
Abstract
Background:
Background: Serum albumin has been known as a strong predictive value of mortality in various disease conditions, severe burns, major surgeries, stroke, myocardial infarction, etc. But little is known for the effect of serum albumin level on out-of-hospital cardiac arrest patients.
Objectives:
This study aimed to investigate the effect of serum albumin level on the outcome of out of hospital cardiac arrest.
Methods:
This study was a prospective hospital-based patient cohort study, conducted during January to December 2014 at 27 emergency departments in Cardiac Arrest Pursuit Trial with Unique Registration and Epidemiologic Surveillance project. The albumin was measured immediately after arrival to the emergency department during cardiopulmonary resuscitation, and albumin was categorized into two groups, group < 3.5 g/dL group and ⩾ 3.5 g/dL group. The primary outcome was a good neurological recovery at discharge (cerebral performance category scale 1 or 2). Multivariable logistic regression was used for adjusting for confounders.
Results:
During the study period, 1616 out-of-hospital cardiac arrest patients with presumed cardiac etiology were enrolled, and the total of 1013 patients were analyzed in this study. A total 452 (44.6%) patients had serum albumin level less than 3.5 g/dL. The serum albumin ⩾ 3.5 g/dL group showed better neurological outcomes than the serum albumin < 3.5 g/dL group: 18.5% versus 4.0%, and ⩾ 3.5 g/dL group had higher survival discharge rates than the < 3.5 g/dL group: 23.9% versus 9.1% (p < 0.01). After adjusting for potential covariates, patients with serum albumin ⩾ 3.5 g/dL had a higher odds of good neurological recovery (adjusted odds ratio: 2.94 (95% confidence interval: [1.57, 5.49])), and higher survival to discharge (adjusted odds ratio: 1.74 (95% confidence interval: [1.10, 2.76])).
Conclusion:
Low serum albumin levels are associated with a worse neurologic outcome in patients with out-of-hospital cardiac arrest.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a global burden to public health since it has a high incidence and low survival rate.1,2 Although constant efforts have been done to improve the OHCA outcome, the survival rate changed very little in almost 30 years. 3 Furthermore, less than 50% of OHCA survivors discharge from the hospital without major neurological deficits. 4 Patients survived from cardiac arrest shortly undergo cardiac, cerebral dysfunction with a systemic response. This phenomenon is called postcardiac arrest syndrome (PCAS). PCAS is known to have two main pathophysiology. One is an ischemia-reperfusion injury and the other is the activation of the systemic inflammatory response. 5
During cardiac arrest, low oxygen supply causes cellular damage, and reperfusion makes oxygen radicals. And these radicals cause further tissue damages. Albumin plays a key role in protecting our system from such state by maintaining plasma colloid osmotic pressure; delivering several endogenous and exogenous compounds with antioxidant and anti-inflammatory properties; and scavenging reactive oxygen species. 6
Serum albumin has been known to have a strong predictive value of mortality in various disease conditions, severe burns, and major surgeries. 7 Any pathological process such as inflammation, degeneration, or malignancy is related to the use of albumin. Association between serum albumin and a poor outcome is statistically proven in almost every critically ill condition. Postcardiac arrest situation and other critically ill conditions share some common pathophysiology. One of that is an activation of the systemic inflammatory response that is similar to those observed during severe sepsis.8,9 Previous studies showed that hypoalbuminemia is a risk factor of poor prognosis in severe sepsis patients. 10
Considering that low serum albumin level is a well-established predictor of poor clinical outcome in severe stressful conditions, which have similar pathophysiology of postcardiac arrest situation, it is probable that albumin level can be a prognostic factor of the OHCA outcome. However, the results from previous studies are conflicting.11,12 This study aimed to investigate the effect of serum albumin level on the outcome of OHCA, and further identify a high-risk population that is more susceptible to the harmful effect of low serum albumin level.
Methods
Study setting and design
The study protocol was approved by all institutional review boards of 27 participating study institutions, and informed consent was obtained from all responders. This study was financed by the Korea Centers for Disease Control and Prevention (CDC; 2013–2014). This study was a cross-sectional analysis using the Cardiac Arrest Pursuit Trial with Unique Registration and Epidemiologic Surveillance (CAPTURES) study database in Korea. This was a prospective hospital-based patient cohort study, conducted from January to December 2014 at 27 emergency departments (EDs).
