
Abstract
Exsanguinating neck injury is a rare presentation to the emergency department. However, when such a scenario occurs, emergency physicians should be able to readily employ the various methods available to control the exsanguination. Furthermore, the application of inotrope or vasopressor in a hypotensive traumatic patient despite aggressive fluid/blood product resuscitation is explored.
Case
A 43-year-old male was found unconscious on the street with a pair of scissors loosely over his exsanguinating neck wound. The ambulance crew administered fluid bolus and attempted bleeding control by direct compression over the neck wound (Photo 1) upon arrival. The patient developed witnessed cardiac arrest on arrival to the emergency department (ED) of a secondary hospital (with no trauma call activation available) with initial cardiac rhythm being pulseless electrical activity. Cardiopulmonary resuscitation (CPR) was immediately initiated. Fluid resuscitation was continued. Neck wound bleeding was controlled by manual external compression. Airway was secured with endotracheal tube intubation. Return of spontaneous circulation (ROSC) with sinus rhythm was achieved after 30 min of cardiac arrest. Bedside ultrasound showed reduced cardiac contractility and a flat and distensible inferior vena cava (IVC). However, he remained hypotensive (blood pressure 59/58) at the ED despite aggressive fluid resuscitation with 4.5 L of normal saline and 4 units of unmatched packed cells. Adrenaline infusion via femoral central venous catheter was started to achieve a systolic blood pressure of 80–90 mmHg. The patient was transferred to a trauma center for direct emergency operation by head and neck surgeons. Repair of the right common carotid artery (CCA) failed intraoperatively. Instead, damage control was achieved with transection and ligation of the right CCA. Post-operatively, his Glasgow Coma Score was 3 all along and blood pressure was persistently low with vasopressor. Angiography showed cross-flow to the right hemisphere, and serial computed tomography of the brain demonstrated increasing cerebral edema. The patient was finally certified brain dead on post-operative day 5.

Exsanguinating neck wound.
Questions
Describe the injury. What structures are at risk of damage?
What mechanical methods can be employed to stop the bleeding?
Should vasopressors or inotropes be given in case of hypotension despite massive transfusion during secondary transfer to a trauma unit?
Answers
Penetrating neck injury with airway compromise and hemodynamic instability. The structures damaged in this patient were right CCA, right and part of left sternocleidomastoid muscles, right internal jugular vein, right vagus nerve, pharynx, and thyroid cartilage.
