
Abstract
Background:
To our knowledge, there has been no study comparing intubation characteristics between attending and non-attending emergency physicians in Southeast Asia. We aim to identify whether the use of direct laryngoscopy compared to video laryngoscopy affects first-pass success rates between attending emergency physicians and non-attending emergency physicians.
Materials and methods:
Retrospective analysis of data from 2009 to 2016 in an existing airway registry managed by an academic Emergency Department in Singapore. Primary outcome was first-pass success intubation rate. Secondary outcome was first-pass success rate for difficult intubations. Difficult intubations were defined as LEMON (Look externally, Evaluate 3-3-2 rule, Mallampati score, Obstruction, Neck mobility) score of more than 1.
Results:
There were a total of 2909 intubations. Attending emergency physicians conducted 1748 intubations, while non-attending emergency physicians conducted 1161 intubations. The first-pass success rates for AEP were 84.2% and 67.4% for non-attending emergency physicians. Direct laryngoscopy was used in 86.2% of intubation by attending emergency physicians compared to 89.0% in the intubation by non-attending emergency physicians. Also, 7.6% of intubations by the attending emergency physicians were difficult compared to 8.8% by the non-attending emergency physicians (p = 0.25). Logistic regression of the effect of laryngoscopy device on first-pass success in all intubations showed a negative association with video laryngoscopy (odds ratio, 0.70; 95% confidence interval, 0.56–0.88). In the subgroup of difficult intubations, non-attending emergency physicians are 1.54 times (95% confidence interval, 0.53–4.42) as likely to have first-pass success with video laryngoscopy compared to that with direct laryngoscopy. On the contrary, in the subgroup of difficult intubations, attending emergency physicians are 0.90 times (95% confidence interval, 0.38–2.12) as likely to have first-pass success with video laryngoscopy compared to that with direct laryngoscopy.
Conclusion:
Our study showed that video laryngoscopy has a lower first-pass success rate for all intubations in general. Intubations performed by attending emergency physicians with direct laryngoscopy were associated with a higher first-pass success rate.
Keywords
Introduction
First-pass success in emergency intubations has been associated with a reduced incidence of adverse events. 1 Level of experience and choice of video laryngoscopy (VL) or direct laryngoscopy (DL) have been reported to be features associated with first-pass success in intubations.2–4 In Southeast Asia, there have been no studies examining the relationship between these two factors and how they relate to first-pass success in intubation. We aim to identify whether the use of VL compared to DL affects first-pass success rates for endotracheal intubations – difficult or otherwise – when performed by attending emergency physicians (AEP) and non-attending emergency physicians (NAEP).
Materials and methods
This was a single-centre retrospective observational study. Data were obtained from the Emergency Airway Registry of Singapore General Hospital (SGH), an academic Emergency Department (ED) in Singapore, between 2009 and 2016. Data from all intubations performed in the ED during this period were recorded on a standardized paper form, post-intubation. The entries were then transcribed into the electronic Emergency Airway Registry and anonymized. These forms collected data on patient demographics, types of laryngoscopy device used and complications that occurred as a result of the intubation. Examples of complications that occurred include, but not limited to, mainstem intubation, oesophageal intubation and hypotension. This study was approved by the Institutional Review Board. Data collection did not require written consent from the patients.
AEP are senior physicians who are board certified in emergency medicine by the Specialist Accreditation Board of the Ministry of Health, Singapore. NAEP are physicians who are not board certified – these include emergency medicine residents, residents from other disciplines and medical officers who are not in a Residency Programme. All intubations by NAEP were supervised by AEP. For this study, intubations performed in the ED by physicians from other disciplines, for example, anaesthetists, were excluded.
The VLs used during this period were GlideScope® (Verathon Medical Inc., Bothell, USA), C-MAC (Karl Storz GmbH & Co. KG, Tuttlingen, Germany) and McGrath (Aircraft Medical, UK). DL was carried out with the Macintosh Curved or Miller Straight Blade (Welch Allyn, NY, USA). The choice of VL device was left to the discretion of the intubating physician. Both AEP and NAEP were trained to use VL via several methods, including task-trainers, simulation sessions and the hospital’s Emergency Airway Management Course.
