
Abstract
Objective:
The aim of this study was to report and analyse the poisoning data of Hong Kong Poison Information Centre in 2018.
Methods:
In 2018, all poisoning cases received by Hong Kong Poison Information Centre were retrieved from its database, Poison Information and Clinical Management System, for analysis.
Results:
A total of 3960 poisoned cases were analysed. There were 1770 male patients (44.7%), 2188 female patients (55.3%) and 2 sex-unspecified patients (<0.1%). The majority of cases (68.3%) were between 20 and 69 years old, and 9.9% involved children of 0–5 years old. The common causes of poisoning were suspected self-harm/suicidal attempt (36.6%), unintentional exposure (18.4%) and abusive substance use (11.1%). Excluding the common co-ingestant ethanol, the five commonest types of poison were benzodiazepines, paracetamol, Chinese herbal medicine, household products and zopiclone. Most patients were managed with supportive measures, while 13.5% and 13.7% of consultation cases were treated by decontamination and antidotes, respectively. The majority of cases had uneventful recovery; 0.8% resulted in death and 4.9% had major outcomes. A total of eight interesting cases were discussed.
Conclusion:
This 13th annual report provided the updated epidemiological information on poisoning pattern in Hong Kong and highlighted important changes in comparison with our previous reports.
Introduction
The Hong Kong Poison Information Centre (HKPIC) was established in 2005. Currently, it provides round-the-clock phone consultation service to health care professionals in Hong Kong for poison information and clinical management advice on poisoning. It also provides onsite clinical toxicology service to poisoned patients in the United Christian Hospital where the centre is located. The HKPIC also collects important poisoning epidemiological data in Hong Kong from voluntary poisoning reporting in the Hospital Authority (HA). It also contributes to the development of clinical toxicology and emergency medicine by organizing regular training activities, such as monthly seminar, basic clinical toxicology course, certificate course, the 1-year quotable diploma course in clinical toxicology (Dip Clin Tox (HKCEM and HKPIC)) and the clinical toxicology subspecialty fellowship training programme in conjunction with the Hong Kong College of Emergency Medicine (HKCEM), as well as training for overseas doctors. Besides, HKPIC published 6 articles in peer review journals in 2018, adding up to a total of 105 articles since its establishment. The mission of the HKPIC is to minimize the mortality and morbidity of poisoning by the provision of high-quality clinical toxicology service and to become one of the leading toxicology training centres in Asia-Pacific region.
HKPIC has started to publish its annual reports since 2006. It continues to provide the updated information in poisoning epidemiology and its changing trend in Hong Kong. This 13th annual report of HKPIC covers the data in 2018 and focuses on the latest poisoning pattern as in the previous reports. It also highlights some important poisoning cases in Hong Kong.
Methods
The HKPIC received its poisoning cases from two primary sources: consultation and reporting. Consultation is defined as poisoning case that health care professional consulted us for poison information and management advice, while reporting is defined as the poisoning case reported in HA, majority by all accident and emergency departments (AEDs). In 2018, all poisoning cases received by HKPIC were retrieved from its database, Poison Information and Clinical Management System (PICMS), for analysis.
The data of each poisoning case were inputted into PICMS according to the information obtained from the consulting health care professional, medical record, electronic patient record (ePR) of HA and other relevant sources. Data collected included patient demographic data, poison data (poison type and dose, route, time, place and reason of exposure), clinical data (clinical features, investigation results), management data (use of decontaminations, antidotes and other specific treatments) and outcome data (disposal for AED patient, final outcome and its relationship with the poison exposure) for consultation cases, while only patient demographic data, poison data and outcome data were inputted for the reporting cases.
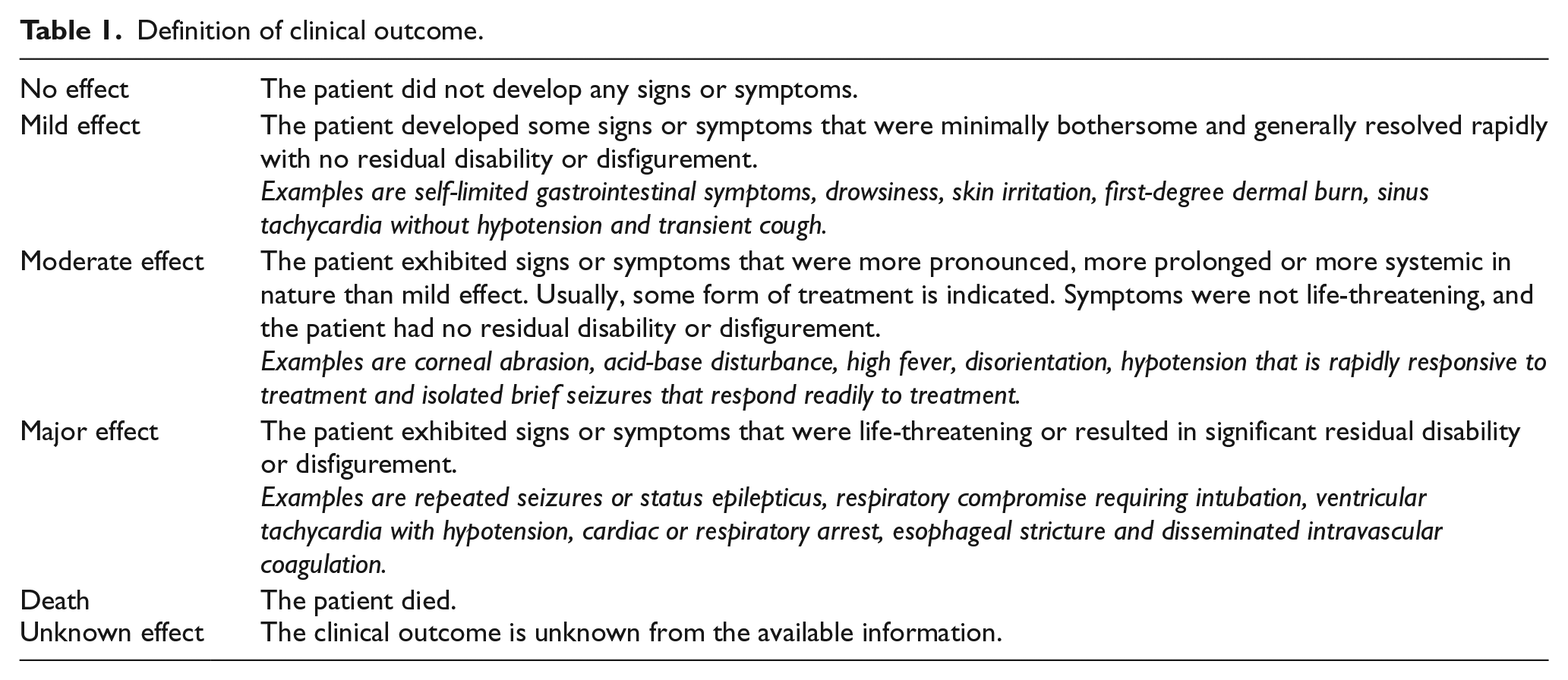
Senior doctors from the HKPIC would classify the outcome of the cases into five categories: no effect, mild effect, moderate effect, major effect or death with reference to the American Association of Poison Control Centers’ National Poison Data System 1 (Table 1). Besides, the relationship between the poison exposure and clinical outcome was graded as definite, probable, possible, not related or undetermined/not applicable according to the available information. All death or major effect cases were further reviewed by a second senior doctor to ensure that the grading was appropriate.
Definition of clinical outcome.
Information used in this annual report was considered as a part of the usual clinical data obtained by HKPIC and was passed to the researchers in a fully anonymized format.
Results
After excluding duplicate and invalid cases, the PICMS generated 3960 valid cases, including 2041 (51.5%) consultation cases and 1919 (48.5%) reporting cases for analysis in the year 2018.
