
Abstract
Background:
The therapeutic hypothermia protocol for out of hospital cardiac arrest is not standardized and the decision to apply therapeutic hypothermia relies on a physician’s judgment. Elderly patients who rely on this judgment are less likely to receive therapeutic hypothermia.
Objectives:
This study aimed to provide an analysis of the impact and utility of therapeutic hypothermia on elderly out of hospital cardiac arrest.
Methods:
This was a multicenter, retrospective, observational, registry-based study from 2007 to 2012. Adults who suffered out-of-hospital cardiac arrest and were treated with therapeutic hypothermia were included. We divided the patients into a group of elderly patients 65 years or older and a group of young adults under 65 years old and compared the neurologic outcomes and adverse events after one-to-one matching by propensity score.
Results:
In total, 930 patients were enrolled in the study. Among these patients, 343 were ⩾65 years, while 587 were <65 years. Of the adverse events in therapeutic hypothermia, hyperglycemia (51.31%), hypotension (41.98%) during cooling was more frequent in aged ⩾65 years and rebound hyperthermia (7.14%) and hypotension (29.93%) during rewarming. After propensity score matching was applied to all subjects of the study, 247 matched pairs of patients were available. The two groups showed no statistically significant difference in the adverse events during therapeutic hypothermia.
Conclusion:
Elderly patients exhibited a decreased survival to hospital discharge and good neurologic outcomes. The two groups showed no differences in the frequency of adverse events during therapeutic hypothermia, when comparing in a propensity score matching cohort analysis.
Introduction
Elderly patients experience major debilitating and life-threatening conditions, but the relative contribution of age to disease course has yet to be fully understood. Some authors have suggested that instead of age, pre-morbid health status should be utilized for medical decisions related to the intensity or goals of treatment. 1 Treatment guidelines for elderly patients are grounded in insufficient evidence and are often excluded from randomized clinical trials because of their age or comorbid medical conditions.
Therapeutic hypothermia (TH) improves the survival rate and neurological convalescence and has emerged over the past 10 years as a new treatment only because of incomplete compliance for comatose patients after out-of-hospital cardiac arrest (OHCA). 2 In a recently disclosed target temperature management (TTM) trial, which dealt with a study of unconscious patients with OHCA, the effect of maintaining the target temperature at 33°C failed to show any noteworthy advantages compared with that when maintaining the target temperature at 36°C.3,4 Nevertheless, a number of hospitals use TH to a certain extent. Because the protocol is not standardized, physicians apply TH using various methods and scopes, and the decision to apply TH relies on a physician’s judgment. Elderly patients who rely on this judgment are less likely to receive advanced interventional procedures, including TH, during recovery from cardiac arrest. 5 Moreover, patients who are 75 years or older have been excluded from several studies on TH; thus, insufficient research has been conducted on the influence of TH in elderly patients.
In this study, we compared the impact of TH in an elderly patient group with a young adult group and discuss the usefulness of TH performed on elderly patients.
Methods
Study design
This was a multicenter, retrospective, observational, registry-based study utilizing the Korean Hypothermia Network (KORHN) registry data. KORHN investigators collected data from adult (⩾18 years) OHCA patients who received TH in 24 teaching hospitals throughout South Korea from 2007 to 2012. The institutional review board of each institution approved the study protocol before data collection began. Informed consent was waived because of the retrospective nature of the study.
Adults who suffered OHCA and were treated with TH after return of spontaneous circulation (ROSC) in the emergency department (ED) were included. The data form, standard definitions of 87 variables, and the investigator manual were developed according to a literature review and consensus of the study investigators. The registry data were collected by manual medical chart or electronic medical record reviews. The collected data in each hospital were verified for completeness by the site principal investigator and recorded in a web-based data registration system by the site clinical research coordinator. 6
Study patients and variables
This study included all patients listed in the registry. We divided the patients into a group of elderly patients aged above 65 years and a group of young adults aged below 65 years. Data included covariates, such as basic demographics, resuscitation variables and post-resuscitation variables, adverse events, and concomitant treatments during TH and the advanced critical care period. Adverse events were divided into three phases: cooling-related, rewarming-related, and advanced critical care-related.
