
Abstract
Introduction:
Subarachnoid hemorrhage (SAH) is a critical disease, and people may get mortality on SAH. Another severe disease induced cardiac arrest is acute coronary syndrome (ACS), and our two cases share the typical characteristics of ACS electrocardiogram (ECG) with ST-segment elevation. The experience is rare and educable, so we present this article to remind emergency physicians in similar cases.
Case presentation:
Two post-resuscitation electrocardiogram (ECG)-proven cases of out-of-hospital cardiac arrest (OHCA) revealed ST-segment elevation.
Discussion:
However, the etiology of the arrest was proven to be subarachnoid hemorrhage (SAH) in the Emergency Department. In this article, we shared ECGs and brain CT scans as a reminder to ED doctors to bear in mind other differential diagnoses when ECGs show ST-segment elevation post-resuscitation.
Conclusion:
Cases such as these alert frontline ED physicians to the possibility of SAH in cardiac arrest patients and the potentially lethal consequence of inappropriate treatment.
Keywords
Introduction
Acute coronary syndrome (ACS) is the main cause of out-of-hospital cardiac arrest (OHCA). Advanced cardiac life support (ACLS) guidelines recommend immediate coronary reperfusion therapy for return of spontaneous circulation (ROSC) following ACS-related OHCA. Twelve-lead electrocardiograms (ECGs) performed immediately after ROSC play a role in initiating coronary reperfusion therapy in the Emergency Department (ED). On the contrary, subarachnoid hemorrhage (SAH) is known as one of the etiologies of OHCA, accounting for 3%–11% of cases.1,2 SAH-related cardiac manifestations have been reported3,4 and diverse ECG presentations of SAH have been observed, but ST-segment elevation has rarely been reported. Treatment required for SAH is totally different to that needed in cases of ACS, and therefore, in patients such as these, clinicians must ensure that they make the correct diagnosis.
Case 1
A middle-aged person, without any cardiovascular risk factors or pre-medication, was brought to our ED by ambulance due to sudden OHCA. According to family members, the patient did not complain of any discomfort before collapsing. The patient experienced sudden onset of loss of consciousness after sneezing.
The Emergency Medical Service (EMS) provider responded within 7 min; they performed cardiopulmonary resuscitation (CPR) and arrived at the ED about 20 min after the patient had collapsed. Neither pulse nor responses were detected from the patient upon arrival at the ED. An automated external defibrillator did not perform an electric shock. In the ED, CPR was performed according to the 2015 Advanced Cardiac Life Support Guidelines. After ROSC, the patient’s vitals were as follows: blood pressure—134/71 mmHg, pulse rate—144/min, and Glasgow Coma Scale score—E1M1V1. Both pupils were dilated without light or corneal reflexes. A 12-lead ECG after ROSC showed atrial flutter and ST-segment elevation in leads II, III, and aVF without reciprocal change (Figure 1(a)).
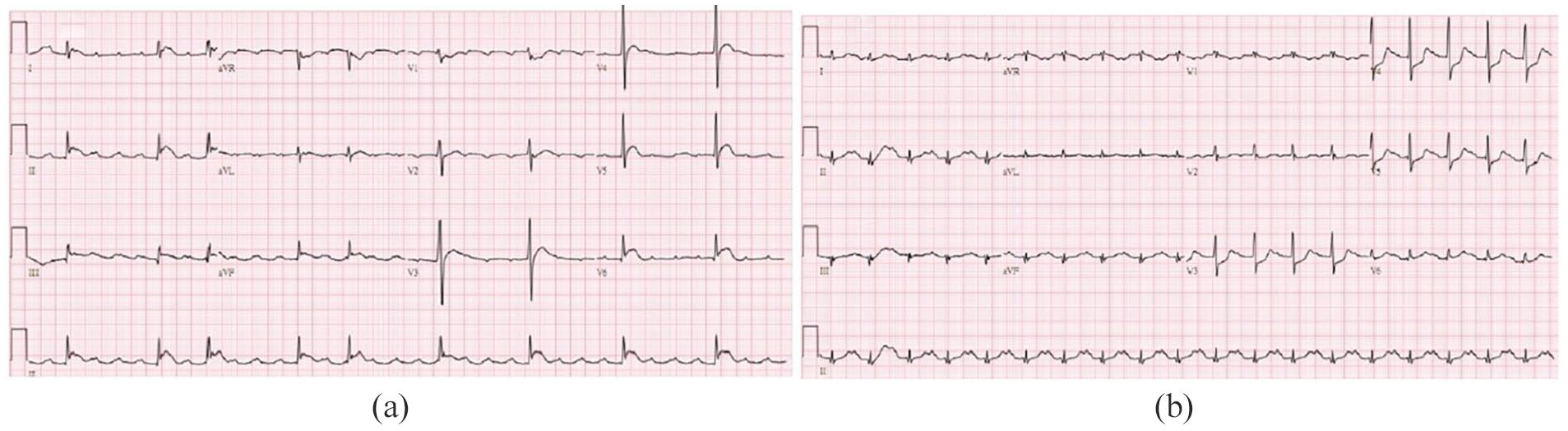
ECG: (a) the initial ECG after ROSC, showing atrial flutter and ST-segment elevation in leads II, III, and aVF without reciprocal change and (b) the second ECG (performed 10 min after ROSC), showing sinus tachycardia, ST-segment depression over V3–V5, and resolution of ST-segment elevation over II, III, and aVF.