The age and gender distribution of the cases are shown in Figure 1. There were 1770 male patients (44.7%), 2188 female patients (55.3%) and 2 sex-unspecified patients (<0.1%). A female predominance was noted in the majority of the age groups except for the children of age 0–12 years and for the elderly of age 70–79 years. Concerning the age distribution, the middle-aged group (40–49 years) was the commonest and the majority (68.3%) of them were between 20 and 69 years. Around one-tenth of the cases (9.9%) were children from the age of 0–5 years.
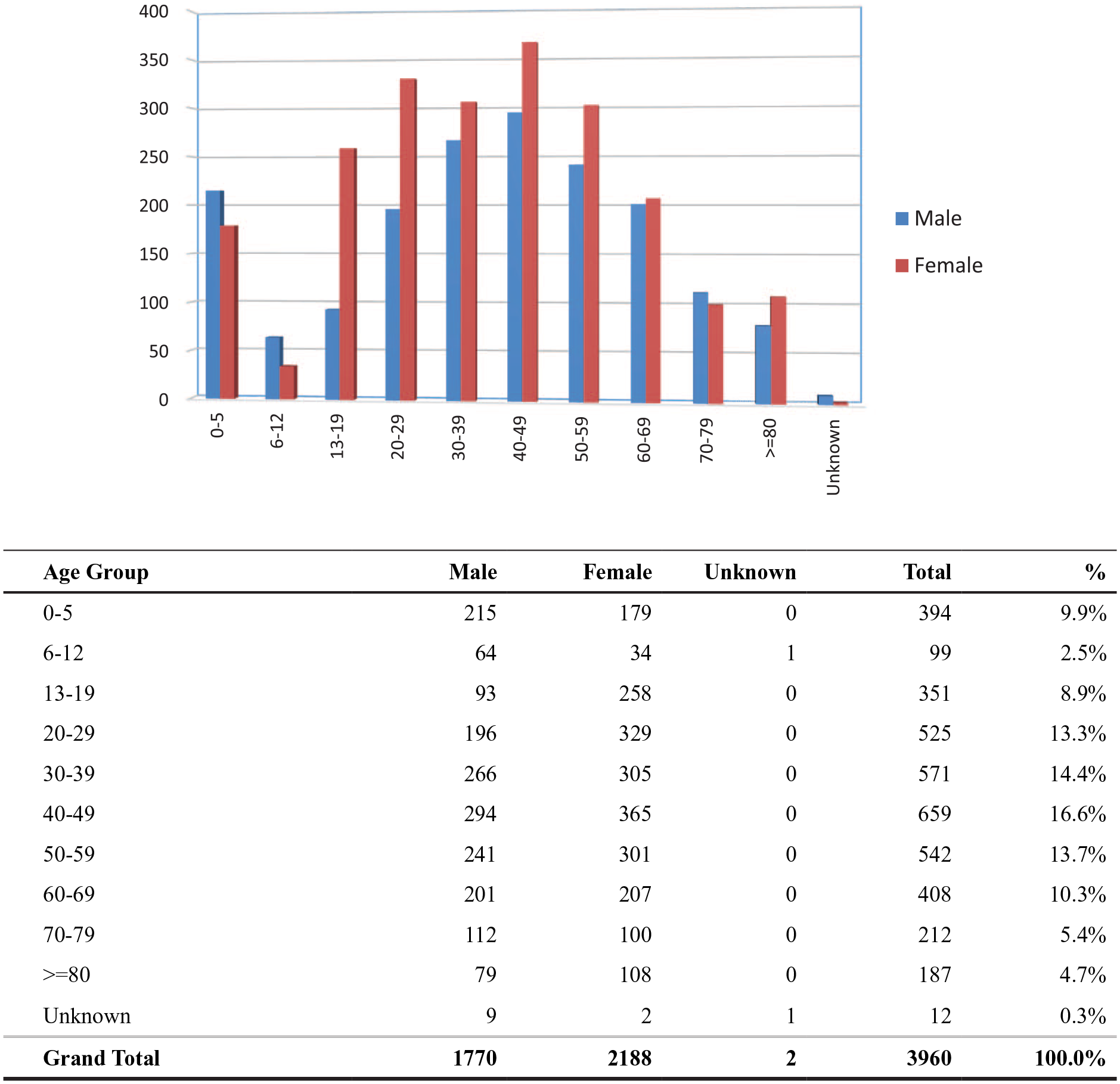
Age and gender distribution.
The reasons for poisoning are listed in Figure 2 with the most frequent cause being suspected self-harm/suicidal attempt, which accounted for 36.6% of the cases. Poisoning due to unintentional exposure (18.4%) and abusive use (11.1%) ranked the second and third commonest cause, respectively. Together with venomous bites and stings (10.0%) and adverse reactions secondary to herbal or proprietary Chinese medicine (9.4%), these five commonest reasons for poisoning contributed to the vast majority (85.5%) of the cases. As shown in Figures 3 and 4, the commonest place of exposure was in the patient’s residential place (63.7%). The commonest route of poisoning was oral exposure (81.5%), followed by dermal (7.6%) and inhalational exposure (6.0%).
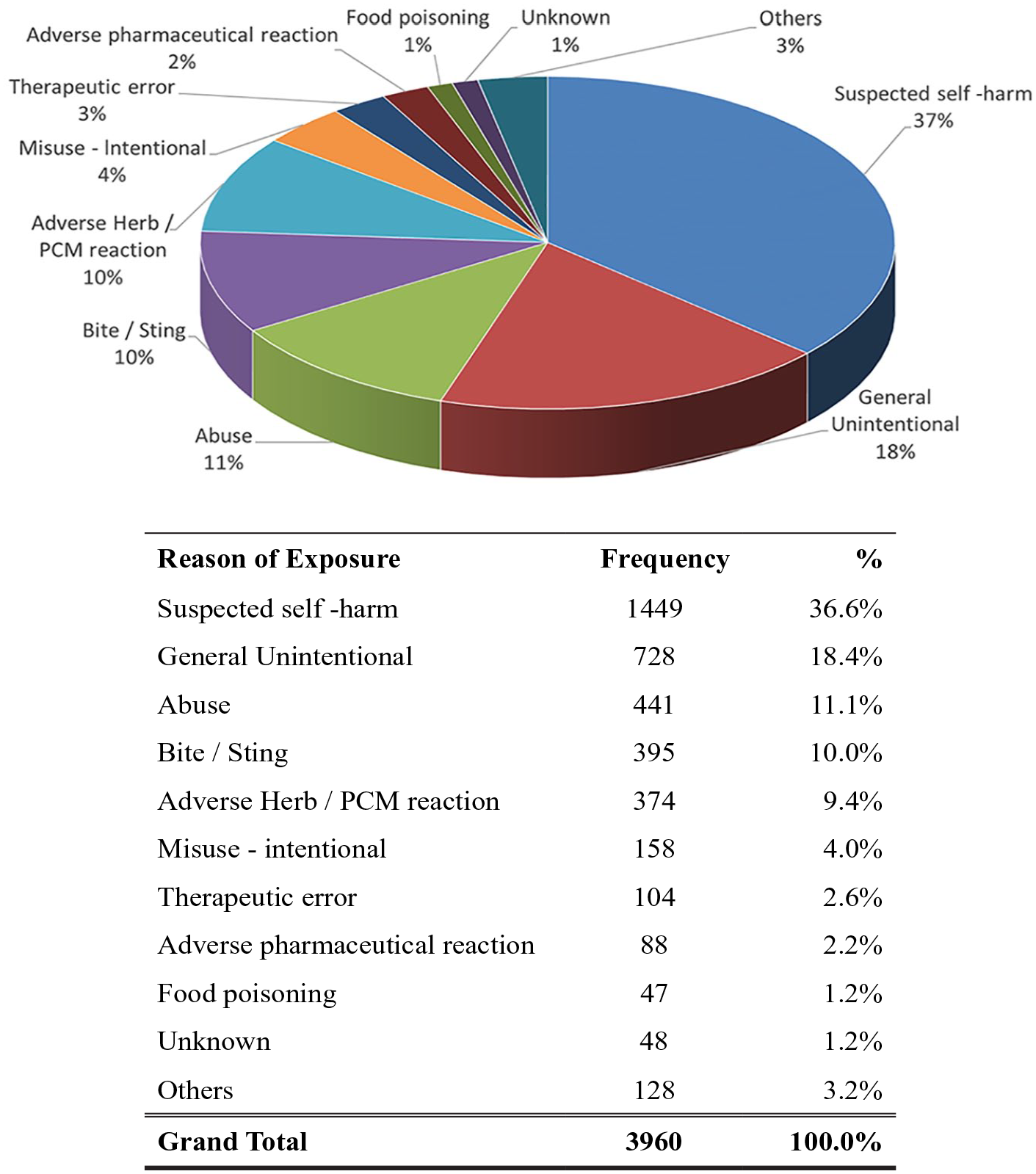
Reason of exposure.
