
Abstract
Objective:
We aimed to evaluate Model for End-stage Liver Disease excluding international normalized ratio (MELD-XI) score for prediction of 30-day in-hospital mortality in a cohort of patients with ST elevation myocardial infarction.
Methods:
The medical records of a total of 256 patients admitted with ST elevation myocardial infarction to the emergency department between January 2015 and January 2019 were retrospectively reviewed. A total of 111 patients were found eligible for the study. MELD-XI score was analyzed and compared on the basis of survival status.
Results:
A total of 111 patients with a mean age of 62.5 ± 2.55 years were included in the study. In total, 81% (n = 90) of the patients were male and 19% (n = 21) were female. The mean MELD-XI score of the patients was 10.1 ± 1.1. A total of 12 patients (12.9%) died within 30 days after hospitalization. The median MELD-XI score of the patients who died in the hospital was significantly higher than the patients survived (11.0 (10.5–11.6) vs 9.5 (9.4–13.8); p < 0.01). However, Gensini score was not significantly different between the surviving and deceased patients (p > 0.05). MELD-XI score was significantly correlated to left ventricular ejection fraction (r = −232, p < 0.01), and both parameters and age were significant independent predictors of in-hospital mortality (odds ratio: 1.73, 95% confidence interval: 1.25–2.39, p < 0.05; odds ratio: 0.89, 95% confidence interval: 0.81–0.99, p < 0.05; and odds ratio: 1.07, 95% confidence interval: 0.99–1.15, p < 0.05, respectively). A MELD-XI cut-off point of 10 had a sensitivity of 100% and a specificity of 78.8% for in-hospital mortality (area under receiver operating characteristics curve: 0.92, 95% confidence interval: 0.87–0.97, p < 0.05). A survival analysis based on a MELD-XI threshold of 10 revealed that the patients in the high-MELD-XI group had a significantly worse in-hospital survival (log rank test p < 0.001).
Conclusion:
MELD-XI score is a useful tool for in-hospital mortality prediction in patients referring to emergency medicine with acute ST elevation myocardial infarction.
Introduction
Liver dysfunction is a common sequela of heart failure (HF). 1 Poor global perfusion and hepatic congestion secondary to right ventricular failure are the main mechanisms of liver dysfunction in HF patients. Studies have demonstrated that abnormal results on liver function tests in patients with HF were independently related to adverse outcomes and increased risk of mortality.2,3 Liver dysfunction due to congestive HF is often referred to as congestive hepatopathy. HF represents a state of reduced cardiac output, leading to diminished organ perfusion, hepatocellular hypoxia, and poor prognosis. As in acute or chronic HF patients, right or left ventricular dysfunction that occurs during each episode of acute coronary syndrome is one of the key elements leading to poor prognosis. Furthermore, an increased right atrial (RA) pressure raises passive venous hepatic congestion. Similarly, worsening of renal function is strongly related to cardiac disease. Hemodynamic alterations due to low cardiac output and altered venous return contribute to the development and progression of cardio–renal interactions. 4
Model for End-stage Liver Disease (MELD) scoring system was originally developed for patients with cirrhosis awaiting liver transplantation and it could estimate the progression of liver dysfunction based on the level of creatinine, total bilirubin, and the international normalized ratio (INR). 5 Modification of the MELD score excluding the INR (MELD-XI score) was proposed more recently, since the INR becomes dissociated from liver dysfunction in patients receiving anticoagulation therapy. 6 Previously, this scoring system has been applied and tested in patients with end-stage HF, such as patients with Fontan circulation requiring surgery, patients with acute HF, and those with advanced HF awaiting heart transplantation. In both studies, an elevated MELD-XI score was strongly associated with an increased risk of adverse outcomes.7,8 However, the prognostic impact of the MELD-XI score has not been investigated in patients with acute coronary syndrome, specifically ST elevation myocardial infarction. The aim of this study was to determine the prognostic value of the MELD-XI score calculated at admission with respect to 30-day in-hospital mortality in patients with acute ST elevation myocardial infarction.