Outcome measures
The primary endpoint of the study was hospital mortality. A good neurological outcome at hospital discharge was defined as a Glasgow–Pittsburgh Cerebral Performance Categories (CPC) score of 1 and 2. Secondary outcomes included the incidence of adverse events during cooling, rewarming, and advanced critical care. To adjust for differences in the baseline characteristics of each group, we performed one-to-one matching using the propensity score.
Finally, the outcomes were reevaluated in the propensity score matched cohort.
Statistical analysis
We used the chi-square, Fisher’s exact, and Wilcoxon rank-sum tests as appropriate for univariate comparisons of differences between groups. A multivariate analysis of the relationship between functional outcomes and baseline characteristics was performed using a stepwise logistical regression method. The results are presented as the mean or median difference with p values or odds ratios (ORs) with 95% confidence intervals (CIs). We performed rigorous adjustments for differences in the baseline characteristics of patients using the propensity score. We performed one-to-one matching with the propensity score using the Greedy-matching macro. After propensity score matching, the success of the propensity score modeling was assessed by the standardized difference and the balance between the two groups was evaluated using Student’s t test for continuous variables and a chi-square test or Fisher’s exact test for categorical variables. After estimating the propensity scores, we performed a logistic regression analysis to assess the prognostic factors and adverse events. Less than 5% of missing data were found in the basic demographics, OHCA factors, and adverse events during TH categories. Missing data were assumed to be missing at random and imputed data sets were generated with the Markov Chain Monte Carlo method. Multiple imputation was used in combination with a full model multivariable logistic regression analysis. All statistical analyses were performed using the software package SAS Enterprise Guide 5 or R software version 2.15.3.
Results
Characteristics of the study population
A total of 930 patients who suffered OHCA and were treated with TH after ROSC in the ED were enrolled in the study. A total of 343 patients were ⩾65 years (36.9%), while 587 patients were <65 years. The average age of all subjects was 57.18 years. Among the ⩾65 aged group, the average age was 73.90 years. The male-to-female ratio for each group was not significantly different. For comorbidities, many of the patients aged <65 years were healthy prior to their cardiac arrest, and 174 patients (50.7%) of the patients aged ⩾65 years had at least two underlying diseases. Regarding pre-hospital factors, 71.4% of the patients aged ⩾65 years had a witnessed cardiac arrest, but the two groups showed no difference in implementation of bystander cardiopulmonary resuscitation (CPR). The first monitored rhythm was ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT) and OHCA with cardiac causes showed a high percentage in the <65 years aged group. The average time from cardiac arrest to ROSC was 33.3 and 33.2 min in the ⩾65 and <65 groups, respectively (not significantly different; Table 1). A total of 367 (62.5%) and 163 (47.5%) patients recovered spontaneous respiration within 72 h following ROSC (a significantly higher percentage in the <65 years group). Regarding neurological function after ROSC, the Glasgow Coma Scale (GSC) for the patients aged ⩾65 years was 3.22 (±0.86), which was statistically significantly lower than that for patients aged <65 years (3.54 (±1.18)). In addition, fewer elderly patients tested positive in the pupil light reflex and corneal reflex (45.67% vs 31.2%, p < 0.001% and 35.8% vs 23.6%, p < 0.001, respectively).
Basic demographics and OHCA factors of each age group in the overall cohort and in the propensity-matched cohort.