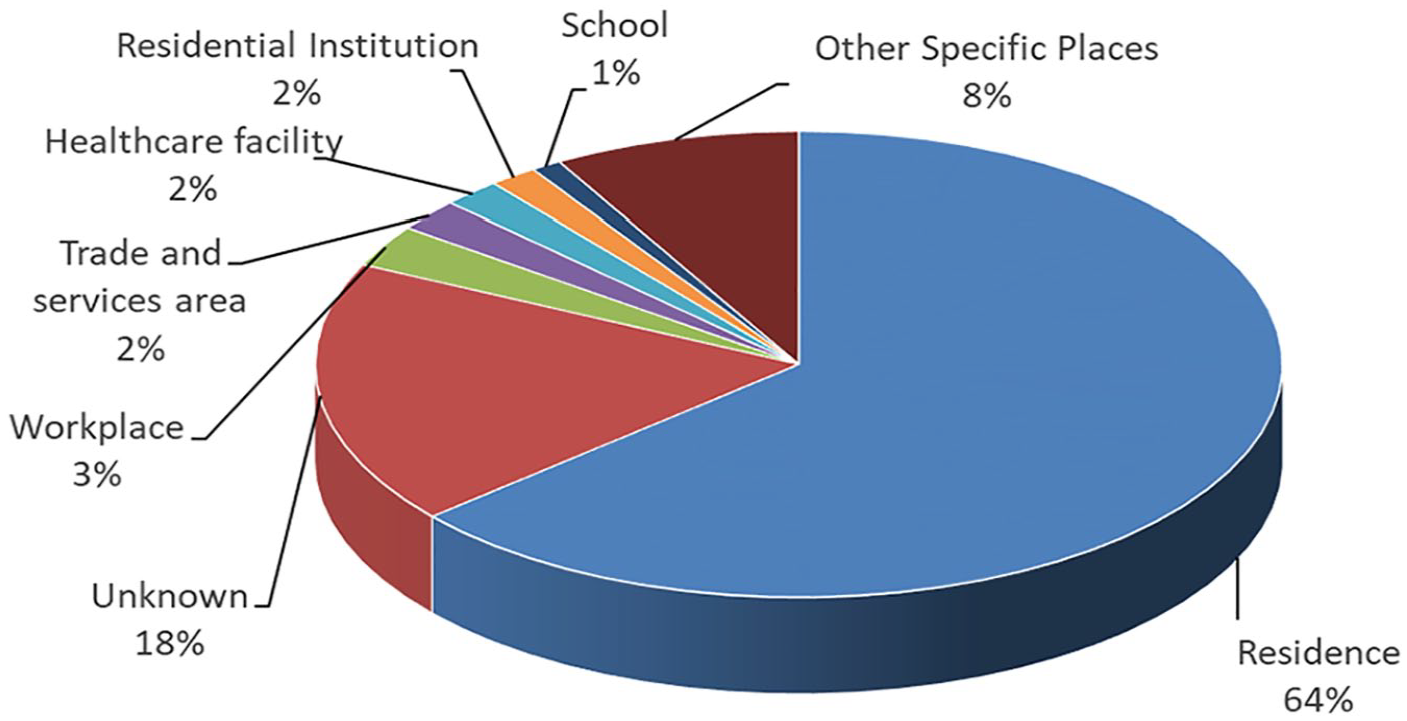
Place of exposure.
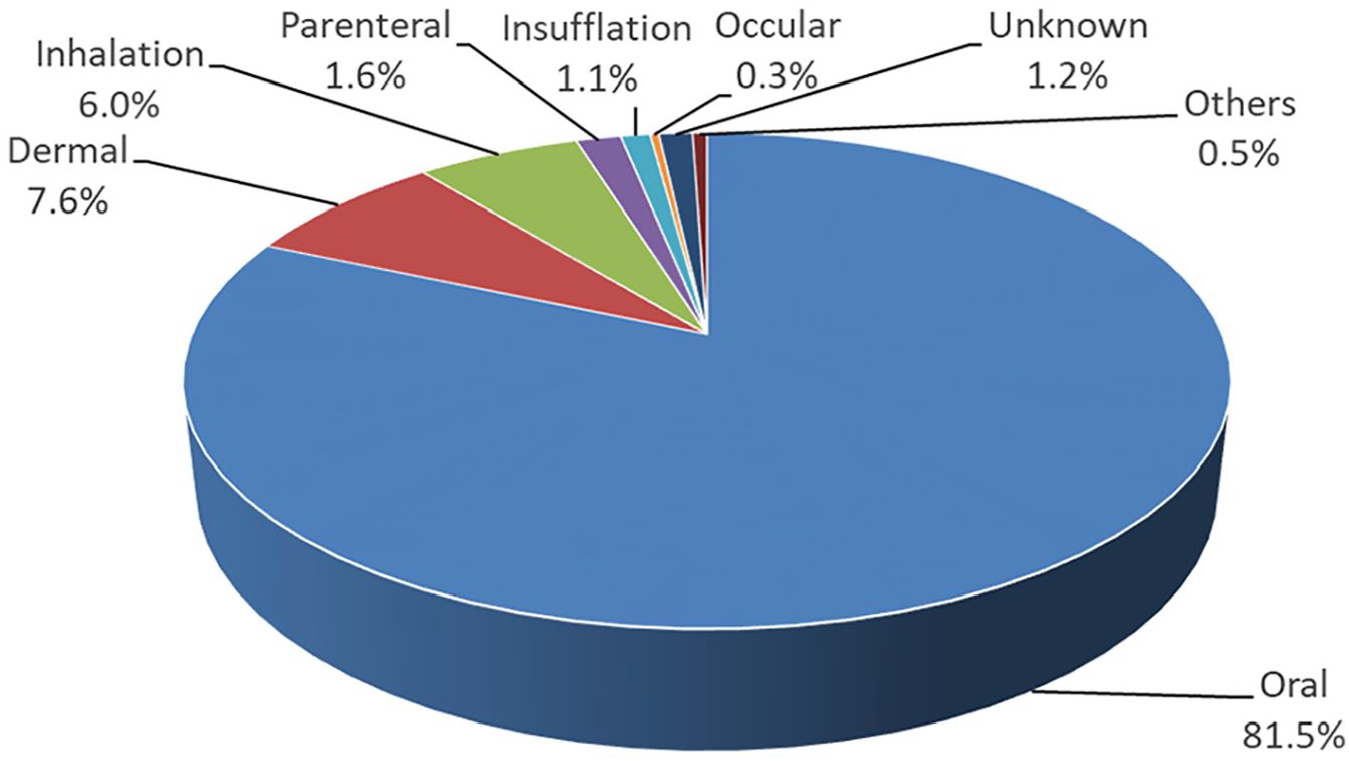
Route of exposure.