The initial method to control the bleeding is simple external compression on the wound. Wound packing is an alternative. Specific to penetrating neck injuries, Foley balloon catheter tamponade (Picture 1) can be used for bleeding that is not amenable to control through simple external compression. It involves introducing the Foley catheter into the wound, following the wound track and inflating the balloon with 10–15 mL of water until resistance is met. The catheter is then clamped and the neck wound is sutured. 1 A number of topical hemorrhage control agents are being developed, but they require further study before widespread use in civilian populations. If bleeding is still not amenable by the measures above and no surgeon is available, the emergency clinician may have no choice but to attempt to explore the wound and control bleeding by other means (e.g. placing a clamp).
Yes and no.
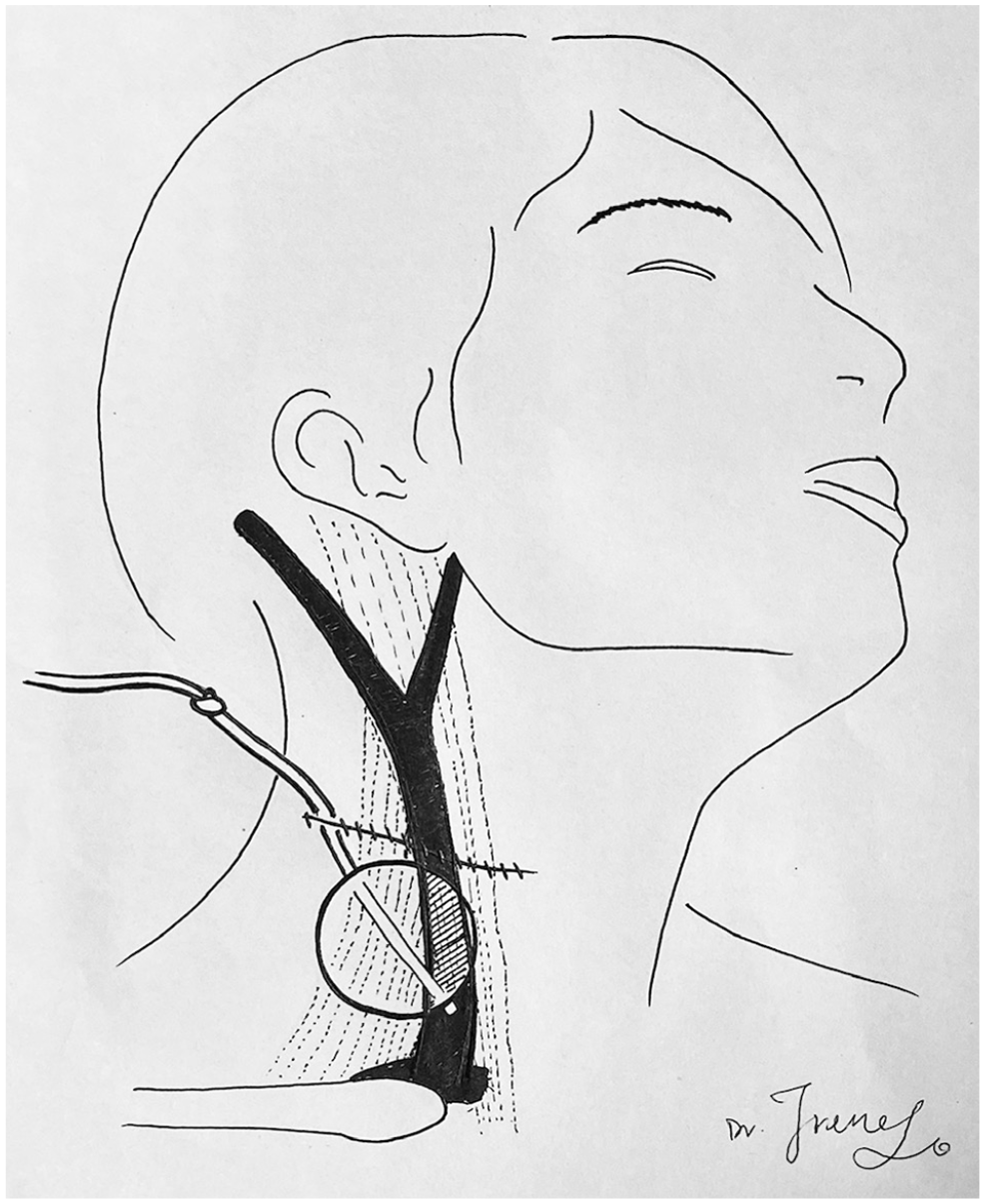
Foley catheter balloon tamponade in a neck injury. The catheter is knotted on itself acting as a clamp to prevent blood flow through the lumen. The wound is sutured around the catheter.
Up to date, no clinical studies have validated any vasopressor support for the management of hemorrhagic shock. Early use is generally not recommended according to the European guideline on management of major bleeding and coagulopathy following trauma 2 and Advanced Trauma Life Support (ATLS). This should also be tempered by the risk of excessive vasoconstriction during such hypovolemic state. Nevertheless, the administration of vasopressors in trauma resuscitation is a common practice in some trauma centers. 3 The initiation of vasopressor therapy may have usefulness in restoring hemodynamic parameters and vital organ perfusion, thereby reducing the need for aggressive fluid therapy, minimizing dilutional coagulopathy, and preventing circulatory collapse. Furthermore, inotropic agent infusion of dobutamine or epinephrine may be helpful in the presence of myocardial dysfunction, which often occurs in those trauma patients with pericardial effusion, cardiac contusion, or secondary to brain injury. 2
Discussion
Overview of topical hemostatic agents
The two main categories of topical hemostatic agents are physical agents, which promote hemostasis using a passive substrate, and biologically active agents, which enhance coagulation at the bleeding site (Photo 2). Physical agents promote hemostasis through several effects. The matrix material provides a stimulus that activates platelets and extrinsic pathway, and a scaffold for thrombus deposition. The dry matrix also absorbs water, concentrates hemostatic factors at the site of bleeding, and tamponades bleeding vessels by exerting pressure. Examples include bone wax and putty, dry matrix, and external agents (HemCon bandage, ChitoFlex, QuikClot). On the contrary, biologically active agents or procoagulant supplementors augment hemostasis. Examples include topical thrombin, fibrin sealant, and tranexamic acid. The choice of topical hemostatic agents depends on the amount and location of bleeding, and the availability and cost of an agent. Biologically active agents are more useful for brisk bleeding compared with dry matrix agents and are more effective in the setting of coagulopathy. For pulsatile external exsanguinating hemorrhage, it is recommended to pack with dry fibrin sealant dressing. 4