The primary outcome was first-pass success rate. A single pass was defined as an attempt to pass the endotracheal tube (ETT) through the vocal cords. A pass will usually be followed by airway manoeuvres, for example, bagging or suctioning. Confirmation of ETT placement was determined by a combination of direct visualization, auscultation, observation of ETT misting and end-tidal CO2 capnography (EtCO2).
The secondary outcome was first-pass success rates for difficult intubations. A difficult intubation is defined as the presence of two or more LEON features (Look externally, Evaluate 3-3-2, Obstruction, Neck Mobility). This definition was chosen as the LEON criterion is a validated and commonly used tool to assess a difficult airway. 5 The ‘M’ for Mallampati in the traditional LEMON (Look externally, Evaluate 3-3-2 rule, Mallampati score, Obstruction, Neck mobility) score has been removed due to its impracticality in the emergency setting.
Statistical calculations were performed using SPSS 26.0 for Windows (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). Continuous and ordinal variables were presented as median and categorical variables as frequencies. Categorical variables were analysed using chi-squared test for differences between groups. The Wilcoxon signed-rank test was used to identify differences between groups for continuous variables. Logistic regression analysis was carried out for factors hypothesized to be associated with first-pass intubation success. Statistical significance was considered if p < 0.05. Odds ratios (OR) and 95% confidence intervals (95% CIs) were presented where applicable.