Methods
This study was approved by Local Institutional Review Board (Project No: KA19/217) and supported by Local University Research Fund. We retrospectively analyzed the data of 256 consecutive patients admitted with acute ST elevation myocardial infarction between January 2015 and January 2019. Of these, 111 of them were found eligible. The demographic, clinical, electrocardiographic, echocardiographic, and biochemical information of the study population were recorded. The MELD-XI score was calculated as follows: MELD-XI = 5.11 × In bilirubin (serum total bilirubin) + 11.76 × In creatinine (serum creatinine) + 9.44. 6 Admission serum creatinine and bilirubin values were used, and if there was more than one serum creatinine or total bilirubin value on the day of admission, the highest value was used. The lower limit of bilirubin and creatinine was set at 1.0 mg/dL.6,8 Patients with known liver disease on dialysis and using oral anticoagulants were excluded, as were those who had any of clinical, demographic, electrocardiographic, laboratory, echocardiographic, or angiographic data missing. Every patient underwent standard clinical evaluation and received guideline-recommended therapy. 9 Gensini score was calculated from the angiograms in all patients to assess the extent of coronary artery disease. No informed consent was obtained from the subjects due to the retrospective nature of this study.
Statistical analysis
SPSS v 21.0 (IBM, Armonk, NY, USA) was used for all statistical analyses. Normality of data was tested using Kolmogorov–Smirnov test. Descriptive statistics included mean ± standard deviation for normally distributed quantitative variables; median (min–max) for non-normally distributed quantitative variables; and number and percentage for categorical variables. Normally distributed variables were compared using Student’s t test; non-normally distributed quantitative variables using Mann–Whitney U test; and categorical variables using the chi-square test or Fisher’s exact test. Correlation analysis between variables was performed using Pearson and Spearman correlation tests were applicable. The significant predictors of in-hospital mortality were initially tested with a univariate analysis using all available variables. All univariate predictors of mortality with p value ⩽0.2 were then used in a binary logistic regression model with forward Wald method to determine the independent predictors of in-hospital mortality rate. Receiver operating characteristics (ROC) curves were drawn to determine the predictive powers of independent predictors of 30-day in-hospital mortality. Kaplan–Meier curve for cumulative survival was drawn and log-rank test performed to explore the effect of variables on in-hospital survival. A p value of <0.05 was considered statistically significant.
Results
We initially included 256 patients in our retrospective analyses.We excluded 145 patients due to missing medical data. The eligible patients (n = 111), with a mean age of 62.5 ±2.55 years, were predominantly men (n = 90, 81%). A total of 37 (33.3%) patients had acute anterior ST elevation myocardial infarction; 65 (58.6%) had acute inferior ST elevation myocardial infarction; 8 (7.2%) had acute right ventricular ST elevation myocardial infarction; 11 (9.9%) had acute lateral ST elevation myocardial infarction; and 10 (9%) had acute posterior ST elevation myocardial infarction. The demographic, clinical, biochemical, and echocardiographic data of the patient population was shown in Table 1. A total of 12 (10.9%) patients died at hospital. The deceased patients had a significantly higher MELD-XI score, age, creatinine, and blood urea nitrogen (BUN) as well as significantly higher rates of previous history of coronary artery disease, coronary artery bypass surgery, and anterior myocardial infarction but a significantly lower left ventricular ejection fraction (LVEF), hemoglobin count, and tricuspid annular plane systolic excursion (TAPSE) compared with the survivors (Table 2). However, Gensini score was not significantly different between the surviving and deceased patients. Significant univariate predictors of in-hospital mortality were age (p < 0.05), MELD-XI (p < 0.01), ejection fraction (EF; p < 0.05), TAPSE (p < 0.05), and Hb (p < 0.05). In binary logistic regression analysis, the independent predictors of in-hospital death were MELD-XI score (odds ratio (OR) 1.73, 95% confidence interval (CI) 1.25–2.39, p < 0.05), age (OR 1.07, 95% CI 0.99–1.15, p < 0.05), and LVEF (OR 0.89, 95% CI 0.81–0.99, p < 0.05). MELD-XI score was significantly and negatively correlated to LVEF in Pearson’s bivariate correlation test (r = −232, p < 0.01).