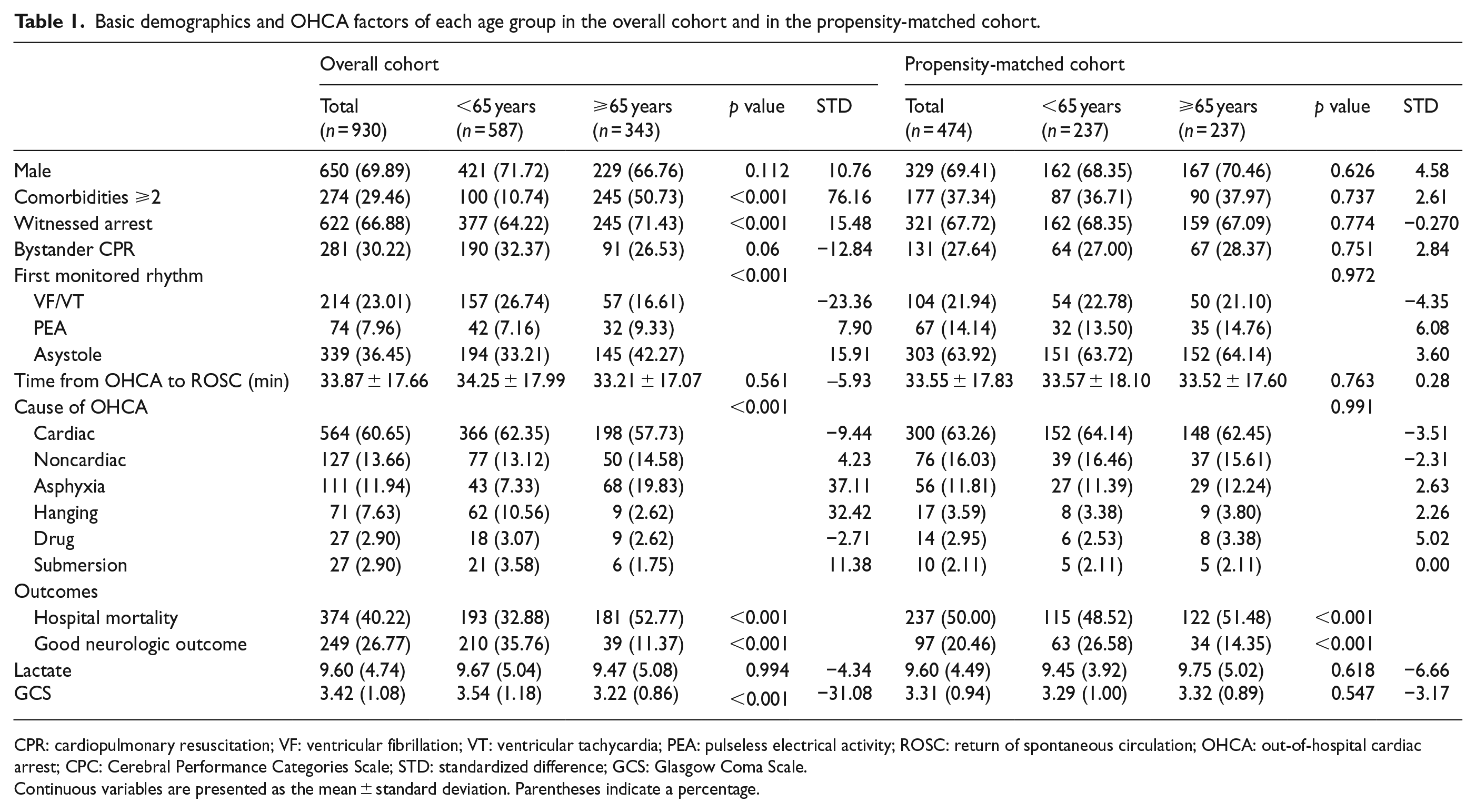
CPR: cardiopulmonary resuscitation; VF: ventricular fibrillation; VT: ventricular tachycardia; PEA: pulseless electrical activity; ROSC: return of spontaneous circulation; OHCA: out-of-hospital cardiac arrest; CPC: Cerebral Performance Categories Scale; STD: standardized difference; GCS: Glasgow Coma Scale.
Continuous variables are presented as the mean ± standard deviation. Parentheses indicate a percentage.
Adverse events during TH
Adverse events during TH are shown in Table 2. The two groups were not significantly different in the occurrence of cardiogenic shock and hypoglycemia. Of the adverse events that occurred during the cooling phase, hyperglycemia and hypotension were observed more frequently among patients aged ⩾65 years than among patients aged <65 years. During the rewarming phase, rebound hyperthermia and hypotension occurred more frequently among patients aged ⩾65 years than among patients aged <65 years.