Results
Patient characteristics
In all, 2950 intubations were performed in SGH ED from 2009 to 2016. Of these, 2909 (98.6%) were conducted by emergency physicians, with 1748 (59.3%) intubations by AEP and 1161 (39.3%) by NAEP (Table 1). Patients intubated by AEP were slightly younger than those intubated by NAEP (mean age, 60.7 vs 63.5 years, p < 0.01). Gender distribution between the groups was otherwise similar. AEP performed more trauma intubations than NAEP (13.6% vs 8.5%, p = 0.01).
Baseline characteristics.
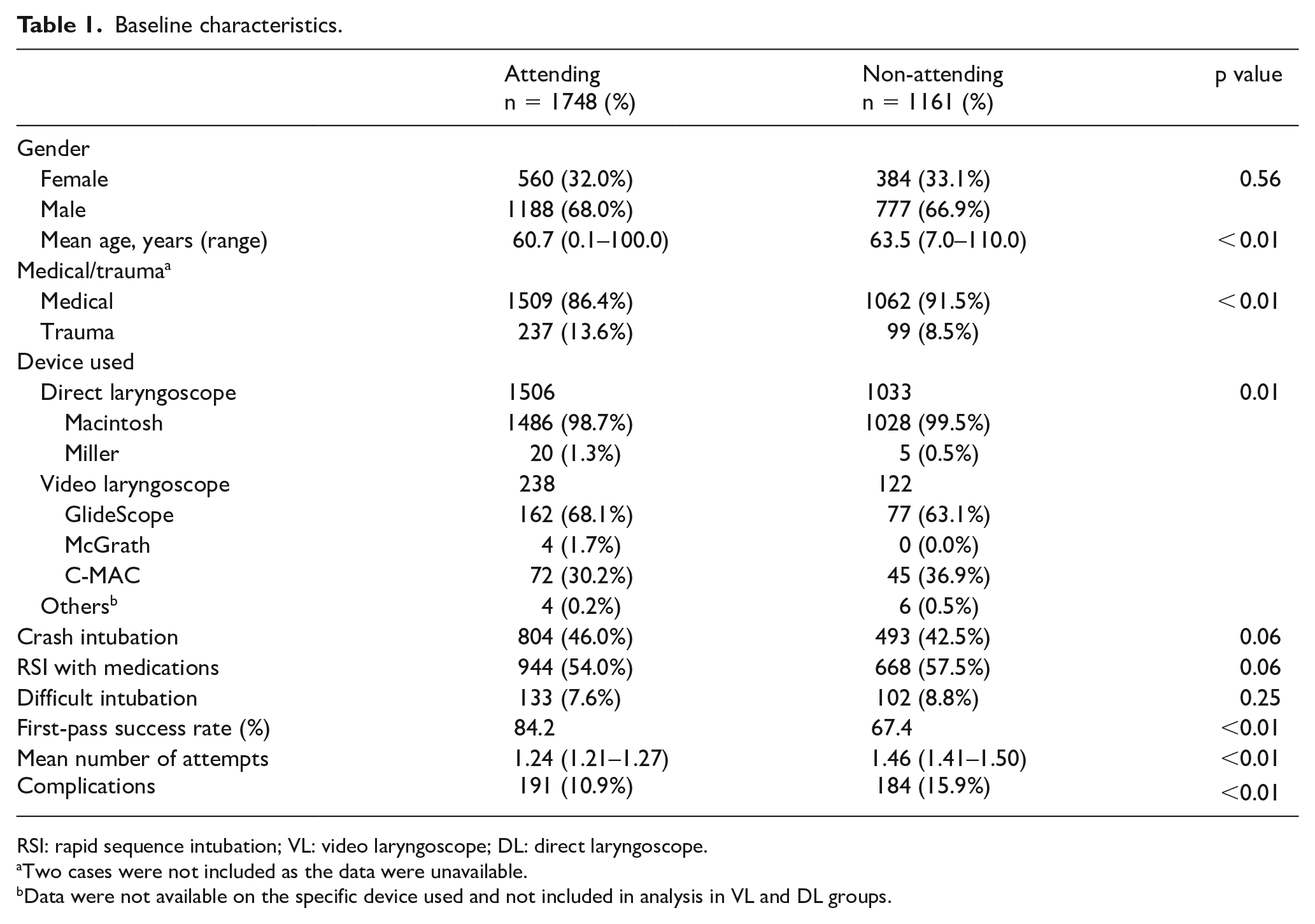
RSI: rapid sequence intubation; VL: video laryngoscope; DL: direct laryngoscope.
Two cases were not included as the data were unavailable.
Data were not available on the specific device used and not included in analysis in VL and DL groups.
All intubations
Overall, AEP had a higher first-pass success rate than NAEP (84.2% vs 67.4%, p < 0.01). The mean number of attempts was 1.24 among AEP and 1.46 among NAEP. Intubation by AEP was positively associated with first-pass success (OR, 2.63; 95% CI, 2.20–3.15) (Table 2). AEP experienced significantly lower complication rates than NAEP (10.9% vs 15.9%, p < 0.01).
Results of logistic regression for effect of predictors on first-pass success.
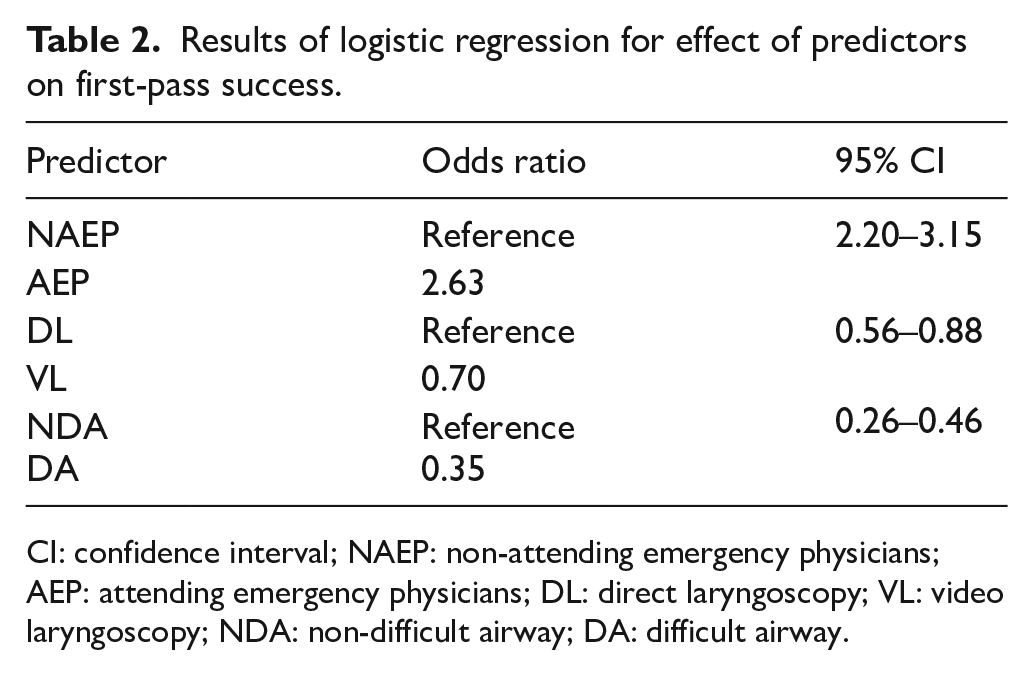
CI: confidence interval; NAEP: non-attending emergency physicians; AEP: attending emergency physicians; DL: direct laryngoscopy; VL: video laryngoscopy; NDA: non-difficult airway; DA: difficult airway.