The Korean emergency medical service (EMS) system is a single tiered and government-based system, and it provides a basic-to-intermediate service level of ambulances operated throughout 16 provincial headquarters of the national fire department. 13 Emergency medical technicians (EMTs) can provide cardiopulmonary resuscitation (CPR) at the scene and while transporting the patients. They cannot stop CPR or declare death without medical direction from a physician. Therefore, all OHCA patients assessed by EMS providers should be transported to the ED. The Ministry of Health and Welfare designate all EDs into three levels by resource and functional criteria such as staffing, equipment, and department size. Levels 1 (n = 20) and 2 EDs (n = 110) must have emergency physicians 24 h 365 days, and it provides the highest level of emergency service. Level 3 EDs (n = 310) can be staffed by general physicians and provide basic emergency care. All EDs perform CPR and postresuscitation care based on the international standard guidelines. 14
Data source
This study was based on CAPTURES database, which is a prospective multicenter project to identify the relationship between possible OHCA risk factors and its prognostic effect on long-term basis. The CAPTURES project collected information of cardiac origin OHCA patients resuscitated by EMS and transported to EDs, and each ED staff identified OHCA etiology.
Each ED emergency physician interviewed patients’ family face-to-face and filled out the structured survey papers. This article has a patient’s sociodemographic information, past medical history, family history of cardiovascular disease, lifestyle, etc. Study coordinators registered laboratory test and cardiac examination results by reviewing medical record and called patients’ family to identify 6 and 12 months’ long-term outcomes. All collected data were registered to central data server using EpiData Version 3.1 (The EpiData Association, Denmark, Europe).
Study population
The study population was EMS-treated OHCA patients with presumed cardiac etiology who were transported to 27 EDs participating in the study from January to December 2014. OHCA patients whose arrest occurred at nursing homes or clinics and cases with unknown information of serum albumin level were excluded. The project also excluded the patients under 15 years old, with a terminal illness, under hospice care, with pregnancy, living alone or homeless without reliable information source, and with a “Do Not Resuscitate” card.
Variables and measurements
We investigated all potential confounders including age, gender, location of arrest (public, home or healthcare), witnessed arrest, bystander cardiopulmonary resuscitation, initial cardiac rhythm (shockable vs. nonshockable), prehospital defibrillation, response time interval (from EMS call time to EMS arrival time), transport time interval (from EMS arrival time to ED arrival time).
Potential cardiovascular risk factors such as diabetes mellitus, hypertension, and dyslipidemia were collected. When OHCA patients arrived at the EDs, arterial blood gas analysis (ABGA), routine laboratory examinations including serum albumin were done as soon as possible. Study blood samples were taken by an EMT or a nurse in EDs and sent to each hospital’s laboratory room, and the samples were examined by the commercially available laboratory machines. All the laboratories participated in a qualification program such as College of America Pathologist (CAP) survey.
Main exposure of this study was initial serum albumin level during CPR. We categorized serum albumin level to two groups according to normal range of serum albumin level (3.5~5.5 g/dL), group 1 < 3.5 g/dL, which is below normal group, and group 2 ⩾ 3.5 g/dL. We analyzed the impact of elevation of serum albumin level on the survival rate and favorable neurologic outcomes.
Outcome measures
The primary outcome was the favorable neurological outcome at discharge. The secondary outcome was survival to hospital discharge rates. Hospital discharge included discharge to home, discharge to other hospitals, and discharge to hospice or other health care center. Neurological outcome was evaluated according to the Glasgow-Pittsburgh cerebral performance category (CPC) scores. CPC 1 and 2 were classified as a good neurological outcome, and CPC 3, 4, and 5 were categorized as a poor outcome.
Statistical analysis
Categorical variables were analyzed using the chi-square test, and continuous variables were analyzed using the Wilcoxon rank sum test. Continuous variables are presented as median and 25% to 75% interquartile range (IQR). Unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to estimate the effect of serum albumin level on the good neurological outcome, as well as the survival to discharge. Adjusted ORs (AORs) with 95% CIs were calculated using multivariable logistic regression analysis to adjust the effects of serum albumin level and potential risk factors such as age, gender, prearrest comorbidities (diabetes, hypertension, dyslipidemia), witnessed the arrest, bystander CPR, the location of arrest, EMS defibrillation, EMS ECG (electrocardiography). In addition, we put an interaction term of patient characteristics and albumin level to the multivariable logistic regression model to estimate the effect of albumin changes by the patient characteristics on the study outcome. Age (below 65 years vs. above or equal to 65 years), sex (male vs. female), diabetes, cholesterol level (below 200 mg/dL vs. above or equal to 200 mg/dL) were included in those patient characteristics. If there is an interactive effect between patient characteristics and albumin, the AOR of albumin on the study outcomes would be different across a patient with those characteristics or without those characteristics. Statistical significance was defined as a p value less than 0.05. SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
Results
During the study period, total 1616 EMS-treated OHCA patients with presumed cardiac etiology were enrolled in the database. We excluded patients aged under 15 years, resuscitation not attempted at EDs, a transfer from another hospital, not measured albumin, and unknown outcomes (Figure 1). Table 1 shows the patient characteristics based on the serum albumin level. Significant differences were found in patient demographics, prehospital, and hospital emergency treatment based on serum albumin level. The serum albumin ⩾ 3.5 g/dL group showed better neurological outcomes than the serum albumin < 3.5 g/dL group: 18.5% versus 4.0%, and ⩾ 3.5 g/dL group had higher survival discharge rates than the < 3.5 g/dL group: 23.9% versus 9.1% (p < 0.01).