A total of 5820 poisons were involved in the 3960 cases. About three-quarters of the cases (72.7%) had exposed to a single poison, while the remaining (27.3%) cases had exposed to multiple poisons. Types of poison exposure are shown in Figure 5. Apart from ethanol which was commonly involved as a co-ingestant, the five commonest types of poison were benzodiazepines (397 cases), paracetamol (337 cases), Chinese herbal medicine (CHM; 319 cases), household products (307 cases) and zopiclone (295 cases).
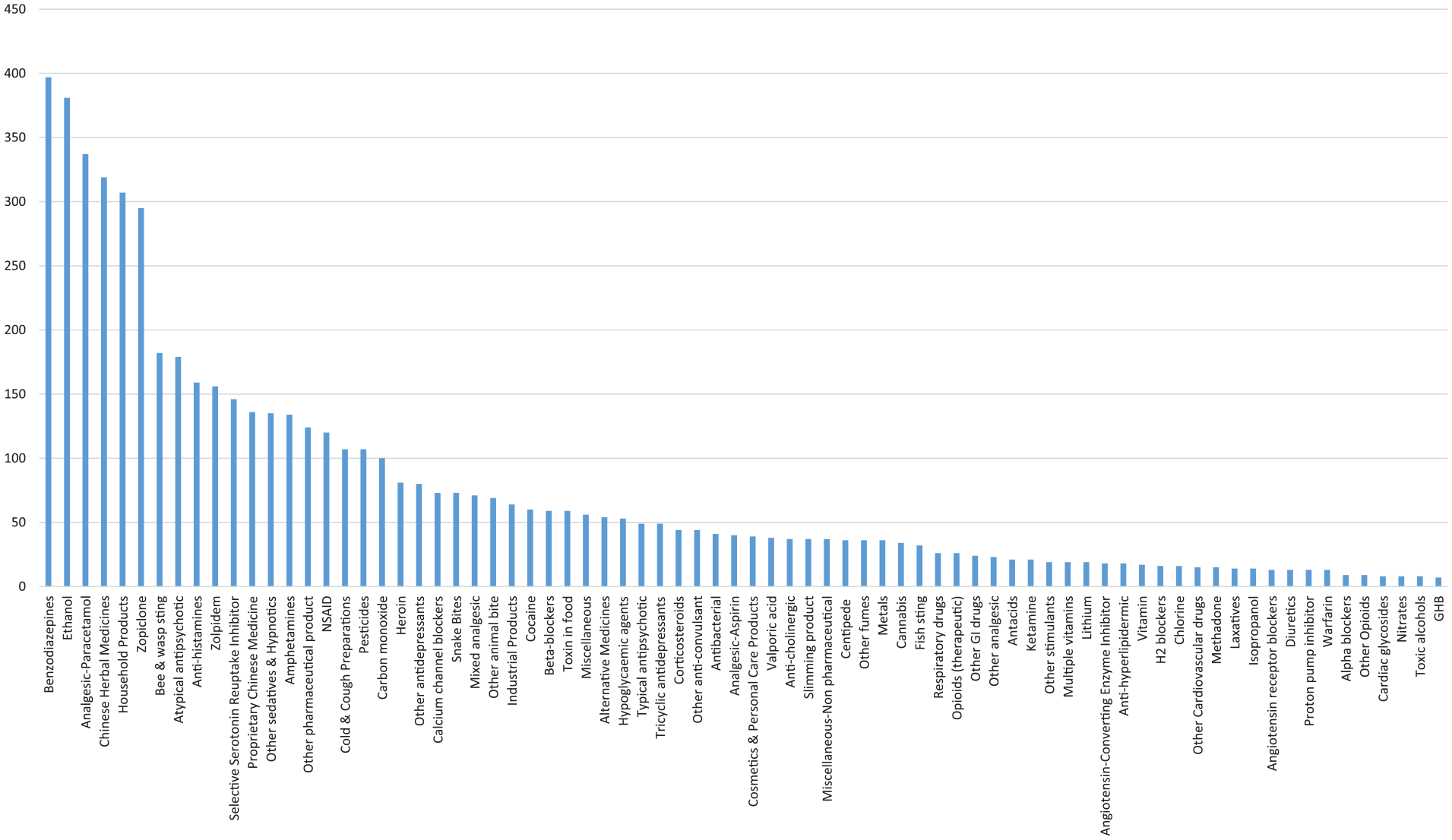
Type of poison exposed.
For the analysis on the management in terms of decontamination and antidote uses, only the consultation cases were included. For the 2041 consultation cases, 275 (13.5%) patients underwent decontamination, including 23 of them given multiple decontamination methods. The commonest method was single-dose activated charcoal (AC) (90.9%), followed by gastric lavage (9.5%) and multiple-dose activated charcoal (MDAC) (5.5%) as shown in Table 2. Regarding the antidote use, 280 (13.7 %) patients were treated with antidotes and 36 of them were given more than one antidote. The five commonest antidotes used were N-acetylcysteine (NAC), benzodiazepines, snake antivenin, calcium and sodium bicarbonate as listed in Table 3.
Decontamination.
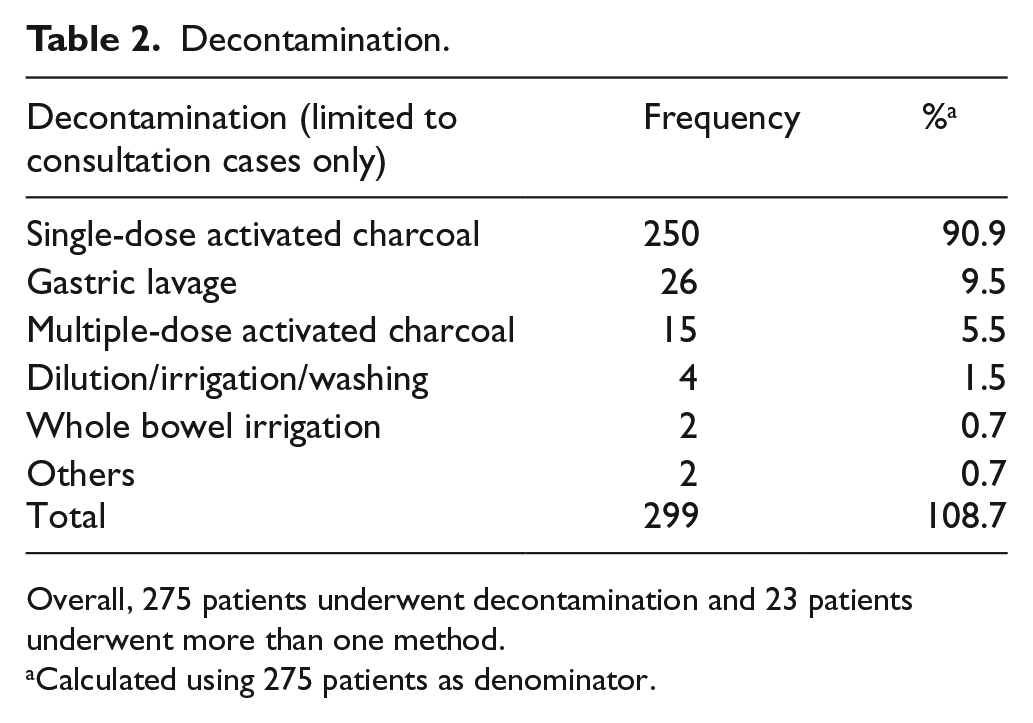
Overall, 275 patients underwent decontamination and 23 patients underwent more than one method.
Calculated using 275 patients as denominator.
Antidote.