Of the 1748 intubations performed by AEP, 238 (13.6%) were with VL. Among AEP, use of VL was associated with a lower first-pass success rate compared to use of DL (70.6% vs 86.3%; OR, 0.38; 95% CI, 0.28–0.52) (Table 3). Of the 1161 intubations performed by NAEP, 122 (10.5%) were with VL (Table 4). Among NAEP, there was no difference in first-pass success rates whether VL or DL was used (70.6% vs 67.1%; OR, 1.17; 95% CI, 0.78–1.77).
First-pass success rates.
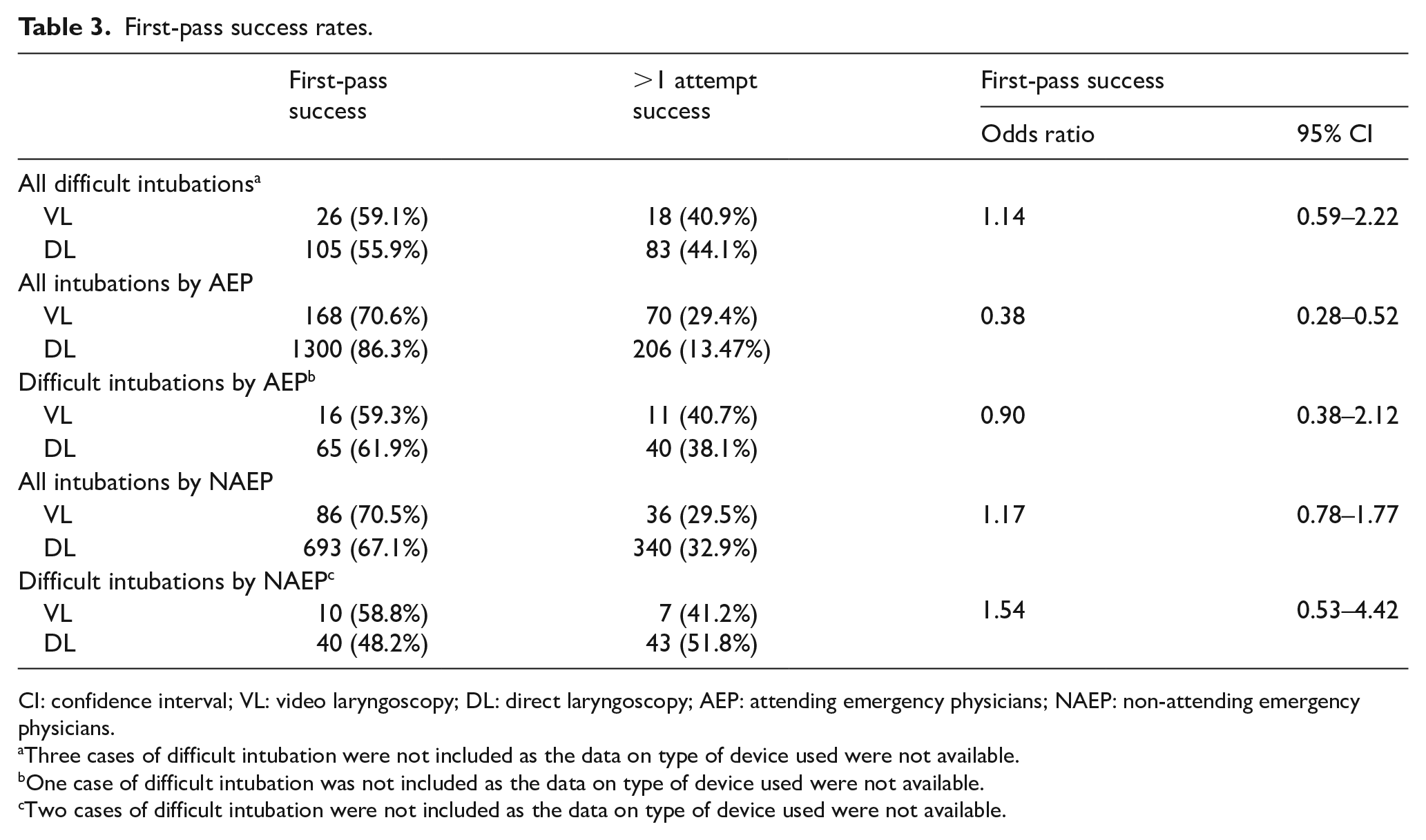
CI: confidence interval; VL: video laryngoscopy; DL: direct laryngoscopy; AEP: attending emergency physicians; NAEP: non-attending emergency physicians.