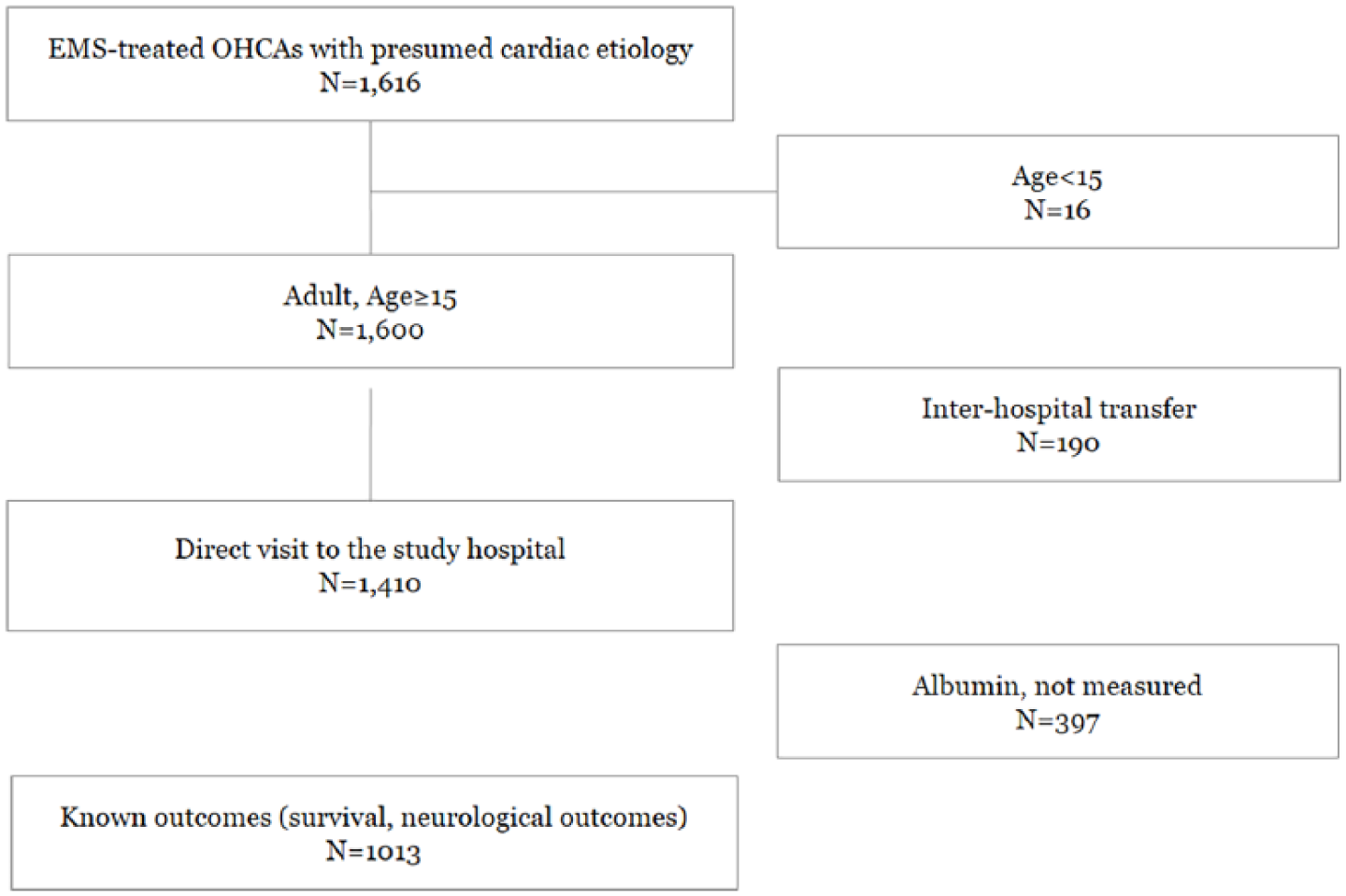
Patient enrollment flow.
Demographics and outcomes of the study population by serum albumin level.