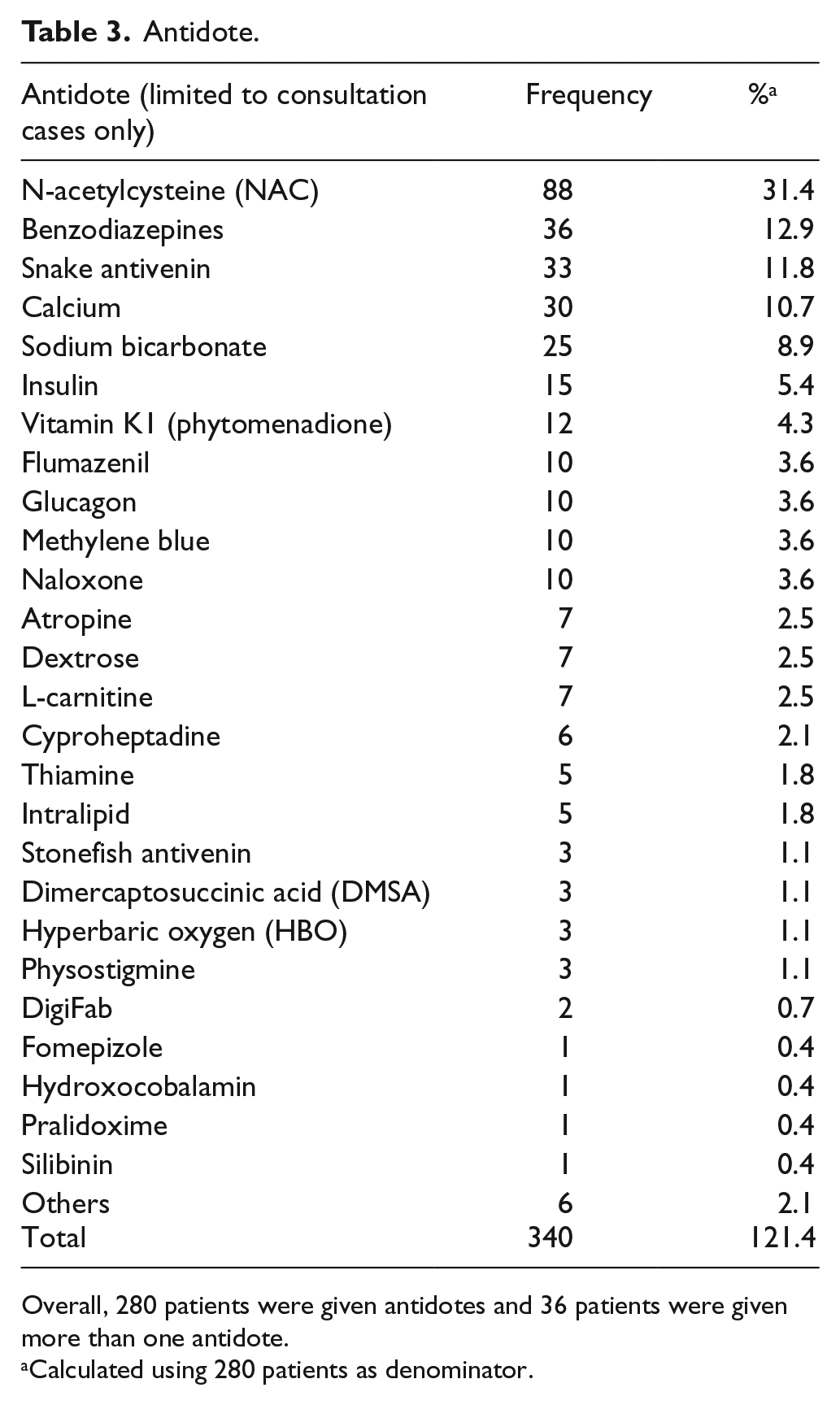
Overall, 280 patients were given antidotes and 36 patients were given more than one antidote.
Calculated using 280 patients as denominator.
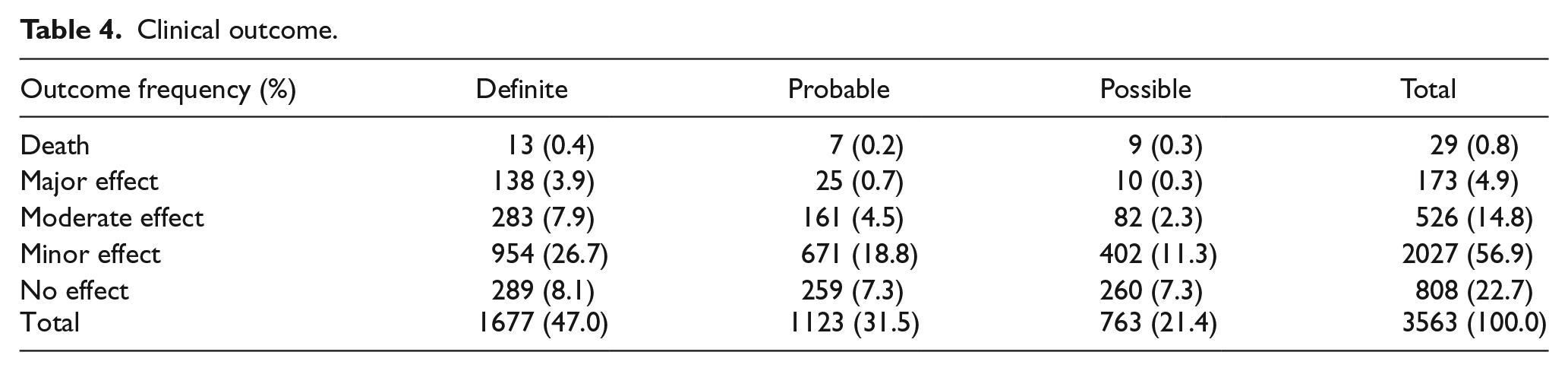
After excluding 397 cases in which the clinical outcomes were graded as not related to the poison exposure, or clinical outcome could not be assessed from the available information, the remaining 3563 cases (100%) were analysed for the outcome. There were 29 deaths (0.8%), 173 cases of major effects (4.9%), 526 cases of moderate effects (14.8%), 2027 cases of mild effects (56.9%) and 808 cases of no effect (22.7%) as shown in Table 4. As for the relationship between poison exposure and the outcome, 47.0%, 31.5% and 21.4% of the outcomes were graded as definitely, probably and possibly related to the poison exposure, respectively.
Clinical outcome.
In 2018, we received 251 consultations on pre-hospital AC administration. Among these 251 patients, 145 (57.8%) patients were given AC by ambulance paramedics. The remaining 106 (42.2%) patients were either not indicated for AC administration or judged to be not feasible for AC administration during the ambulance transfer.
Discussion
This 13th annual report of HKPIC analysed the data of 3960 poisoned cases in 2018 which represented the most updated poisoning pattern in Hong Kong.
The poisoning reporting is not compulsory and it remains one of the intrinsic limitations in our poisoning data, which is common to other poisoning databases in developed countries. However, HKPIC recorded around 4000 cases yearly, with comparable figures of death and major outcomes over the past few years. We believe that we have captured the majority of poisoning cases for analysis.
The age and gender distribution, and routes of exposure were grossly similar when compared with our previous reports and overseas data.1,2 Last year, we reported a mildly increased proportion in teenage group (13–19 years, from 6.3% in 2016 to 7.6% in 2017) and elderly group (>80 years, from 3.9% in 2016 to 4.7% in 2017). The proportion in teenage group further increased to 8.9% this year and the elderly group remained static at 4.7%. Although there is an increasing trend of poisoning in the teenage group in recent years, it is still within the proportion of our past available records in which before year 2009, the teenage group was involved in > 9% of the total poisoning case. Having said that, this increasing trend of poisoning in teenage group may represent a potential public concern and needs further monitoring.