General demographic, clinical, biochemical, and echocardiographic data of the study population.
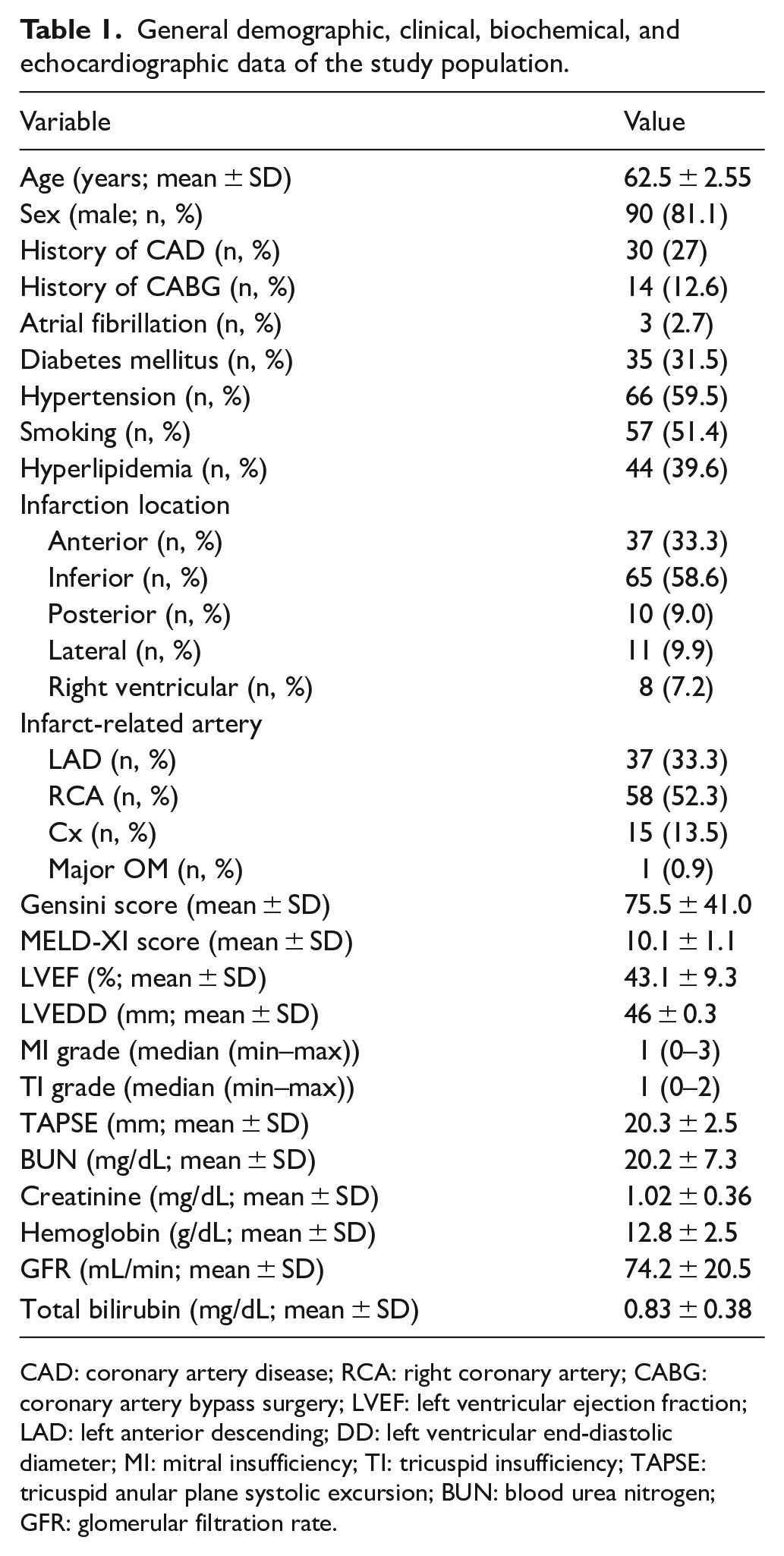
CAD: coronary artery disease; RCA: right coronary artery; CABG: coronary artery bypass surgery; LVEF: left ventricular ejection fraction; LAD: left anterior descending; DD: left ventricular end-diastolic diameter; MI: mitral insufficiency; TI: tricuspid insufficiency; TAPSE: tricuspid anular plane systolic excursion; BUN: blood urea nitrogen; GFR: glomerular filtration rate.
