
Abstract
Neck pain is a common complaint in the emergency department. It is often attributed to sprain and strain, and cervical spine degeneration. However, when the pain is prolonged, refractory to treatment and not improved after multiple consultations, an alternate diagnosis should be considered.
Keywords
A lady in her 70s who is a smoker with hyperlipidaemia and suboptimal diabetic control complained of increasing neck pain for 5 months. The pain was insidious in onset, sharp in character and persistent in nature. It was worse when she moved her neck. There were no radiation, history of trauma, fever, limb numbness or weakness. She visited numerous doctors including a specialist in orthopaedics. Despite tramadol and physiotherapy, her neck pain showed no improvement. Other than the obvious distress, physical examination showed a stiff neck and bilateral paraspinal muscle tenderness. There were no spinal tenderness and cervical myelopathic hand signs. Upper and lower limbs examination revealed full strength, normal tones, normal deep tendon reflexes, and intact fine touch and pinprick sensation symmetrically. Range of movement of neck was full. A X-ray of her cervical spine was taken (Figure 1).
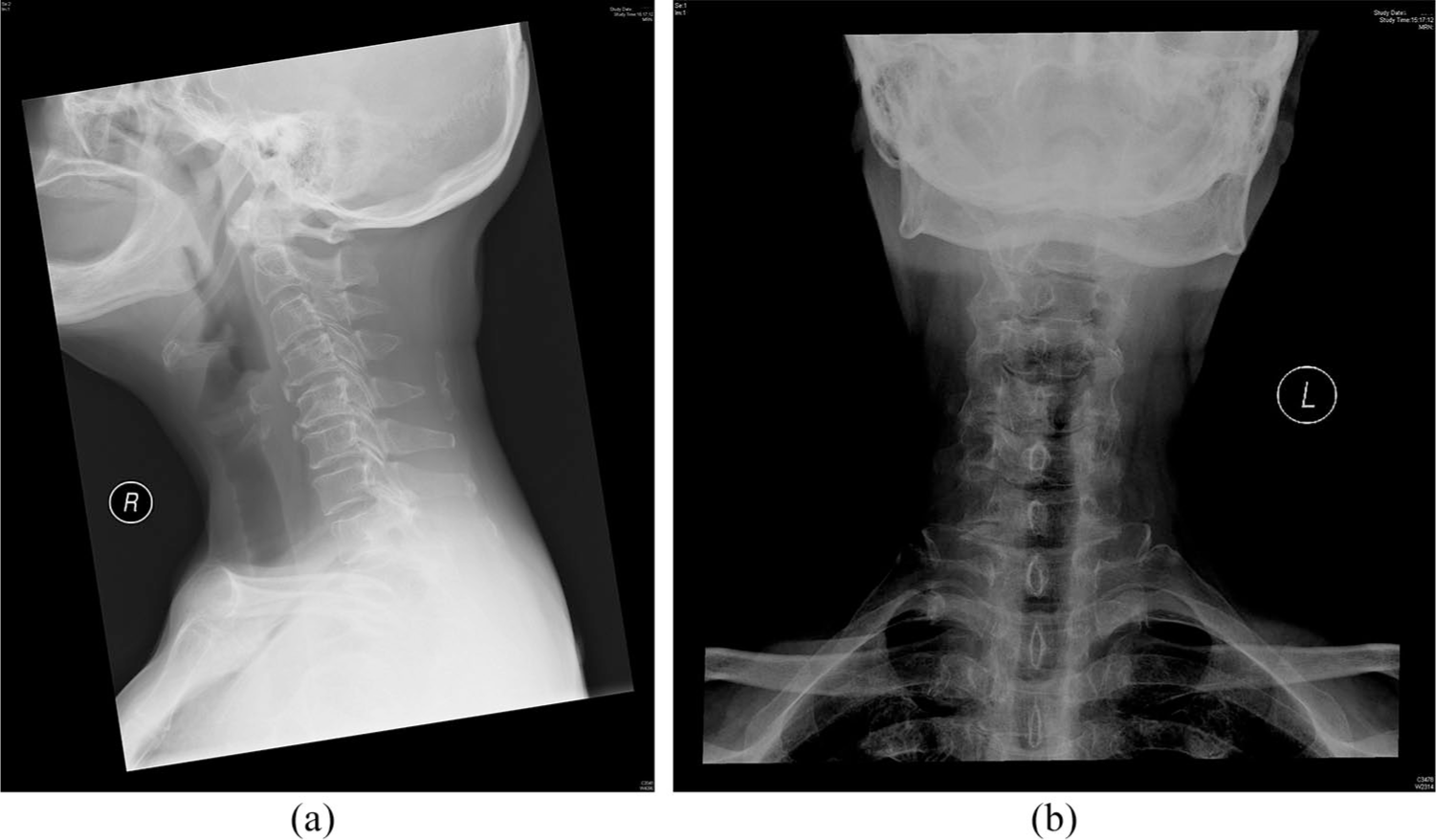
X-ray of her cervical spine: (a) lateral view and (b) anteroposterior view.
Questions
Other than the degenerative changes of the cervical spine, what is the most striking finding?
Name the condition.
What are some of its presentations?
Answers
There is an elongated ossified stylohyoid ligament on the right, which measures 8.8 cm and angulates anteromedially.
Eagle’s syndrome.
Two variants were described by Eagle. 1 The classic styloid syndrome often presents with sore throat, odynophagia, globus sensation, dysphagia and hoarseness secondary to irritation of cranial nerves V, VII, IX and X by the elongated process. However, the stylo-carotid syndrome is related to the irritation of carotid arteries and its perivascular carotid nerve plexus which results in neck pain on rotation in the carotid territory. Most importantly in emergency setting, it can result in dissection of the carotid arteries leading to cerebrovascular symptoms. 2
Discussion