Three cases of difficult intubation were not included as the data on type of device used were not available.
One case of difficult intubation was not included as the data on type of device used were not available.
Two cases of difficult intubation were not included as the data on type of device used were not available.
First-pass success rate for various VLs.
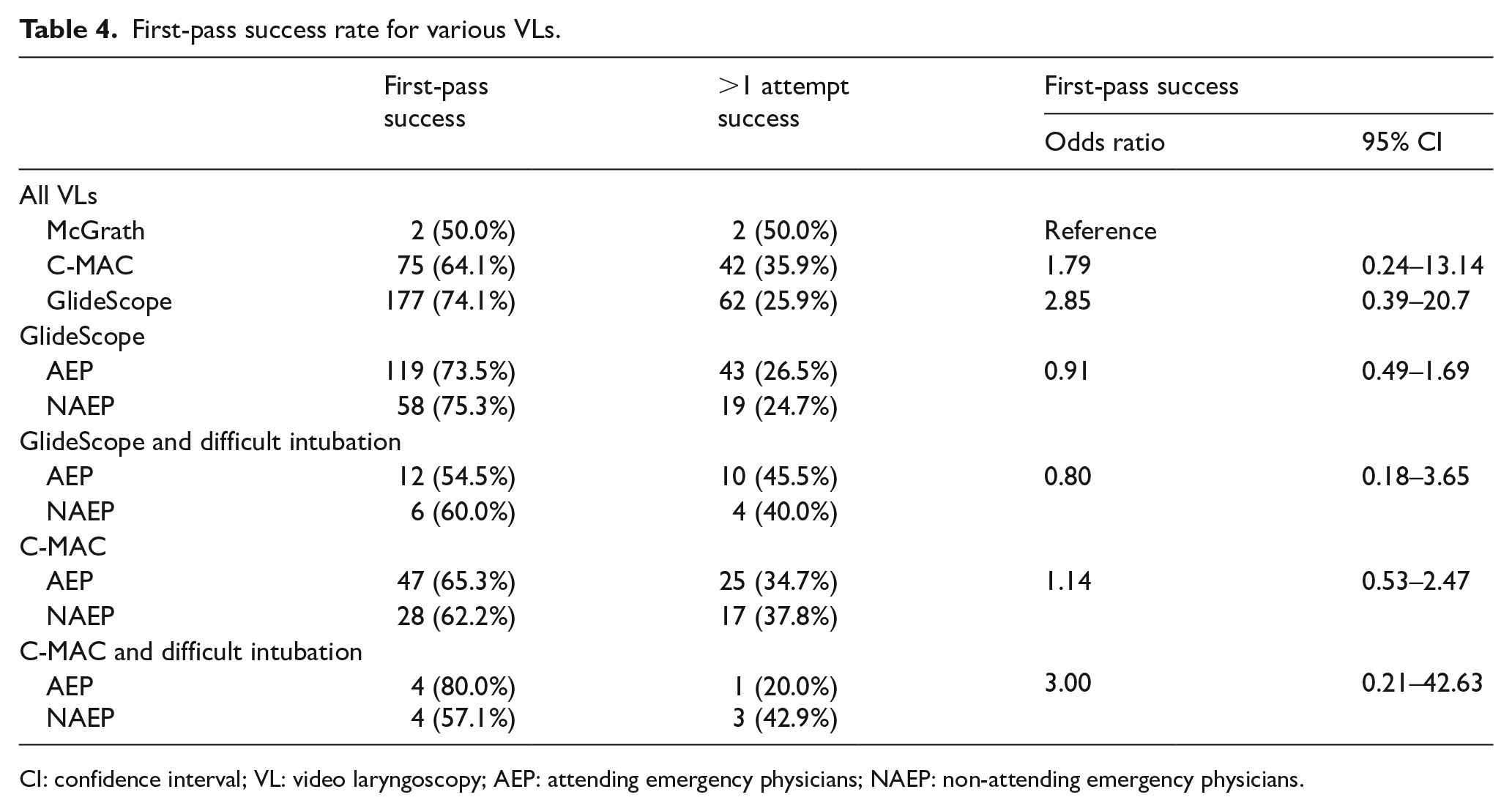
CI: confidence interval; VL: video laryngoscopy; AEP: attending emergency physicians; NAEP: non-attending emergency physicians.
The overall first-pass success rate for all intubations was lower for VL (70.6%) than for DL (78.5%). Logistic regression of the effect of laryngoscopy device on first-pass success in all intubations showed a negative association with VL (OR, 0.70; 95% CI, 0.56–0.88).
Difficult intubations
Altogether, there were 235 difficult intubations. AEP encountered fewer difficult intubations than NAEP (7.6% vs 8.8%, p = 0.25). The first-pass success rates for difficult intubations were higher among AEP compared to NAEP, although this difference did not reach statistical significance (61.4% vs 50%, p = 0.07). Unsurprisingly, a difficult airway was negatively associated with first-pass intubation success (OR, 0.35; 95% CI, 0.26–0.46) (Table 2).
There was no statistically significant difference in first-pass success rate between VL (52.3%) and DL (55.9%) in difficult intubations (OR, 1.14; 95% CI, 0.59–2.22) (Table 3). First-pass success rates were similar for difficult intubations performed by AEP and NAEP using VL (59.3% vs 58.8%, p = 0.98). For difficult intubations performed with DL, AEP had a higher first-pass success rate (61.9%) than NAEP (48.2%) (p < 0.01).
Video laryngoscopy
The GlideScope had the highest first-pass success rate among all VLs (OR, 2.85; 95% CI, 0.39–20.7), followed by C-MAC (OR, 1.79; 95% CI, 0.24–13.14). There was no statistically significant difference in the first-past success rates among AEP and NAEP between different VL models (Table 3).