Adverse events during TH of each age group in the overall cohort and in the propensity-matched cohort.

TH: therapeutic hypothermia; SBP: systolic blood pressure; MAP: mean arterial pressure.
Parentheses indicate a percentage. Pulmonary complication; pneumothorax, pulmonary contusion, hemothorax, aspiration, and pulmonary edema; cardiogenic shock, hypotension (SBP < 90 mmHg or MAP < 60 mmHg for at least 30 min or the need for supportive measures to maintain an SBP > 90 mmHg or MAP > 60 mmHg) and end organ hypoperfusion.
There was a significant difference in the reason for stopping TH between the two groups. Among patients aged <65 years, TH was discontinued due to shock, arrhythmia, and other causes, while not attempting resuscitation (DNaR) was the major cause among patients aged ⩾65 years.
Adverse events related to infections and lungs occurred more frequently among patients aged ⩾65 years than among patients aged <65 years. Infection, sepsis, and pneumonia occurred in 50.15%, 21.87%, and 43.73% patients aged ⩾65 years, who were treated with TH. The incidence of these adverse events in elderly patients was significantly higher than that in patients aged <65 years (38.67%, 14.65%, and 33.22% for infection, sepsis, and pneumonia, respectively).
After propensity score matching (propensity score matching is used to reduce bias in nonrandomized and observational studies) was applied to all subjects, 247 matched pairs of patients were available (Table 3). The matched cohorts did not show any age-specific differences related to basic demographics, OHCA factors, or adverse events. The two groups did not significantly differ regarding the incidence of adverse events during TH (which was different from the results before matching). Cardiogenic shock, hypoglycemia, adverse events during the cooling and rewarming phases, infection, and pulmonary events did not show any age-specific differences after propensity score matching.
Multivariate logistic regression analysis of predictors for good neurological outcome of each group with survival hospital discharge.

CI: confidence interval; OR: odds ratio; OHCA: out-of-hospital cardiac arrest; CPR: cardiopulmonary resuscitation; ROSC: return of spontaneous circulation; VF: ventricular fibrillation; VT: ventricular tachycardia; PEA: pulseless electrical activity; GCS: Glasgow Coma Scale.
Parentheses indicate a percentage.
Univariable logistic regression.
Multivariable logistic regression.
Predictors of neurological outcomes and survival to hospital discharges
Of the 930 patients, 556 patients survived to discharge. A total of 394 patients were aged <65 years, and 162 patients were aged ⩾65 years. A total of 210 patients (53.3%) aged <65 years and 39 patients (24.1%) aged ⩾65 years had a good neurologic outcome (Table 1). There was a significant difference in the cause of death between the two groups. Multi-organ failure (MOF) was the most common cause of death in both the groups, but hypoxic brain damage and MOF were similar among patients aged <65 years.
With the age of 65 at the center of the analysis, factors related to good neurologic outcomes were compared for survival to hospital discharge. Among patients aged <65 years, patients with good neurologic outcomes were significantly more likely to be young or male. However, patients aged ⩾65 years characteristically showed that age and gender were unrelated to good neurologic outcomes. Of the patients aged <65 years, those who had been healthy before they suffered cardiac arrest, those with fewer comorbidities, those with a witnessed cardiac arrest, and those who received bystander CPR showed good convalescence, and these characteristics were not found for patients aged ⩾65 years. Of the adverse events that occurred during TH, hypoglycemia, hyperglycemia, and infection were factors specific to convalescence for patients aged <65 years. For patients aged ⩾65 years, bradycardia and tachyarrhythmia were significant factors for their convalescence.
In the multivariate logistic regression model for good outcomes that included basic demographics, resuscitation and post-resuscitation variables, adverse events and concomitant treatments during TH (Table 3), good outcomes were more common among patients who had been previously healthy, who recovered spontaneous respiration within 72 h, who underwent coronary angiography, and who had a pupil light reflex at any time among patients aged <65 years. For patients aged ⩾65 years, coronary angiography or the use of a paralytic agent were highly related to good outcomes.