Comparison of demographic, clinical, biochemical, and echocardiographic data between the deceased and surviving patients.
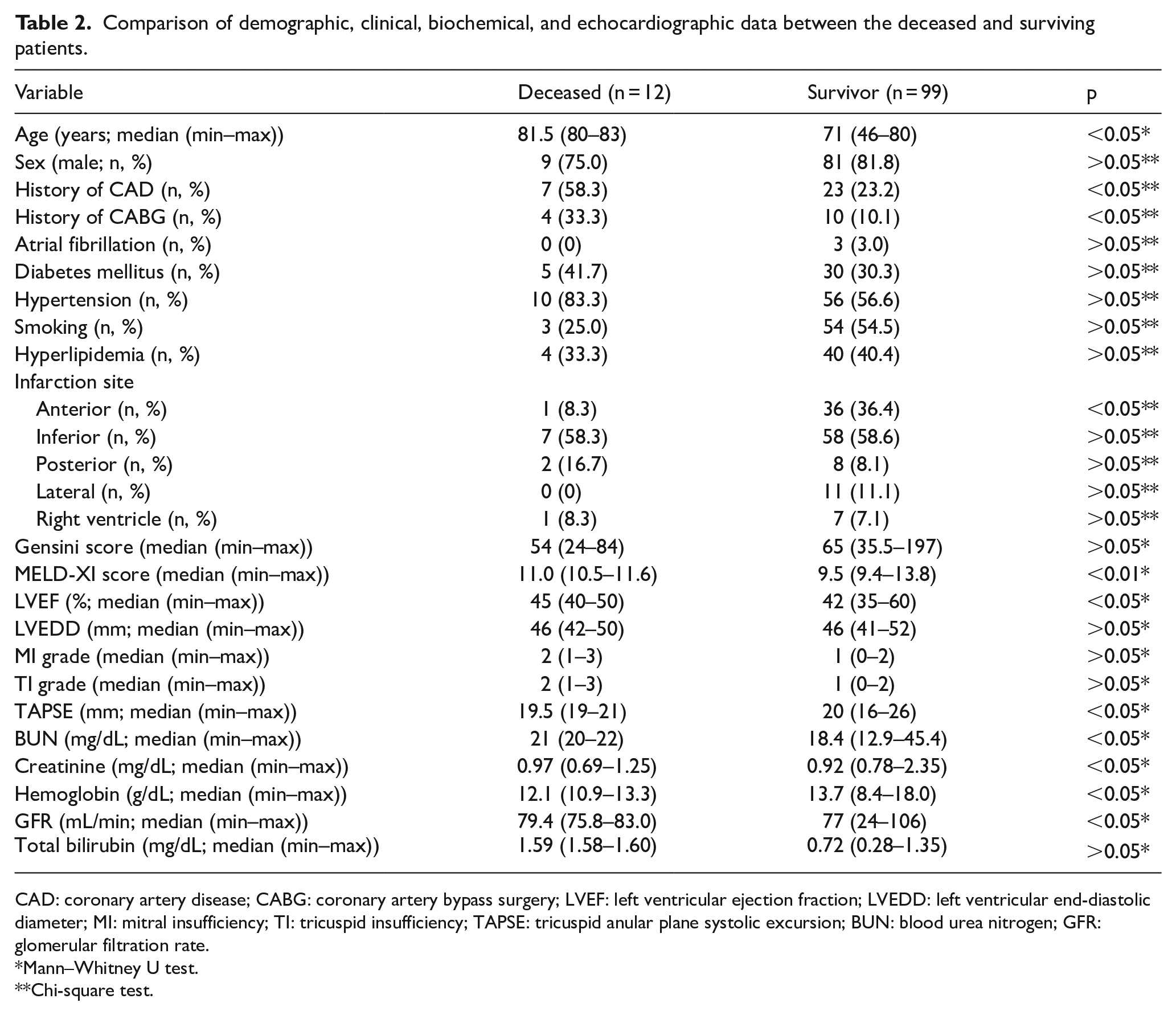
CAD: coronary artery disease; CABG: coronary artery bypass surgery; LVEF: left ventricular ejection fraction; LVEDD: left ventricular end-diastolic diameter; MI: mitral insufficiency; TI: tricuspid insufficiency; TAPSE: tricuspid anular plane systolic excursion; BUN: blood urea nitrogen; GFR: glomerular filtration rate.
Mann–Whitney U test.
Chi-square test.