The three commonest reasons of exposure, namely suspected self-harm, unintentional exposure and substance abuse, remained the same as the data of the previous years.
The five commonest types of poison exposure were benzodiazepines, paracetamol, Chinese herbal medicine, household products and zopiclone. According to our previous HKPIC data, these five types of poison had remained the five commonest exposed poisons since year 2011, with benzodiazepines and paracetamol ranked either the first or second commonest poisons since 2010, each involved in 8%–10% of all poisoning cases. Benzodiazepines had outnumbered paracetamol and remained as the commonest poison for 3 years since year 2016. Although zopiclone dropped from the third commonest last year to fifth commonest this year, it was still the second commonest single poisoning agent in Hong Kong while paracetamol being the commonest, mostly because it is readily available in both over-the-counter and prescribed preparation. Paracetamol, together with benzodiazepines and zopiclone poisoning, commonly occurred in intentional self-harm, as a sole poison or co-poison in multiple poisons exposure. For Chinese herbal medicine poisoning, around one-third was related to herb-induced liver injury, followed by herb-related renal injury or aconite poisoning in 2018. Household products were commonly encountered in intentional overdose in adults as well as accidental exposure in children. Cleansing agents, bleaches, antiseptics and desiccants/oxygen absorbent were the commonest poisons involved in household products.
Unlike last year in which we reported a higher than average decontamination rate (17.4% compare with the 5-year average of 15.5%), 2 the decontamination rate dropped significantly to 13.5% this year. Concerning the method of decontamination, the use of single-dose AC remained the commonest method as expected from our local experience and oversea poison centre data.1,2 The proportion of antidotes (13.7%) was about the same as the average of 14.2% in the previous 5 years. The reason for the abrupt decrease in proportion of decontamination in 2018 needs further monitoring.
Among all types of antidotes, NAC, benzodiazepines and snake antivenins were the three commonest used antidotes. NAC has been the commonest antidotes in all of our previous annual reports except in 2008. NAC was given in around one-fourth of paracetamol poisoning cases. It may also be used to treat other poisonings, such as amatoxin and paraquat, with limited evidence. Concerning benzodiazepine uses, the exceptional high proportional uses in year 2017 (22.1%) 2 is believed to be an isolated event as it did not sustain in this year (12.8%), which was similar to year 2016 (12.8%). Snake antivenins, calcium and sodium bicarbonate ranked third, fourth and fifth mostly used antidotes. The pattern of their uses was similar and together accounted for about 30% of cases treated with antidotes.
Concerning the clinical outcome, the poisoning death rate in 2018 was 0.8%, which was similar to the average in the past 5 years of 1.0% (Table 5). The proportion of major effect was 4.9% and remained comparable in recent years with an average of 4.5%. Meanwhile, majority of cases (79.6%) were classified as no effect or mild effect, which again was similar to our data in the recent years.
The HKPIC annual reports important figures in the latest 5 years.
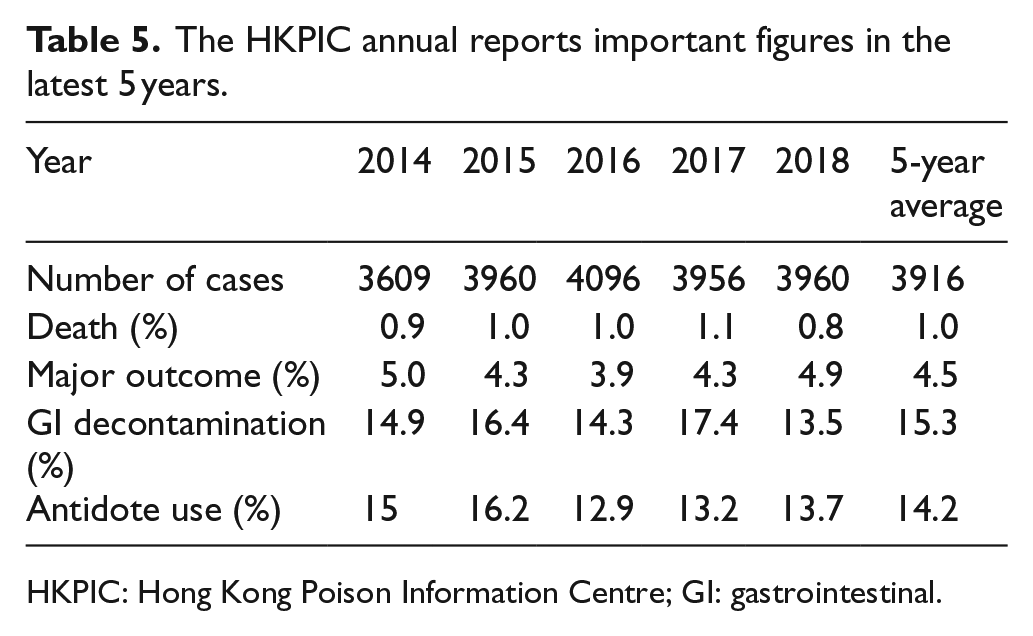
HKPIC: Hong Kong Poison Information Centre; GI: gastrointestinal.
There are limitations in this report as mentioned in our previous annual reports. First of all, reporting of poisoning cases in Hong Kong is on a voluntary basis. Second, the data obtained from the consulting medical professionals may not be comprehensive. However, as most of the poisoning cases were managed in HA hospitals with the patient’s clinical records accessible in ePR, the accuracy and amount of information were expected to be much better than data obtained from other poison centres which may not have direct access to patient records in their managing hospitals. Third, in some of the cases with limited clinical information, it is difficult to make definite judgement on the causal relationship between the outcome and the poison exposure.
Conclusion
This 13th annual report provides the most updated epidemiological information on poisoning in Hong Kong in 2018 and highlights some changes in the pattern of poisoning demography, decontamination and antidote use as compared with our previous reports. Concerning outcome, 0.8% and 4.9% of the cases resulted in death and major outcome, respectively. HKPIC will continue to monitor the poisoning pattern in Hong Kong to facilitate the formulation of strategies in poison control and prevention.
Interesting cases
Case 1 – Octopus bite
A woman in her 40s presented to AED because of octopus bite on her right hand. She was a seafood seller in wet market and was accidentally bitten by a hand-sized red-coloured common edible octopus while removing it from a tank barehandedly. She complained of immediate onset of severe pain and numbness over the bite wound. Physical examination at around 1 h after the accident showed a single small bite wound with no skin loss over the right palm near the base of the right little finger (RLF). There was localized erythema and swelling over the wound, which extended to the hypothenar eminences proximally and the little, ring and middle fingers distally. X-ray of right hand showed no embedded foreign body. Immersion of the right hand in hot water at 40°C–45°C was given for pain control, together with oral diclofenac and antibiotics cover. Pain improved shortly after hot water immersion (HWI) commenced. However, 4 h after the accident, the patient developed urticaria over right hand and right periorbital region. She was treated with intravenous chlorpheniramine and hydrocortisone as suspected allergic reaction. The wound swelling and urticaria were resolving after 24 h and the patient was discharged home. Follow-up at 1 week showed persistent mild pain and swelling around the healed wound, with limited range of movement of RLF. The pain and swelling gradually resolved over 8 weeks in subsequent follow-ups.