Eagle’s syndrome also termed as ‘stylohyoid syndrome’ encompasses a collection of symptoms resulting from irritation of structures coursing through the parapharyngeal space (mentioned above) by the abnormal elongation and/or anterior angulation 1 of the styloid process. The prevalence of adults with an elongated styloid process ranges from 4% to 7.3% depending on the upper limit of its normal length, but not everyone is symptomatic. 3 Nevertheless, it is elongated if it exceeds 3 cm, which is measured between its base and apex along the posterior aspect.
The cause of elongation is not well understood, which can be idiopathic, congenital (persistence of cartilaginous precursors) and acquired (osseous tissue proliferation due to trauma). 1 There are multiple pathophysiological mechanisms. Commonly, contracture of post-tonsillectomy scar tissue can lead to a narrow parapharyngeal space which results in impingement of various structures. However, granulation tissue proliferation resulting from avulsion fractures (often remote from presentation) caused by coughing, seizures and sudden laughter can bring irritation. On its own, the inflammation from degenerative changes of the tendinous stylohyoid insertion can cause pain.
Clinically, symptoms may be reproduced by digitally palpating the styloid process intraorally around the tonsillar fossa. Relief of symptoms by injecting local anaesthetic into the tonsillar fossa establishes the diagnosis. Computed tomography (CT) scan of the neck not only can discern the anatomic relationships and help with surgical planning, it can also rule out other differential diagnosis of glossopharyngeal neuralgia. Indeed, CT angiography is the gold standard for the stylo-carotid variant. 3
Finally, Eagle’s syndrome should be managed surgically given the possibility of cerebrovascular events. Analgesics, steroid injections, antidepressants or anticonvulsants such as gabapentin 4 can be tried as a bridge to surgery. Long-lasting relief of symptoms requires the surgical removal or shortening of the elongated process by otorhinolaryngologist which is performed intraorally or extraorally.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was not necessary because no patient data have been included in the manuscript.