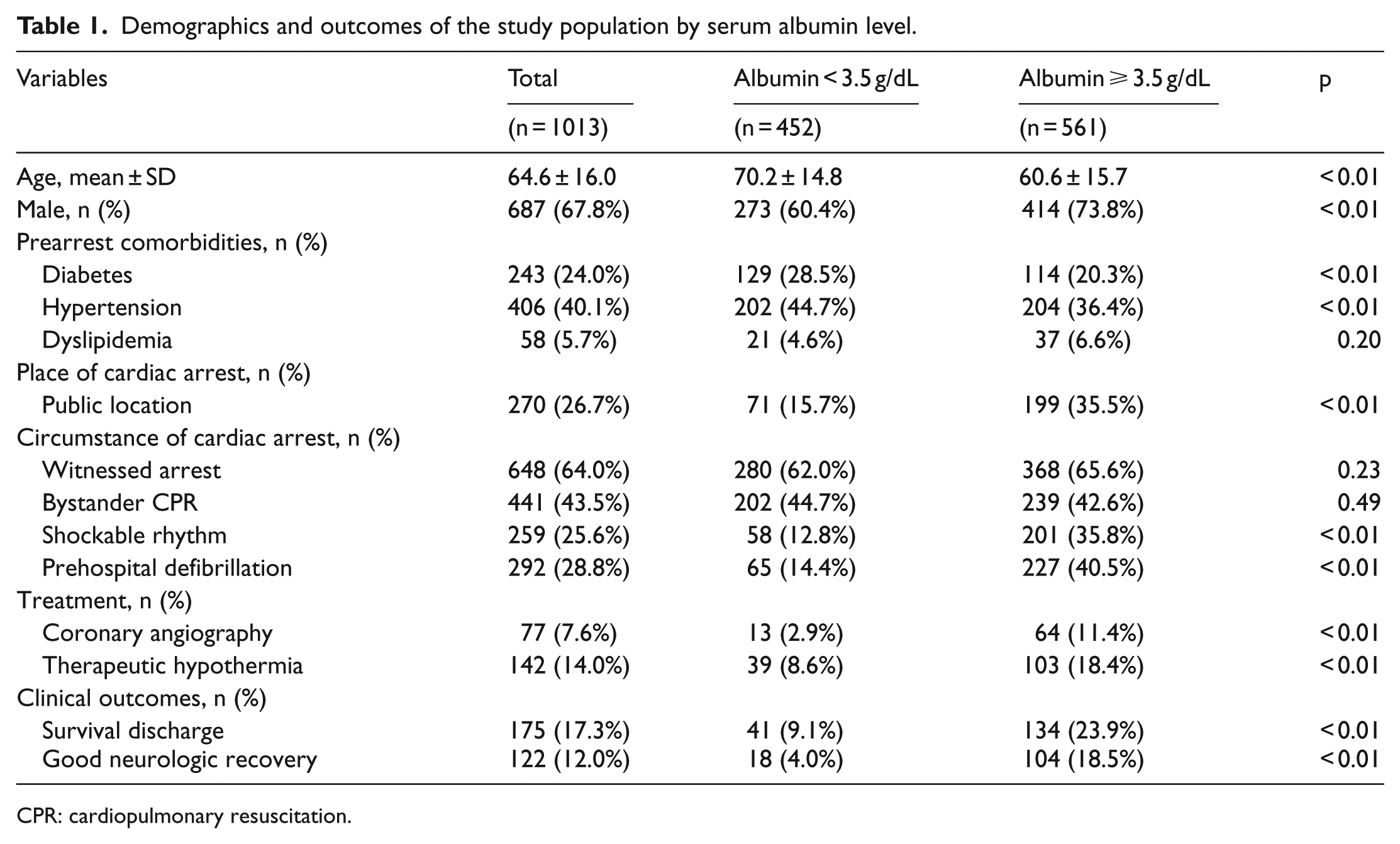
CPR: cardiopulmonary resuscitation.
Tables 2 and 3 show the patient characteristics by survival discharge outcomes and neurological outcomes, respectively. After adjusting for potential covariates, patients with serum albumin ⩾ 3.5 g/dL had a higher odds of good neurological recovery (AOR: 2.94 (95% CI: [1.57, 5.49]; Table 4)) and higher survival to discharge (AOR: 1.74 (95% CI: [1.10, 2.76]); Table 4). Table 5 shows the effects of serum albumin level on good neurological recovery in the interaction model with demographic characteristics. The measure of interaction on the multiplicative scale in this model was not statistically significant (all p > 0.05).
Demographics of the study population by survival discharge outcomes.