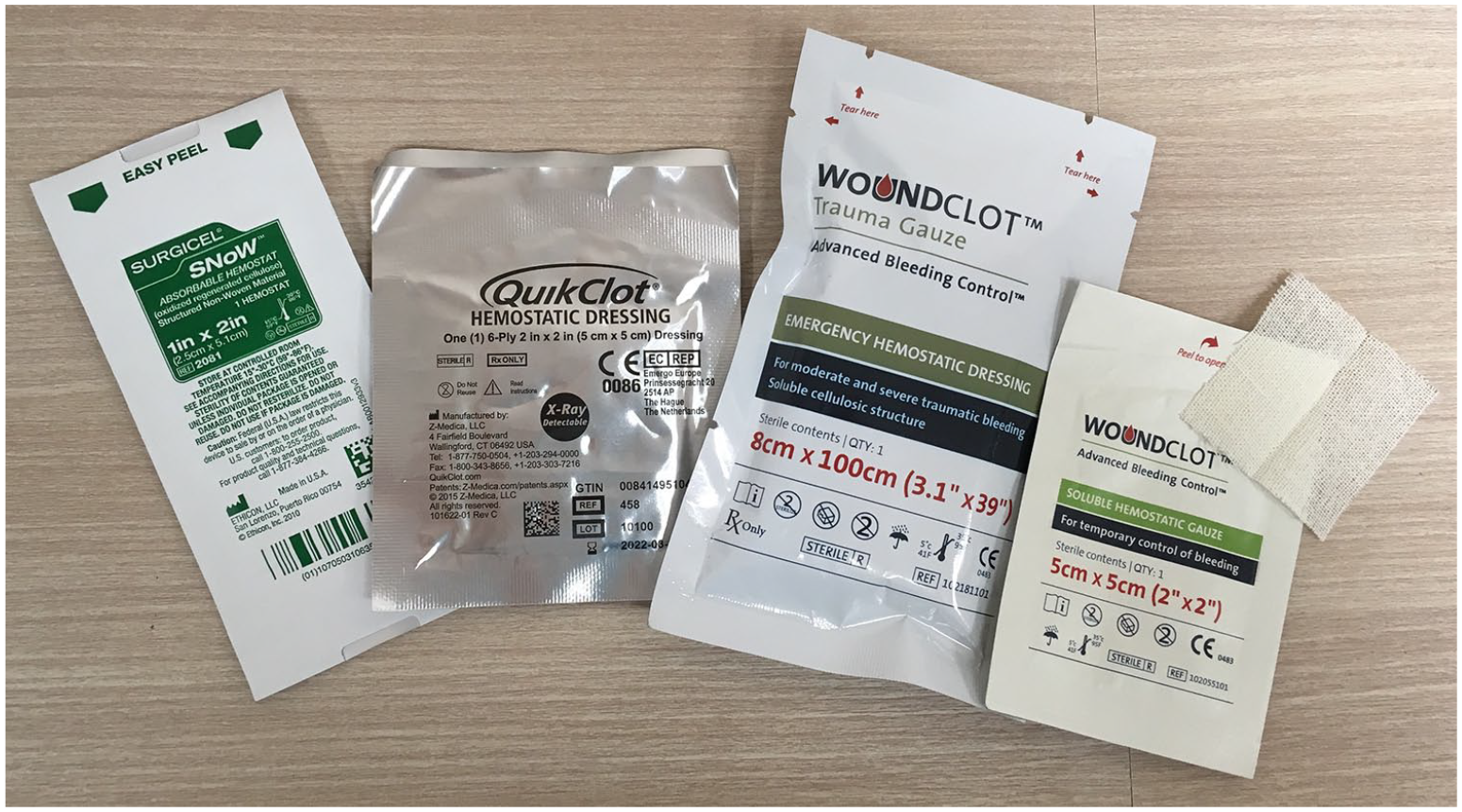
Examples of topical hemostatic agents available in the ED.
Use of vasopressors and inotropes in hemorrhagic shock in trauma
The use of vasopressors and inotropes in hemorrhagic shock in trauma is controversial. Generally, vasopressors are contraindicated in the early management of hemorrhagic shock, due to their deleterious consequences.5,6 Vasopressors like vasopressin, in the absence of adequate volume resuscitation, are shown to worsen the outcome by increasing mortality.7,8 Treatment of hypovolemic (hemorrhagic) shock requires correction of inadequate organ perfusion by increasing organ blood flow and tissue oxygenation. Increasing blood flow requires an increase in cardiac output. The formula MAP = CO × TPR states that the mean arterial pressure (MAP) is proportional to cardiac output (CO) and total peripheral resistance (TPR). An increase in blood pressure should not be equated with a concomitant increase in cardiac output or the recovery from shock. An increase in peripheral resistance (e.g. with vasopressor therapy) with no change in cardiac output results in increased blood pressure, but no improvement in the tissue perfusion or oxygenation. However, in many trauma situations, their use may be required to salvage a severely injured critical patient. In a few trauma centers, administration of vasopressors is a common practice. 3 In the presence of insufficient vasoconstrictive response or vasoplegia, it may be justified to use vasopressors to prevent circulatory arrest. The initiation of vasopressor therapy in hemorrhagic shock may have usefulness in restoring hemodynamic parameters and vital organ perfusion, thereby reducing the need for aggressive fluid therapy and minimizing dilutional coagulopathy. Among vasopressors, norepinephrine and vasopressin have been used in the majority of the trials. Norepinephrine, being a sympathomimetic agent with predominant vasoconstrictive effect, has been suggested as a first-line vasopressor in hemorrhagic shock. Inotropic agent infusion of dobutamine or epinephrine is advocated in the presence of myocardial dysfunction, 2 which often occur in those trauma patients with pericardial effusion, cardiac contusion, or secondary to brain injury. 2 In the event of inability to evaluate for myocardial dysfunction as it would be in the majority of trauma situations, cardiac dysfunction must be suspected if the patient fails to respond to adequate fluid therapy and norepinephrine infusion.
Footnotes
Acknowledgements
The authors would like to thank all the nurses and supporting staff for the resuscitation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent is not obtainable as patient is deceased. All identifying details of the patient are omitted.