Trend of good neurologic outcomes during the study period
The number and ratio of patients who survived to discharge from the hospital with good neurologic outcomes specific to age during the study period are shown in Figure 1. In 2007, TH was applied to 39 patients. In 2012, TH was applied to 375 patients, which was nearly a 10-fold increase. The percentage of patients with good neurologic outcomes was 33.3% (2008) at the minimum and 63.2% (2007) at the maximum among patients aged <65 years; thus, no statistical significance was found during the study period. For patients aged ⩾65 years, the percentage of patients with good neurologic outcomes increased from 0% (2007) to 32.1% (2012), which was statistically significant.

Trend of good neurologic outcomes of patients who were survival discharge from hospital during the study.
The percentage of patients who survived to hospital discharge and good neurologic outcomes were higher among patients aged <65 years. In the earlier results, the aged ⩾65 years group exhibited a significant increase in good neurologic outcomes during the study period, but the outcomes during the entire study period indicated better outcomes for patients aged <65 years. For patients aged <65 years, 53.3% of the survival-to-hospital discharge patients showed good outcomes, whereas among patients aged ⩾65 years, only 24% showed good outcomes. In the univariable Cox proportional hazards regression analysis, the hazard ratio (HR) for patients aged ⩾65 years was 1.92 (1.57–2.36). In the propensity score regression analysis, the HR was 1.42 (1.03–1.96) (Figure 2).
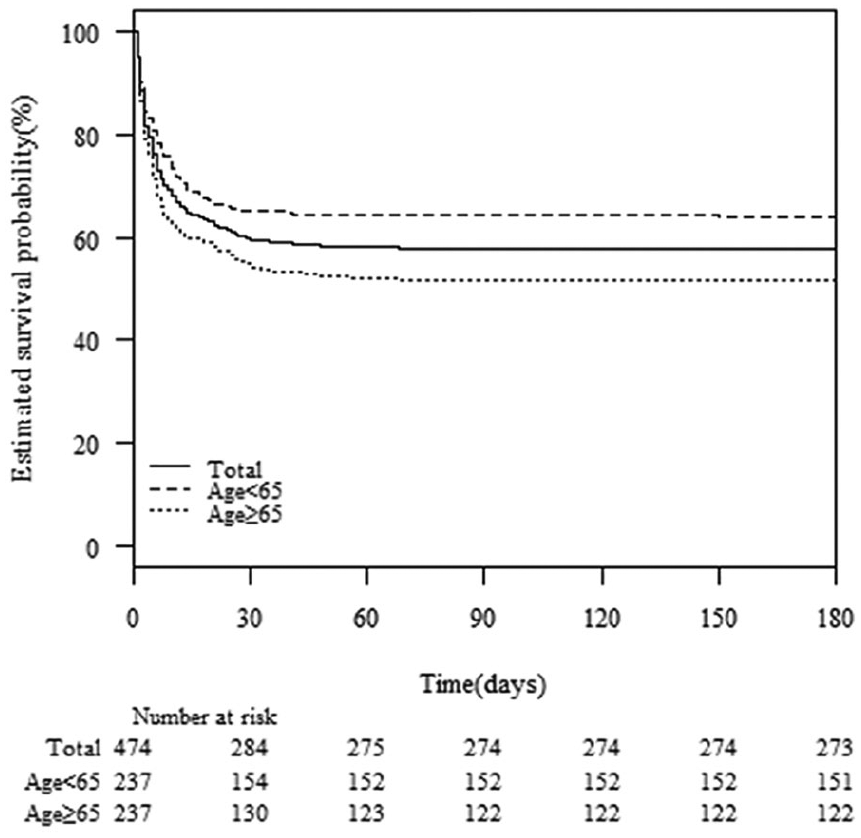
Kaplan–Meier plots for survival discharge from hospital patients after propensity score matching cohort.