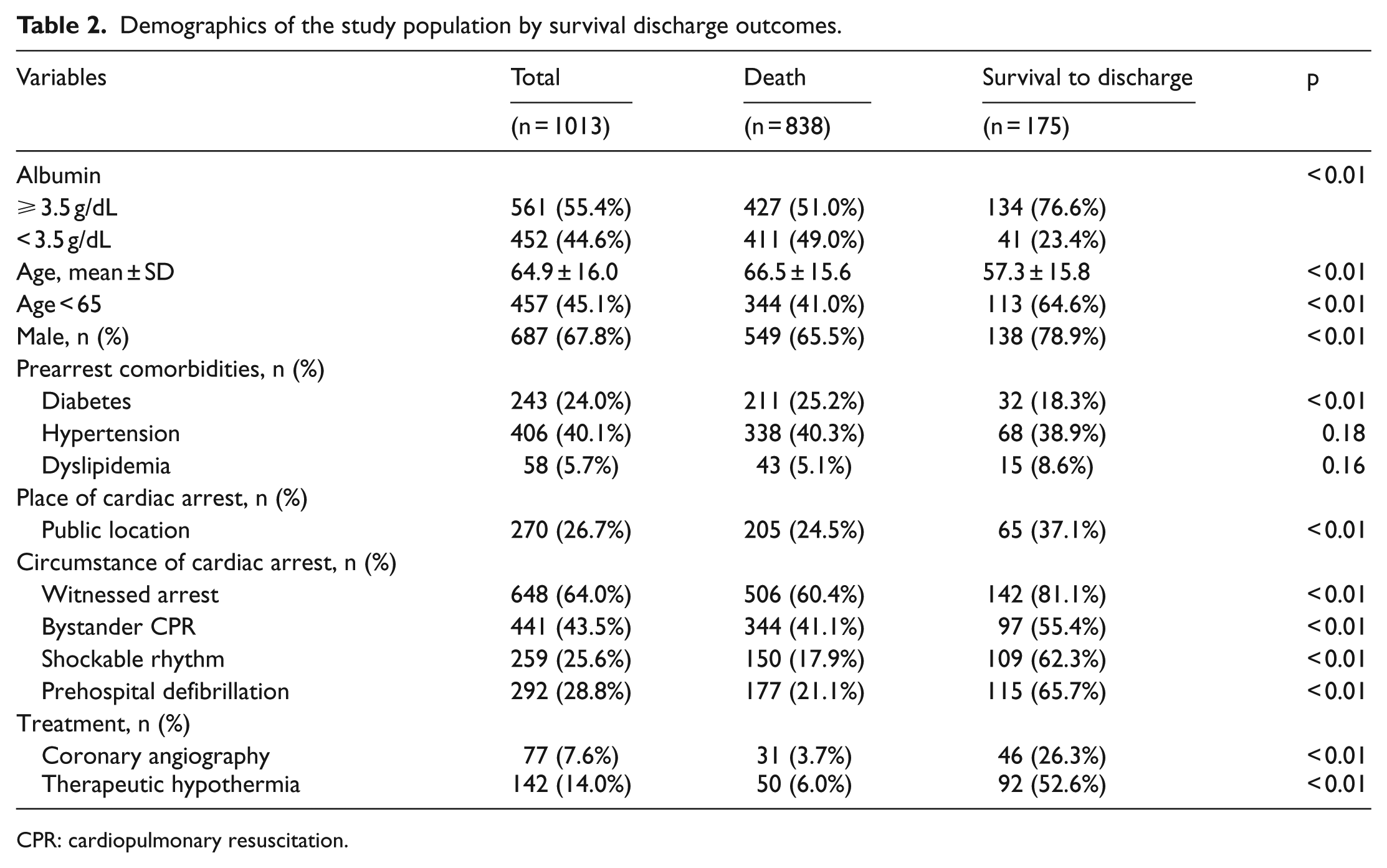
CPR: cardiopulmonary resuscitation.
Demographics of the study population by neurological outcomes.