A ROC analysis of MELD-XI score revealed that a MELD-XI cut-off point of 10 had a sensitivity of 100% and a specificity of 78.8% for in-hospital mortality (area under ROC curve (AUC) 0.92, 95% CI 0.87–0.97, p < 0.05; Figure 1). An in-hospital survival analysis of the two groups based on a MELD-XI threshold of 10, namely the high-MELD-XI score (MELD-XI score ⩾10) and low-MELD-XI score (MELD-XI score <10), revealed that the patients in the high-MELD-XI group had a significantly worse in-hospital (log rank test p < 0.001; Figure 2).
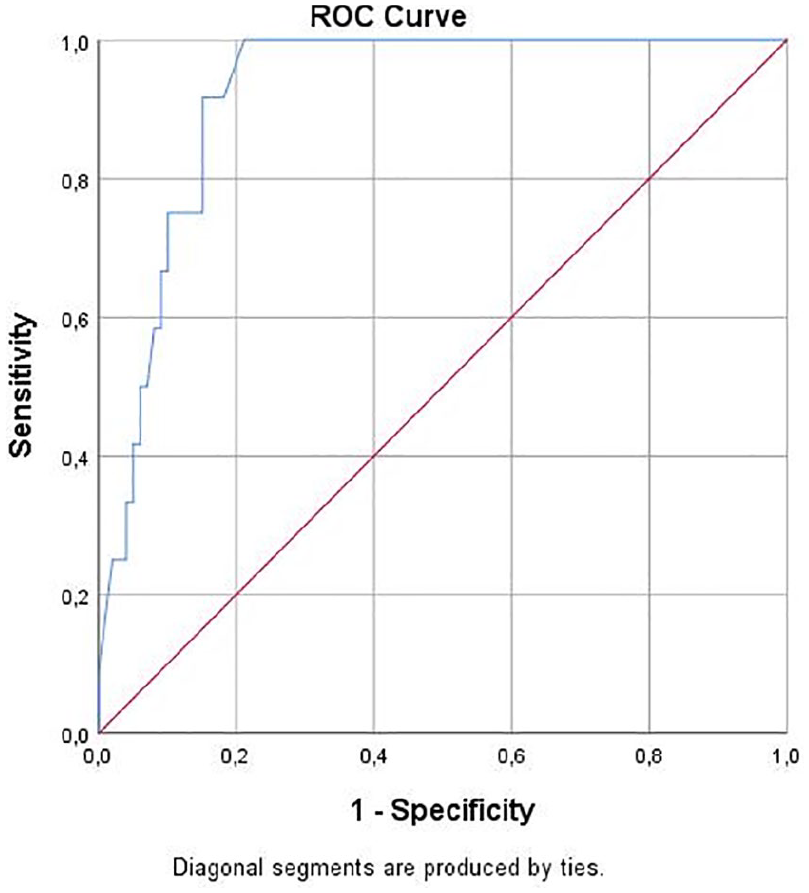
ROC curve for MELD-XI score for prediction of in-hospital mortality after acute myocardial infarction.