Discussion
AEP were 2.63 times (95% CI, 2.63–3.15) as likely to have first-pass intubation success compared to NAEP. It has been shown that multiple attempts at intubation may result in a higher rate of adverse events. 1 Hence, having the most experienced operator to perform intubation in the ED would increase the chance of success and minimize harm to the patient.
Existing publications6–10 report no statistically significant difference in first-pass success rates between VL and DL. Our observed finding of VL having lower overall first-pass success rate compared to DL is dissimilar to current literature. The greater familiarity with DL during the study period likely accounted for the higher rates of DL use in our study and the lower rates of first-pass success with VL.
For difficult intubations, the association of VL with first-pass success rates (OR, 1.14; 95% CI, 0.59–2.22) is inconclusive. The presence of a video camera at the distal end of the VL allows for visualization of the vocal cords without alignment of the three intubation axes (oral, pharyngeal and laryngeal). Specifically, the rigid stylet of the GlideScope Video Laryngoscope allows for smooth insertion11,12 of the ETT along the hyperacute angle of the laryngoscope blade. These features likely helped improve first-pass success rates in difficult intubations,7,11–13 especially where small mouth opening and limited neck mobility posed a challenge. The C-MAC allows the user to perform intubation as if it were a DL or via its attached video camera with an external monitor. The McGrath has a monitor attached to the laryngoscope handle, allowing the user to maintain line of sight of the patient and hand position while intubating. Despite the various traits of each device, our study did not show a statistically significant improvement in first-pass intubation rates in difficult intubations among AEP and NAEP (Table 3).