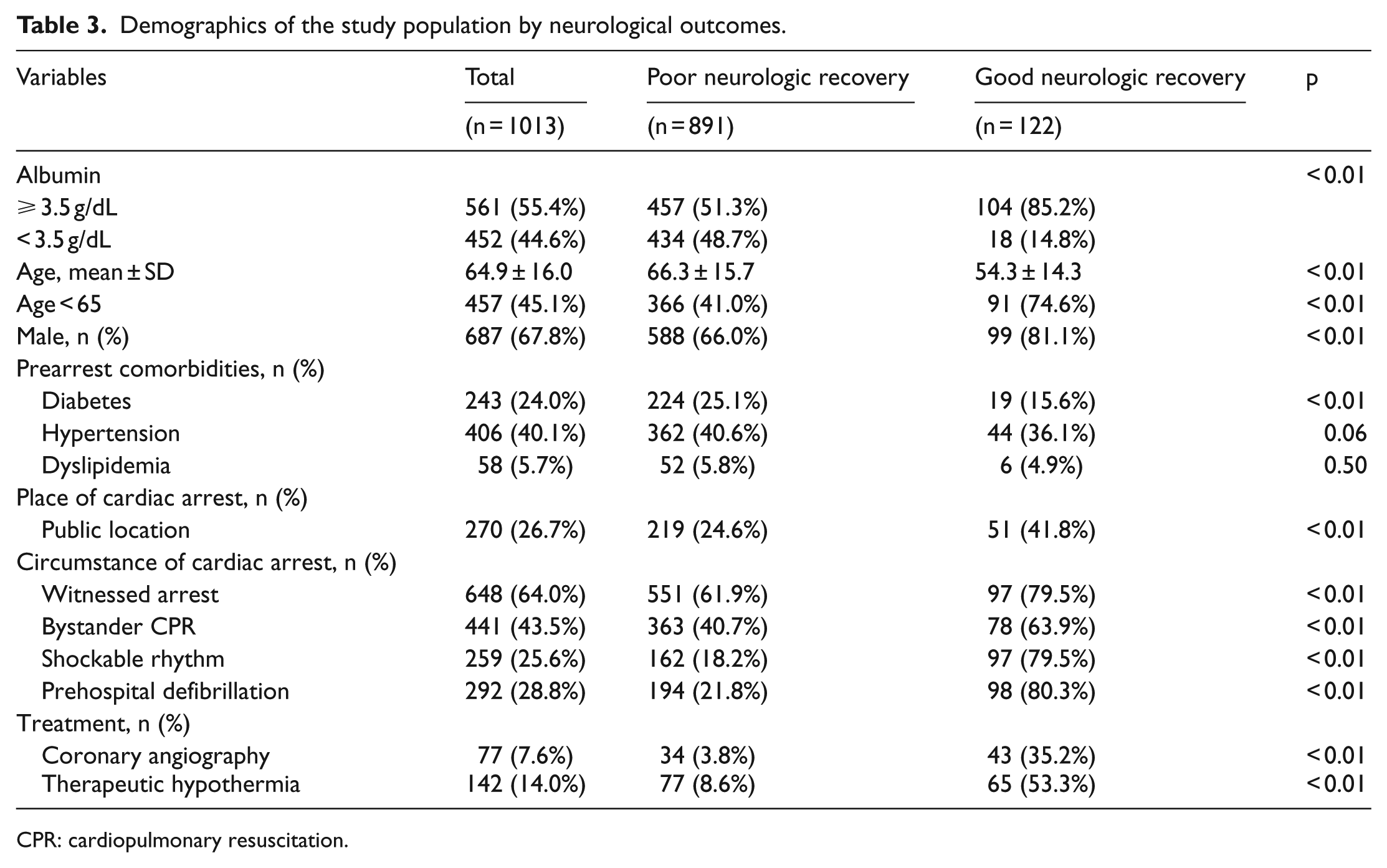
CPR: cardiopulmonary resuscitation.
Effect of serum albumin level on survival discharge and good neurological recovery.
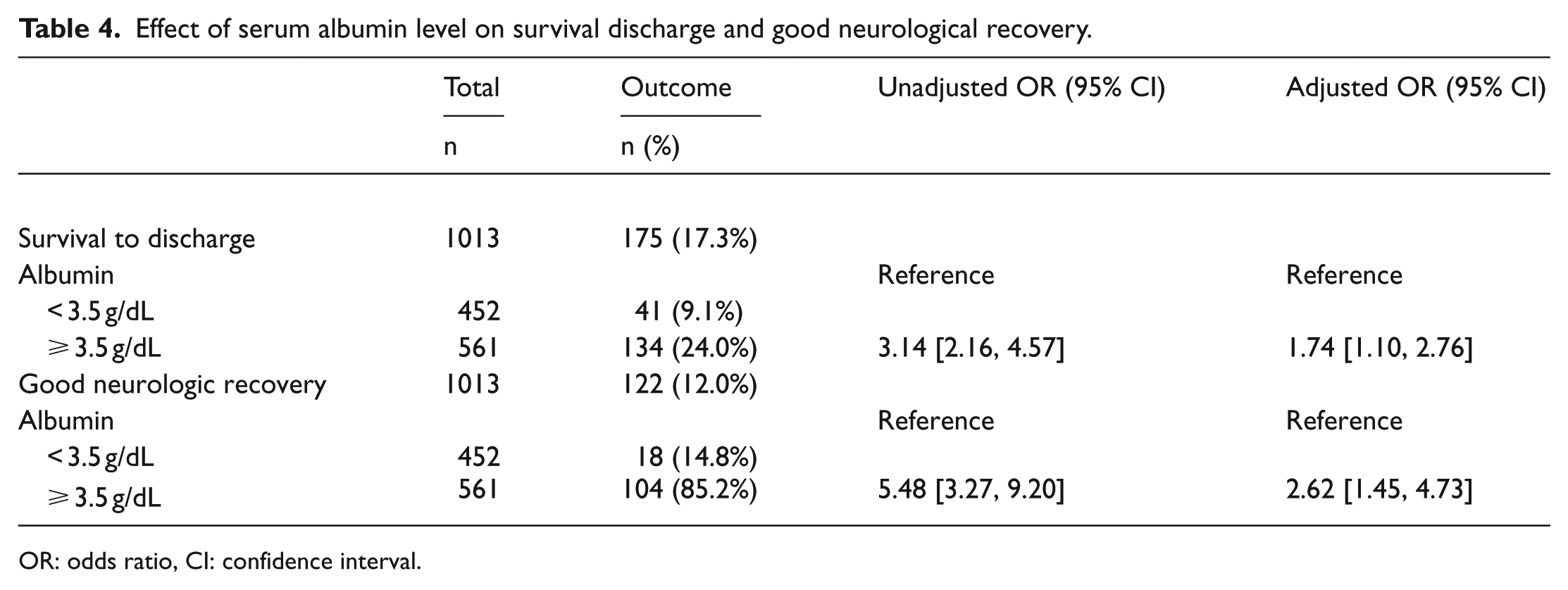
