischaemia, causing perifoveal inner retinal oedema that outlines the very thin fovea at centre as red or orange in colour. Mimics of cherry-red spot can be seen in the case of macular commotio from blunt ocular trauma; and chemical poisoning such as carbon monoxide, methanol, quinine and dapsone. Occasionally, multiple emboli along the arteriole can be seen as the ‘cattle-trucking’ or ‘box-carring’ sign, whereas the commonest yellowish cholesterol emboli are called Hollenhorst plaque. 1
Other than those acute managements mentioned above, breathing over a paper bag or inhalation of carbogen is also recommended. It aims to increase the carbon dioxide level that patients breathe in, inducing vasodilation of the retinal arteriole. In contrast, anti-glaucoma medications work by lowering IOP, reducing the perfusion resistance of retinal arteries. Both measures attempt to flush away the intra-arterial emboli downstream. 2 Other than pharmacological treatment, ocular massage, which produces a fluctuating pressure within the globe, might mechanically help the emboli to migrate distally. Distalization of the emboli aims to convert a CRAO to branch retinal artery occlusion, hoping to salvage the central retina before irreversible damage occurs at around 97–240 min after the insult, 1 thus preserving useful central vision. However, caution on acetazolamide usage warrants attention, as it is contraindicated in sulphur or sulfonamide allergy patients. 3 Other than acetazolamide, mannitol could be a drug of choice, yet caution should be paid on precipitating heart failure in elderly. HBOT serves as the last resort given its availability in Hong Kong. 4 The treatment protocol is of 2.4 atmosphere absolute (ATA), which is different from those for carbon monoxide poisoning or decompression sickness. All in all, despite all the measures available, none of them stands out to be proven with good efficacy. 5
Causes of CRAO include dislodged emboli or secondary to underlying diseases such as GCA, systemic lupus, coagulation disorder, internal carotid artery dissection, orbital fracture’s bony fragment impingement and retrobulbar mass. Ophthalmology consultation is essential, and further workup on aetiology guides management plan. Differentiating the level of arterial occlusion is important, as HBOT works only for CRAO, but not ophthalmic artery occlusion. HBOT relies on the choroidal circulation to diffuse oxygen to the ischaemic retina (Supplemental Figure 2). The choroidal arteries are supplied by the posterior ciliary arteries, which branch from the ophthalmic artery. If the occlusion is over the ophthalmic artery, HBOT has no means to reperfuse the retinal ischaemia through the choroidal circulation. 6
Supplemental Material
Fig_2_FFA – Supplemental material for An old lady with acute headache and sudden blindness
Supplemental material, Fig_2_FFA for An old lady with acute headache and sudden blindness by Sunny Chi Lik Au and Simon Tak Chuen Ko in Hong Kong Journal of Emergency Medicine
Footnotes
Author contributions
S.C.L.A. contributed to the concept and design of study, acquisition of image and drafting the article. S.T.C.K. was involved in revising the article critically for important intellectual content and gave final approval of the version to be published
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.