Based on the photo taken by the patient, the octopus involved was identified as a common octopus (Octopus vulgaris). It has a beak with its mouth at the centre point of the eight limbs. Although octopus seldom bites, its beak can inflict lacerations to human, where the venom contained in the salivary gland penetrates the body.3,4 The venom contains digestive enzymes and proteinaceous neurotoxins that immobilize prey. With the exception of the tetrodotoxin found in blue-ringed octopus, the common octopus venom causes paralysis in crustaceans but not in human. 5 There are no confirmed reports of paralysis after common octopus’s bite or consumption. Similar to our case, octopus bite wound was reported in causing persistent swelling and erythema lasted for about 1 month. 3 Although there was no microbiological or histopathological examination performed in our case or the case report in the literature, the clinical progress was not typical of that of wound infection. We believed that prolonged local reaction was probably inflicted by the octopus’s venom. For the clinical management, we would recommend octopus bite to be managed similarly as venomous fish sting. General wound care, tetanus prophylaxis, pain control, prophylactic antibiotic with Vibrio species cover (e.g. Augmentin and doxycycline) and HWI 6 are recommended as initial management. The allergic reaction occurred upon initial presentation was probably related to diclofenac exposure, as the patient was later diagnosed to have nonsteroidal anti-inflammatory drug (NSAID) allergy after ibuprofen use.
Case 2 – Water-repellent shoe spray
A man in his 40s presented with acute onset of cough and shortness of breath after using a water-repellent shoe spray. He applied the shoe spray over several pairs of shoes in a poorly ventilated indoor area for about 15 min. He started to develop respiratory symptoms 1 hour later. He was found to have tachypnoea with respiratory rate of 28 breaths per minute and oxygen desaturation (SpO2 of 85%) in room air. Chest auscultation was normal. Chest X-ray (CXR) showed bilateral lower zone haziness which was compatible with the clinical diagnosis of chemical pneumonitis. The patient has no history of underlying lung disease and he was a non-smoker. Blood tests showed increase in white cell count of 19.4 × 109/L with neutrophil predominance. Electrocardiogram, cardiac troponin and nucleic acid testing of nasopharyngeal aspirate for common respiratory viral infections all showed unremarkable findings. The patient’s symptoms were partially relieved after receiving oxygen and salbutamol inhaler in AED. He was admitted to medical ward for close observation and empirical antibiotic was given to prevent secondary bacterial chest infection. His symptoms improved and CXR bilateral lower zone haziness cleared up within 2 days after admission. He was then discharged home but lost to subsequent follow-up.
The water-repellent shoe spray used by the patient has no ingredients information on the product label. It was an aerosol spray labelled as extremely flammable and has to be used in places with adequate ventilation. Based on case reports in the literature, inappropriate uses of commercially available aerosol water repellants have caused multiple outbreaks of chemical pneumonitis.7–11 These reports typically described a syndrome with rapid onset of cough, pleuritic chest pain, shortness of breath and diffuse pulmonary infiltrates in CXR shortly after aerosol water repellant exposure. The condition is clinically self-limiting and typically completely resolves in 1–2 days. It has been demonstrated that the aerosol generates ultrafine respirable particles that deliver the ingredients of water repellent to lower airways. 11 The ingredients, typically solvents and fluorocarbon polymers, disrupt pulmonary surfactant function, which result in diffuse alveolar collapse and the above-mentioned clinical presentation. 11
Case 3 – Illicit drug purchased in ‘Darknet’
A teenage boy with a history of depression presented to AED because of suicidal idea. He was fully conscious and claimed to have taken half bottle of whisky and four tablets of alprazolam. During observation in AED, he went to the toilet and injected intravenous drug into his left forearm vein. The event was discovered shortly afterwards when he was found collapsed in the toilet with a used syringe next to him. Physical examination revealed opioid toxidrome with impaired consciousness, pin-pointed pupils and respiratory depression. A total of 0.8 mg intravenous naloxone was administered and the patient regained full consciousness. Bedside urine immunoassay was positive for benzodiazepine and morphine. The boy claimed that he had injected 100 mg heroin in toilet to kill himself. He was then admitted to paediatric intensive care unit (PICU) and was treated with naloxone infusion for 1 day.
Upon further history taking, the boy disclosed that he planned to kill himself since several months ago. He bought 800 mg of morphine and 1 g of heroin from an Internet network called ‘Darknet’. Within the past 2 months, he has several unsuccessful suicidal attempts by injecting escalating doses of morphine. On the day of presentation, he decided to kill himself with heroin which is pharmacologically more potent than morphine. As this method in obtaining illicit drugs was rarely reported in Hong Kong, the case was reported to the Department of Health (DH) for further investigation. ‘Darknet’ is an encrypted part of the Internet which was only be assessable by specific browsers. Within the ‘Darknet’, illicit drugs could be purchased by cryptocurrencies (e.g. Bitcoin) and delivered through mail order anonymously. 12 This case illustrated a non-conventional mode of drug trafficking for the new generations. Law enforcement, anti-drug abuse agencies and health care workers should be aware of this new channel of drug trafficking.
Case 4 – Fentanyl transdermal patch
An elderly lady in her 80s was found to have depressed conscious level in the elderly hostel. She had liver tumour on palliative care on fentanyl transdermal patch for a month without other opioid medications, congestive heart failure, atrial fibrillation, complete heart block on pacemaker and chronic obstruction airway disease on long-term oxygen 1–1.5 L/min. Upon examination, she was drowsy with miosis and SpO2 of 98% on oxygen supplement 4 L/min. Eight pieces of fentanyl transdermal patch, each delivering 12 mcg/h fentanyl, were found on the patient (four pieces on her left arm and four pieces on right side of her back), whereas the prescribed dose was four patches every 72 h. The patches were removed and her condition improved with supportive care.
Fentanyl is a potent synthetic opioid µ-receptor agonist and is well absorbed by dermal route. Fentanyl transdermal patch was approved for the control of chronic pain, especially in patients with cancer since the 1990s. It should not be used for control of acute pain or in opioid-naïve patients. Once applied to the skin, maximum fentanyl concentration is reached at around 24 h and the drug would be continuously delivered up to 72 h after application. However, 28%–84% of the total initial fentanyl dose still remains in the patch following 3 days of continuous use and the dose remaining is potentially lethal for an adult. 13 Patients applying new fentanyl transdermal patch without removing the old ones are, therefore, prone to overdose. The used patches should also be discarded properly to avoid accidental intake. In fact, ingestion of a used fentanyl patch has been implicated in a case of paediatric death. 14 Because heat increases absorption of fentanyl transdermally, the patches should not be placed near a heat source (e.g. hot pads, heating blankets).
Patients suspected to have poisoning from fentanyl transdermal patches should be properly examined with clothing removed to look for the patches in some ‘obscure’ areas, such as the back or the axilla. The patches should be removed and oxygen can be applied as necessary to the patients. Titrated doses of naloxone or naloxone infusion should be administered to reverse the fentanyl effect in patients with significant respiratory depression.
Case 5 – Liquorice-induced pseudo-hyperaldosteronism
An elderly man in his 70s with hypertension, ischaemic heart disease and ischaemic stroke was admitted for recurrent hypokalaemia within 2 months. His potassium level was 2.5 mmol/L, with arterial blood gas showing metabolic alkalosis (pH 7.52, pCO2 5.4 kPa, bicarbonate 32.2 mmol/L and base excess 8.5 mmol/L). He did not have gastrointestinal (GI) symptoms all along. On further enquiry, he admitted taking 10–12 pieces of a ‘herbal snack’ daily in the preceding 2 months. The listed ingredients of the snack included liquorice extract powder (甘草萃取粉), kumquat (金棗), citrus skin (橘皮), menthol (薄荷腦) and so on. Liquorice-induced pseudo-hyperaldosteronism was suspected and supported by the patient’s low plasma renin (<0.10 ng/mL/h; reference 0.51–2.64 ng/mL/h) and serum aldosterone levels (<50 pmol/L; reference 83–444 pmol/L). He was suggested to stop taking the snacks, and his potassium level normalized with replacement.