OR: odds ratio, CI: confidence interval.
Effects of serum albumin level on good neurological recovery in interaction model with demographic characteristics.
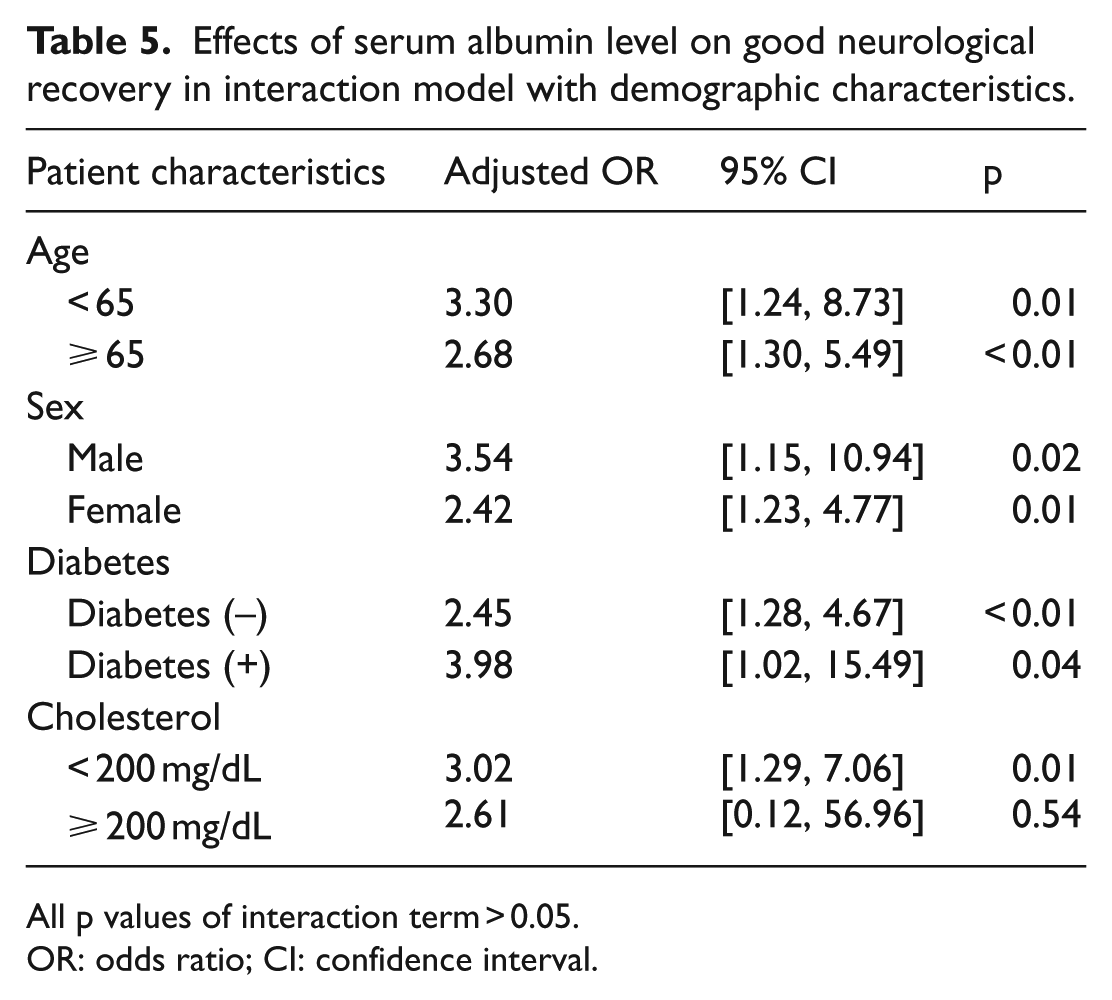
All p values of interaction term > 0.05.