Discussion
We compared OHCA patients receiving TH who were 65 years or older with those who were 64 years or younger in terms of the neurological prognosis, the effect of TH, and the percentage of patients who experienced adverse events. In our study, patients 65 years or older experienced a higher level of mortality with poorer neurological outcomes than patients 64 years or younger. However, the propensity score matching analysis confirmed that the adverse events from TH had no age-specific differences. While showing poorer neurologic outcomes compared with patients 65 years or younger, patients 65 years or older experienced a continuous increase in good neurologic outcomes during the study period. As a result, even though aged patients registered higher post-OHCA mortality and a poor prognosis, our results suggest that active post-cardiac arrest care, such as TH, can significantly improve the outcomes of high-risk patients.
While there is controversy over whether the mortality rate of OHCA patient increases with age, our results are similar to those of several earlier studies.7 –10 In a single-center observational study that included 54% of patients 60 years or older and 21% of patients who received TH, age was not as a simple comorbidity marker, but instead as an independent prognostic factor for OHCA patients. 11 However, the study did not include various confounders presented in The Utstein Style, such as pre-hospital elements, and it differed from this study, as it did not limit study subjects to TH treatment. A recent large-scale population-based study on 30-day mortality in elderly patients with OHCA showed that advanced age was an independent predictor of mortality in OHCA patients over 70 years of age. 12 In addition, in the multivariate analysis, the 30-day survival rate increased for cardiac etiology, bystander witnessed arrest, and VF as first recorded rhythm. This study compared OHCA patients who were 70 years or older with those 70–79 years, 80–89 years, and 90 years or older.
In contrast to our research, recently disclosed studies considering the age of OHCA patients and outcomes reported good neurologic outcomes for elderly patients who survived after OHCA. In a study on OHCA patients who were 75 years or older, 25% of the patients discharged from the intensive care unit (ICU) survived and that one-third of the patients survived 5 years later. 13 However, a post hoc substudy published by a clinical trial group for TTM reported that age was related to mortality, even after adjustment for confounding factors, and that focusing on survival rate increased the likelihood that elderly patients had worse neurologic outcomes. 14 While the subjects in the TTM trial group differed from our study subjects, the findings were similar: mortality and poor neurologic outcomes were more prevalent among elderly patients than younger ones. The authors found that an increase in mortality associated with each year’s increase in age resulted in an HR of 1.04. The HR was 1.8 and 1.8 when comparing patients 66–70 years old and patients 71–75 years old with patients 64 years or younger, respectively. These results are similar to our calculated HR of 1.92 (95% CI 1.6–2.7). Patients whose first rhythm following cardiac arrest was shockable often achieved excellent results, and patients with non-shockable initial rhythms generally had poor results. 15 In the TTM trial, the initial rhythm was VF among 372 (81.93%) of 454 patients who were 64 years or younger and 357 (73.61%) of 485 patients who were 65 years or older. However, in this study, the initial rhythm was VF in 23% of the patients who were 64 years or younger and in 13.99% of patients who were 65 years or older. Interestingly, despite the difference in initial rhythm, the study subjects showed similar results. Therefore, the results of our study suggest that improving the post-OHCA survival rate of elderly patients requires additional research on the effects and usefulness of in-hospital advanced management according to the initial rhythm of cardiac arrest in an aged patient.