Liquorice contains glycyrrhizic acid that inhibits 11β-hydroxysteroid dehydrogenase type 2 (11BHSD2) enzyme both competitively and by reducing gene expression. 11BHSD2 is responsible for the conversion of cortisol to its inactive 11-oxo-metabolite cortisone. With inhibition of the 11BHSD2 enzyme, cortisol exerts its effect on mineralocorticoid receptors, resulting in a cortisol-induced mineralocorticoid effect (an apparent mineralocorticoid excess or pseudo-hyperaldosteronism) with hypertension, hypokalaemia and metabolic alkalosis. 15
Liquorice is a herb that has been used as Chinese medicine, herbal remedies, sweetener in snacks and beverages. 16 These products are often used by the public for the health benefit without recognizing the potential hazards of overconsumption. The history of its use may also be overlooked by the patients as they did not conceive them as ‘drugs’. Clinicians should have a high index of suspicion in patients with recurrent hypokalaemia and metabolic alkalosis, by actively asking about the history of ‘supplement’ or ‘herbal snack’ use, as cessation of the source of liquorice is necessary to stop the inhibition of 11BHSD2. Some patients may also require potassium replacement and spironolactone therapy in the initial stage of management. 17
Case 6 – Glufosinate poisoning with delayed neurotoxicity
A previously healthy man in his 50s presented to AED 4 h after intentional ingestion of 700 mL glufosinate and 400 mL glyphosate for suicidal attempt. A dose of activated charcoal was given. Initial blood tests showed mild hyponatraemia of 133 mmol/L and mildly raised lactate level of 2.8 mmol/L only. Other baseline blood tests, ammonia level, CXR, electrocardiogram and computed tomography (CT) of the brain were all normal. He remained asymptomatic all along in ward until post-ingestion (PI) 20 h; he complained of diplopia. He then developed generalized tonic-clonic seizure at PI 70 h which was aborted by intravenous Ativan. Thiamine and phenytoin were started. He remained confused afterwards and found to have amnesia in ward for 1 week. Ammonia level was elevated after seizure development and normalized on the next day. CT brain was repeated twice after the onset of diplopia and seizure development, respectively, and were all found to be unremarkable. Magnetic resonance imaging of the brain on Day 5 showed few small T2 and T2 flair hyper-intense foci in bilateral frontal and parietal white matter (largest 3 mm) of non-specific nature as unidentified bright objects. His condition gradually improved and he was discharged on Day 15. Subsequent follow-up showed improved cognitive function with Hong Kong version of Montreal Cognitive Assessment (HK-MoCA) from 15/30 before discharge to 24/30 and 27/30 at PI 1 month and 3 months. Overall, his clinical presentation is compatible with glufosinate poisoning, which was confirmed by his urine toxicology screening showing glufosinate only.
Glufosinate-ammonium is a non-selective herbicide. It works by inhibiting the activity of glutamine synthetase (GS) necessary for the production of glutamine and ammonia detoxification in plants. 18 In humans, it is thought that inhibition of GS would lead to imbalance of glutamine, glutamate and ammonia, and inhibition of glutamate decarboxylase would lead to a decrease in gamma aminobutyric acid (GABA) production. 19 Glufosinate also works as an analogue of glutamate, an excitatory amino acid in central nervous system (CNS). 20 It causes several neurological complications, such as impaired consciousness, convulsions and memory impairment, which may be delayed with a latent period of up to 60 h post-exposure.21,22 The mechanism of delayed onset toxicity is not completely understood. Early features of neurotoxicity include tremor, diplopia and nystagmus, while retrograde and anterograde amnesia have been observed upon recovery. Other features of glufosinate poisoning include GI symptoms, respiratory distress, local airway oedema, hyperammonaemia, metabolic acidosis, deranged liver function and cardiovascular collapse. Treatment is mainly supportive, with close monitoring of cases with neurotoxicity or elevated ammonia level. Although glufosinate poisoning is commonly reported in Japan, South Korea and Taiwan, by far only two cases were reported locally to our centre.
This case illustrates the delayed neurotoxicity caused by glufosinate poisoning. A prolonged period of observation with serial ammonia levels is suggested in managing patient with significant glufosinate ingestion in view of its delayed onset neurotoxicity.
Case 7 – Steroid-adulterated herbal products
A woman in her 60s, with known diabetes, stroke, paroxysmal atrial fibrillation and dilated cardiomyopathy, was admitted for left leg skin abscess and skin necrosis. Ultrasound showed left lower limb deep vein thrombosis after admission. Broad-spectrum antibiotics and low molecular weight heparin were started. However, patient was complicated with septic shock and multi-organ failure requiring ICU admission despite antibiotics treatment and debridement by orthopaedics surgeons. Her condition continued to deteriorate despite maximal support and she finally succumbed on Day 12 after admission. The low morning cortisol level prompted the suspicion of adrenal insufficiency, and IV hydrocortisone replacement was given. Subsequent low dose short Synacthen test showed inadequate response confirming the diagnosis. She reported a history of using herbal pills, herbal cream and traditional Chinese medication prior to admission. Analysis of the products showed presence of dexamethasone and other western medications adulteration (including paracetamol, hydrochlorothiazide, chlorpheniramine and diclofenac) in two types of herbal pills by Toxicology Reference Laboratory (TRL). The case was reported to the DH for further investigations.
Undeclared corticosteroids have been found in different types of herbal products, including proprietary Chinese medicine (pCM), Ayurvedic medicine and homoeopathic medicine, and steroid-adulterated pCMs is a recurring problem in Hong Kong, 23 especially in those used for pain, inflammation, skin problems and respiratory disorders. Prolonged use of such kind of products may lead to serious side effects, such as Cushing syndrome, adrenal insufficiency, increased risks of infection and so on. Physician should maintain a high index of suspicion in patients, especially those who have dramatic improvement of their conditions after using herbal products, and have their adrenal functions being evaluated. All patients with the use of steroid (or other Western medication) adulterated products should be reported to the DH for further actions.
A family of ‘石蠄蚷’ poisoning
HKPIC was consulted on a plant or herb named ‘石蠄蚷’ by the DH. Its sale from a herb store was reported by a mother and her son who had developed nausea, vomiting, dizziness, blurred vision and generalized weakness within half an hour after drinking a decoction made with ‘石蠄蚷’. They described that the experience was similar to heavy alcohol intoxication. The two victims did not seek medical attention and the symptoms subsided after 2 days.
石蟾蜍, 石蠄蚷, 山烏龜 or 地烏龜 are confusing names referring to several herbs made from the root of a few toxic or non-toxic Stephania spp (千金藤屬). It could be Stephania tetrandra (粉防己), a commonly used benign herb or toxic ones like S. sinica (汝蘭), S. epigaea (地不容) 24 and S. yunnanensis (雲南地不容). The toxic species harboured the toxic alkaloid tetrahydropalmatine. Acute intoxication mainly causes GI upset, cardiovascular and CNS depression which could result in death. 25 Long-term intake has been reported to cause liver injury. 26 Subsequent morphological identification and biochemical testing suggested that the 石蠄蚷 involved was the unprocessed root bulb of S. epigaea (地不容).
Including this one, at least three cases of similar poisoning involving five victims were known to have happened in Hong Kong since 2005. In view of the significant acute and chronic toxicities of toxic Stephania spp, preventive measures, particularly focused risk communication with the herb sellers, are advisable. Tightened control over the sales of toxic plant parts as herb or food ingredient should also be considered by the government.
Footnotes
Author contribution
The authors certify that they have each made a substantial contribution so as to qualify for authorship and that they have approved the contents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was applied and judged to be not required by the Research Ethics Committee (Kowloon Central/Kowloon East). Please see the attached letter for your reference.
Human rights
Patients’ right to privacy was not infringed in this study.
Informed consent
Since this is an annual report with no patient contact and intervention involved, written informed consent was considered not necessary by our institution and no patient identifiable data have been included in the manuscript. Our previous annual reports were also published in this journal without informed consent.