Nonetheless, VL may have a role in training novices in endotracheal intubation.14,15 An improved glottic view and ease in identification of anatomy are reported factors resulting in success with VL among NAEP when performing difficult intubations. In addition, the ability to visualize the NAEP field of view with VL also allows the supervising AEP to provide timely and appropriate advice during intubation.
Our study suggests that operators performed better with devices they were familiar with, such as DL. Therefore, AEP (who were first trained with DL) did better than NAEP with DL. However, when encountering a difficult airway, the difference in first-pass success rates with DL and VL was greatly reduced. This highlights the need for training in the use VL and its utility as an adjunct for securing the airway during difficult intubations.
We acknowledge the importance of balancing operator experience and device choice so that the first-pass success is achieved. However, if novice operators are not provided with the opportunity to perform intubations in the emergency setting, this may eventually affect their first-pass success rates as future airway managers.
Limitations
This was a retrospective study. Data were manually entered from the standardized paper form into the electronic registry, resulting in possible transcription errors. Whenever possible, the recorded data were crosschecked against existing data in the electronic medical records. There was, however, a large extent of heterogeneity in the completeness of electronic health record documentation, which limited the utility of this solution. Since the forms were completed after resuscitation – including intubation – was concluded, recall bias may contribute to inaccurately recorded data. However, this time lag is likely to be short, and we felt that this was a necessary compromise between maintaining patient safety (as it may not be feasible to complete the form during an ongoing resuscitation/intubation) and accurate data collection. The study data were also obtained from a single institution, limiting the generalizability of the results.
The study was not powered to detect a difference in first-pass success rates between VL and DL for difficult intubations. This could account for the results seen in Table 3, where the positive association of VL with first-pass success within the difficult intubation group was not statistically significant.
We did not use a single standardized definition such as the Intubation Difficulty Score (IDS). 16 The LEON score, by itself, has been shown to correlate well with difficulty of intubation.5,17,18 Reeds et al identified the median LEON score for difficult intubation to be that of 2, which is the definition we adopted. In addition, heterogeneity in training with the use of the various laryngoscopy devices may exert a confounding effect on the results obtained. We were unable to identify the extent of training AEP and NAEP received due to the retrospective nature of this study. Inadequate training with VL may potentially contribute to a poorer overall first-pass success rate with VL use.
Conclusion
Our study shows that video laryngoscopy has a lower first-pass success rate for all intubations in general. Intubations performed by attending emergency physicians with the direct laryngoscope were associated with a higher first-pass success rate. Operators may achieve higher first-pass success rates with a device they are most familiar with. There is a need for further prospective and multi-centre studies to validate these results.
Supplemental Material
APPENDIX_LARYNGOSCOPE_IMAGES_ver_1.2 – Supplemental material for Does video laryngoscopy or direct laryngoscopy affect first-pass success rates for intubation among attending and non-attending emergency physicians in the emergency department?
Supplemental material, APPENDIX_LARYNGOSCOPE_IMAGES_ver_1.2 for Does video laryngoscopy or direct laryngoscopy affect first-pass success rates for intubation among attending and non-attending emergency physicians in the emergency department? by Wan Paul Weng, Nur Diana Bte Zakaria, Seow Gek Ching and Evelyn Wong in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors would like to thank Prof. V. Anantharaman for his guidance and support in writing this manuscript.
Authors’ contributions
W.P.W., N.D.B.Z., and E.W. developed the study and supervised the data collection. S.G.C. assisted with data collection and entry. W.P.W. analysed the data. W.P.W. drafted the manuscript. N.D.B.Z. and E.W. provided advice on the manuscript and contributed as corresponding authors. W.P.W. takes responsibility for the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The dataset analysed in this current study may be made available on reasonable request. Please contact W.P.W.
Ethical approval and consent to participate
Approval from the Singhealth Institutional Review Board was obtained for data collection from the Airway Registry.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.