OR: odds ratio; CI: confidence interval.
Discussion
This prospective cohort study conducted in multiple hospitals throughout Korea found that serum albumin level is associated with outcome of the neurological recovery of EMS-treated OHCA patients with presumed cardiac origin. Patients with serum albumin level under 3.5 g/dL resulted in the less favorable neurological outcome and lower survival rate.
Association between hypoalbuminemia and poor outcome in multiple diseases is well known. Serum albumin level is a proven prognostic factor in patients with cancer, infection, liver disease.15,16 Serum albumin level is affected by both disease’s severity and chronicity. For example, at the acute infectious state, serum albumin is one of the negative acute-phase protein markers. 17 And in chronic diseases such as liver cirrhosis, serum albumin is slowly produced and has a structural change. This together with third space loss causes low effective albumin concentration.18,19
In our study, serum albumin level was obtained right after the patient arrived at the hospital. So, hypoalbuminemia could be a result of the patient’s underlying general condition and comorbidities before the arrest. However, after adjusting possible confounders like age, comorbidity by multivariable analysis, low serum albumin level was independently associated with poor neurologic outcomes.
PCAS pathophysiology was important for understanding the relationship between low serum albumin level and poor outcome of OHCA patients. Patients went through the global ischemic state during the cardiac arrest and soon experienced reperfusion injury when the return of spontaneous circulation (ROSC) occurred.
Inadequate oxygen delivery to the tissue during the arrest makes oxygen debt (the difference between predicted oxygen consumption and actual consumption multiplied by time duration). 20 Oxygen debt causes endothelial activation and systemic inflammation response. This process is mediated by various endotoxins and free radicals. Albumin acts as a scavenger of reactive oxygen radicals through its power to bind and transport toxic substances. 19
During the PCAS, cerebrovascular circulation is very unstable. The cerebral microcirculatory reperfusion failure can cause microvascular occlusion during the arrest. 21 On the other hand, macrocirculation is relatively hyperemic due to the elevated cerebral perfusion pressure and failure of cerebrovascular autoregulation.22,23 Early hemodynamic optimization must be done to improve OHCA patient’s neurologic outcome. Serum albumin is responsible for approximately 60% of plasma colloid oncotic pressure. 19 Hypoalbuminemia can cause hypotension and decrease blood flow to the brain. The PCAS patient has increased vascular permeability due to systematic inflammatory response. 20
Our study has limitations. First, this study is hospital-based study and the hospitals participated were large tertiary hospitals. These hospitals tend to have more chronically ill patients, which can be a possible bias. However, we registered all patients with OHCA treated by EMS and followed by transportation to the participating hospitals, the selection bias was small. Second, we failed to record patients underlying nutrition status and performance level before the arrest. A chronic ill condition such as cancer patients or chronic bedridden state can cause hypoalbuminemia. Third, this study did not adjust the effects of other biomarkers. For example, serum total protein level or cholesterol level can be a surrogate marker for patient’s nutrition status. There is a possibility of missing the hidden confounders. Fourth, there is only limited information about postresuscitation management such as how the patient was nutritionally supported or whether albumin was replaced. Further, there was no information about serum albumin level during hospitalization.
Conclusion
Low serum albumin level is associated with poor neurologic outcome in OHCA patients with presumed cardiac etiology. Measuring serum albumin level in the early course of management and integrating it to the prognostication tools for OHCA patients could improve the validity and reliability of the prediction. Identifying patients with low chance for recovery might help physicians allocate resources for postcardiac care and reduce meaningless treatment for OHCA patients.
Footnotes
Acknowledgements
We thank emergency medical technicians working in Korea.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Korean Centers for Disease Control and Prevention (KCDC) and National Fire Agency (Funding number: 2014-E33001-00).
Availability of data and materials
The data of this study are available and can be reanalyzed by authors.
Ethical approval
Research ethics board approval was obtained for this research (IRB number: H-1401-090-550).
Informed consent
Informed consent was obtained from the patient or patient’s family.