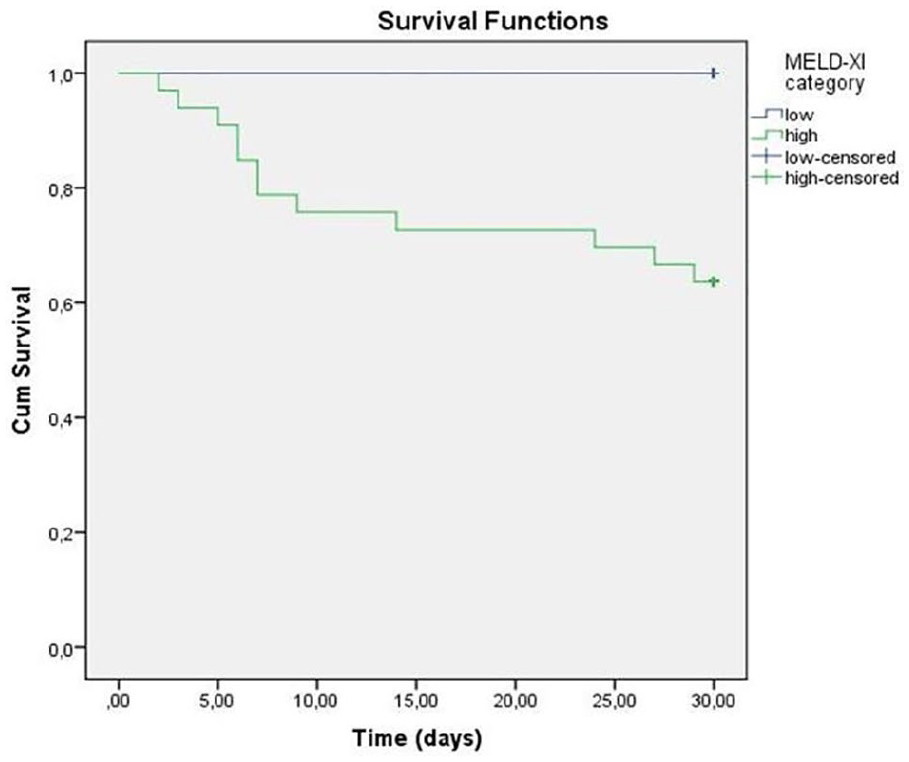
Kaplan–Meier curve to determine the effect of MELD-XI score groups (high vs low) on in-hospital survival.
Discussion
This study demonstrated that MELD XI score calculated at baseline had a significant prognostic value in terms of in-hospital mortality among patients with acute ST elevation myocardial infarction. Originally developed for end-stage liver disease, the MELD-XI score has already been validated and is widely used in the risk assesment of patients with acute HF, critically ill patients, congenital heart disease, hearth transplantation, and percutaneous valve operations.10–15 Recently, the inter-organ interaction and multi-organ dysfunction have been implicated as poor prognosticators in HF. 11 Renal and hepatic dysfunction occurring during both acute or chronic HF can be broadly categorized to be occurring by two distinct hemodynamic abnormalities, namely organ hypoperfusion due to a lowered cardiac index and venous congestion.2,3,16 The MELD-XI score incorporates two variables (serum creatinine and total bilirubin) and can take into account the function of the liver and kidneys at the same time, and an elevated MELD XI score may result from abnormalities of either bilirubin, creatinine, or both.