Our study showed that, during the study period, good neurological outcomes increased year after year from 0% to 32.14% for survival-to-discharge patients who were 65 years or older. This is impressive, considering that the neurologic outcomes did not show a difference in survival to discharge for adult patients who were 64 years or younger. These findings are consistent with the previous literature.16,17 The Utstein Osaka Project was a large prospective population-based cohort study of OHCA and reported that 30-day survival with neurologically favorable outcomes after OHCA among elderly patients increased significantly each year. 18 In addition, the SOS-KANTO 2002 and 2012 study showed that 30-day survival and favorable outcomes for elderly OHCA patients increased significantly. 19 When compared with 2002, the percentage of patients who underwent coronary angiography and intervention and TH in 2012 increased from 4.9% to 16.5% and from 2.6% to 15.1%, respectively. Logistic regression analysis confirmed that the improvement in favorable neurological outcomes in 2012 was related to the increased use of advanced in-hospital treatments. In turn, our results confirm that coronary angiography and intervention were related to good neurologic outcomes for both patients 64 years or younger and patients 65 years or older. In addition, these results reaffirmed the importance of pre- and in-hospital treatments as stressed in the OHCA patient treatment guidelines.20,21
The adverse events that occurred during TH were common side effects, such as infection, cardiogenic shock, and hyperglycemia in the cooling phase and hypotension in the rewarming phase. For patients 65 years or older, statistically significant side effects were hyperglycemia; any complication (overcooling, arrhythmia, hypokalemia, hyperglycemia, bleeding, and hypotension) in the cooling phase; hypotension in the rewarming phase; and infection, pneumonia, and aspiration that occurred at any time during the TH period. However, the two groups were not significantly different following propensity score matching. This result is opposite to the prediction that in-hospital advanced management will cause complications that are common with aged patients. While differentiation from the mixing of cases makes direct comparisons problematic, a study with in-hospital cardiac arrest patients reported infectious complications in 43% of cases, with complications occurring during TH of the order of hyperglycemia, pneumonia, fever within 72 h, and bradycardia. 22 In meta-analysis, patients who received TH had an increased risk of developing pneumonia and infection, while they had a small risk of developing sepsis. 23 This is similar to our study in which we observed less risk for sepsis than for infection and pneumonia. The reduced secretion of proinflammatory cytokines and the inhibition of leukocyte migration and phagocytosis due to hypothermia are believed to increase the chances of infection for patients who receive TH. While the inhibition of neurologic inflammation is a neuroprotective mechanism, this can increase the chances of infection. Adverse events frequently occur during TH, but they did not aggravate neurologic outcomes in the results of our study, which agrees with the results of an earlier study that confirmed no relation between adverse events and mortality. 24 In addition, by comparing patients 64 years or younger with those 65 years or older with regard to the development of adverse events through propensity score matching, the two groups were not significantly different. The results of our study will help physicians make decisions when applying TH to aged patients.
Limitations
This study has several limitations. The retrospective, observational nature of this study and the inclusion of subjects from a multicenter registry entail an inevitable risk of selection bias. During the study period, each hospital attempted to collect all OHCA patients treated with TH, but there was an inevitable risk of selection bias. Although we used the standard survey protocol, the risk of bias in this study remains because it was a registry-based multicenter study. In addition, the timing of the implementation of TH and the variability of the TH protocol between the hospitals may have had an impact on the prognosis and adverse events. However, a data manager and three clinical research associates monitored and reviewed the data quality. The site principal investigators or site clinical research coordinators sought to clarify the data by contacting the query function of the system. The data used in this study were collected at hospitals in a single country. Therefore, our results may have limited generalizability. Several data points were missing, which could affect the results, although the data manager and clinical research associates monitored the data and gave feedback to the principal investigators. Finally, we were only able to record neurological outcomes at hospital discharge and were not able to determine long-term outcomes and the study was conducted from 2007 to 2012, which did not reflect the latest trends. KORHN researchers have been conducting a new prospective study since 2016. Further prospective studies will be published in the future.
Conclusion
Elderly patients exhibited decreased survival to hospital discharge and good neurologic outcomes. However, the increasing frequency of TH application to aged patients and the results indicated a good prognosis for this group of patients. Furthermore, the two groups showed no differences in the frequency of adverse events during TH in a propensity score matching cohort analysis.
Footnotes
Author contributions
S.P.C. was responsible for the study execution, data management, and manuscript writing. J.H.P. was responsible for the study design, data interpretation, and manuscript writing. K.N.P., Y.D.S., H.L., and D.H.L. were responsible for data analysis and interpretation of results. All the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The statistical consultation was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI14C1731).
Availability of data
Data are not shared as the data file contains patient identification information.
Informed consent
An individual patient consent was waived in the context of retrospective study. Informed consent was waived because of the retrospective nature of the study. Written informed consent was not necessary because no patient data have been included in the manuscript. And all guardians gave consent for the treatment and examination at the start of therapeutic hypothermia treatment.
Ethical approval
The study was approved by the Institutional Review Board of the Catholic University of Korea, Yeouido St. Mary’s Hospital.