Acute coronary syndromes, especially acute ST elevation myocardial infarction, are associated with high short- and long-term mortality. Thus, an early identification of patients at high risk of death may aid clinicians to provide the patients with urgent and intensive care to improve their prognosis. Regardless of the application of percutaneous or surgical intervention, a variety of mortality predictors have been defined in acute coronary syndromes, such as hematological markers (red cell distribution, neutrophil count, C-reactive protein, high sensitive troponin T, neutrophil-to-lymphocyte ratio)17–19 or risk scores such as CHADS2VASC2 score, ST score, SYNTAX score.20–22 Although MELD-XI score has been validated as a prognostic marker in various cardiac or extracardiac disorders, it has been poorly studied in acute coronary syndromes. As such, there is only one study investigating the role of MELD score in acute coronary syndrome setting 23 and no study has yet assessed MELD-XI score in patients with acute myocardial infarction, in whom we aimed to use MELD-XI score to predict mortality. The present study demonstrated for the first time that deterioration of hepato-renal function (defined as an increase in MELD-XI score) at baseline carries a prognostic importance for in-hospital mortality among patients with ST elevation myocardial infarction. To our opinion, this could have been occurred in two ways. First, a low cardiac index due to myocardial infarction and/or stunning may have reduced renal and/or hepatic perfusion among other organs and increased MELD-XI score. In line with this hypothesis, we found that MELD-XI score was significantly and negatively correlated to LVEF on echocardiography, a marker of left ventricular contractility and overall systolic function, which was also a significant independent predictor of in-hospital mortality. It is well-known that a lower LVEF after ST elevation myocardial infarction confers a poor prognosis, either due to low pump function or lethal arrhythmias.24,25 Hence, our study may have indirectly verified the poor prognostic sign of reduced LVEF by using MELD-XI score. Another possibility for increased MELD-XI score in the course of acute ST elevation myocardial infarction is that increased venous pressures and engorgement may have also impaired hepatic and/or renal function and increased MELD-XI. Unfortunately, however, we had no invasive (central venous or RA pressure measurement) or noninvasive (ultrasonic assessment of inferior vena cava and/or hepatic veins) information to verify this hypothesis. Another plausible explanation of the observation that higher MELD-XI scores were associated with increased mortality is that patients with a worse in-hospital prognosis may have already had impaired renal and/or hepatic function at the time of presentation. In other words, the prognosis of such patients may have been worsened by already relatively impaired renal and/or hepatic function at the time of presentation, added to the low output and/or high venous-pressure state of myocardial infarction. All the above events may have worsened the prognosis of patients with a higher MELD-XI score. Whatever the mechanism or the cause is, however, MELD-XI score was still able to pick up those who were the sickest and likely to die. We therefore believe that MELD-XI score can be used as a general prognostic score among patients with ST elevation myocardial infarction.
The present study has several limitations that should be addressed. First, this was a retrospective study with a relatively small sample size and a limited follow-up duration. Second, we had no invasive data regarding the cardiac index or central venous pressure to verify the hypothesis that MELD-XI score is elevated in patients with hepatic or renal hypoperfusion due to lowered cardiac index and/or venous hepatic or renal congestion due to increased central venous pressure.
In summary, MELD XI score provides prognostic information about 30-day in-hospital mortality in patients with acute ST elevation myocardial infarction. Randomized controlled studies with larger size and longer follow-up duration are required to confirm our results.
Footnotes
Acknowledgements
The authors are grateful to Dr İ. Haldun Müderrisoğlu for his administrative support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Baskent University Research Fund.
Ethical approval
This study was approved by Baskent University Institutional Review Board (project no: KA19/217).