The results of serum tests were as follows: sodium—146 mmol/L, potassium—3.1 mmol/L, glucose—359 mg/dL, troponin-I—0.36 μg/L, lactate—19.2 mmol/L, pH—6.71, pCO2—144.6, and HCO—318 mmol/L. After 10 min, a repeat ECG showed sinus tachycardia, ST-segment depression over V3–V5, and resolution of ST-segment elevation over II, III, and aVF (Figure 1(b)). Due to sudden onset of consciousness change, an abnormal neurological examination, and serial ECG change after ROSC, a cerebral computed tomography (CT) scan was performed, which revealed profound SAH (Figure 3(a)). A neurological surgeon was consulted immediately; however, the patient expired 4 h later.
Case 2
A middle-aged patient with hypertension was brought to our ED by the EMS due to sudden-onset neck pain and chest pain with radiation to the back. The EMS responded quickly and was with the patient within 5 min; however, on the way to our hospital, the patient’s consciousness deteriorated, and 5 min after arriving at the ED, neither pulse nor breathing was detected. ACLS was performed and it was not shockable rhythm; after 4 min of ACLS, ROSC was noted.
The first 12-lead ECG after ROSC showed supraventricular tachycardia with V2 and V3 ST-segment elevation without reciprocal change (Figure 2(a)). After ROSC, the patient’s vitals were as follows: blood pressure—142/80 mmHg, pulse rate—130/min, and Glasgow Coma Scale score—3. Neither light nor corneal reflex of the bilateral pupils was noted. The results of serum tests revealed the following: sodium—138 mmol/L, potassium—3.4 mmol/L, glucose—325 mg/dL, troponin-I—less than 0.01 μg/L, lactate—5.4 mmol/L, pH—7.14, pCO2—62 mmHg, and HCO3—21 mmol/L. After 7 min, the ECG was repeated and showed supraventricular tachycardia with ST-segment depression over V2, V3, and V4 and resolution of ST-segment elevation (Figure 2(b)). CT of the brain and chest was performed under suspicion of aortic dissection and subsequent stroke. Unexpectedly, chest CT revealed no evidence of aortic dissection, but brain CT showed diffuse SAH and brain edema (Figure 3(b)). Emergency ventricular drainage was performed, and digital subtraction angiography showed one ruptured saccular aneurysm over the basilar artery, for which the patient was treated with stent-assisted coiling. Unfortunately, the patient expired 10 days later.
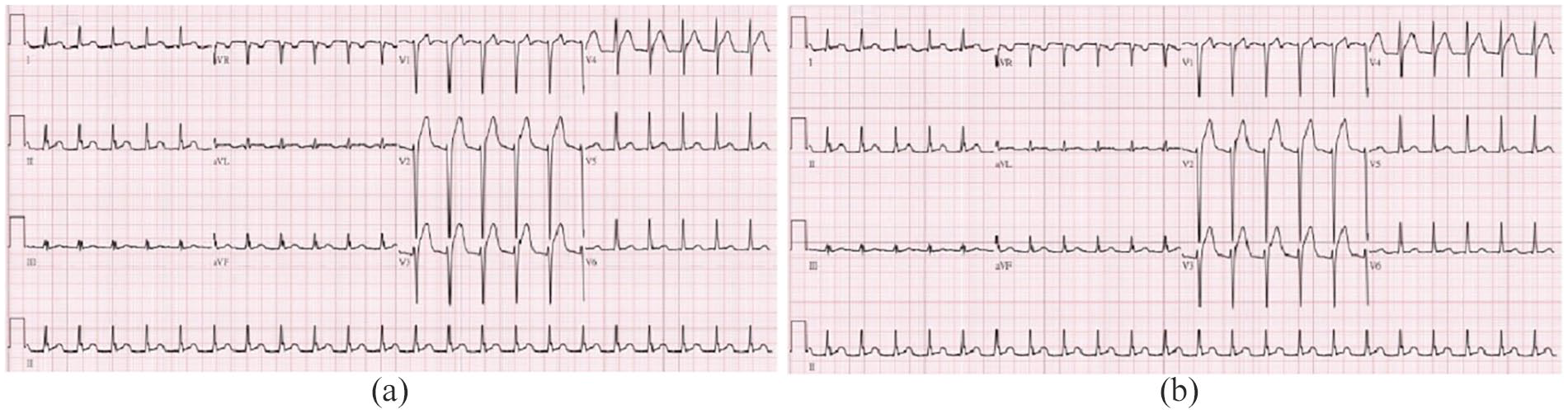
ECG: (a) the initial ECG post-ROSC, showing supraventricular tachycardia with V2 and V3 ST-segment elevation and (b) the second ECG (performed 7 min after ROSC), showing supraventricular tachycardia with ST-segment depression over V2, V3, and V4 and resolution of ST-segment elevation.
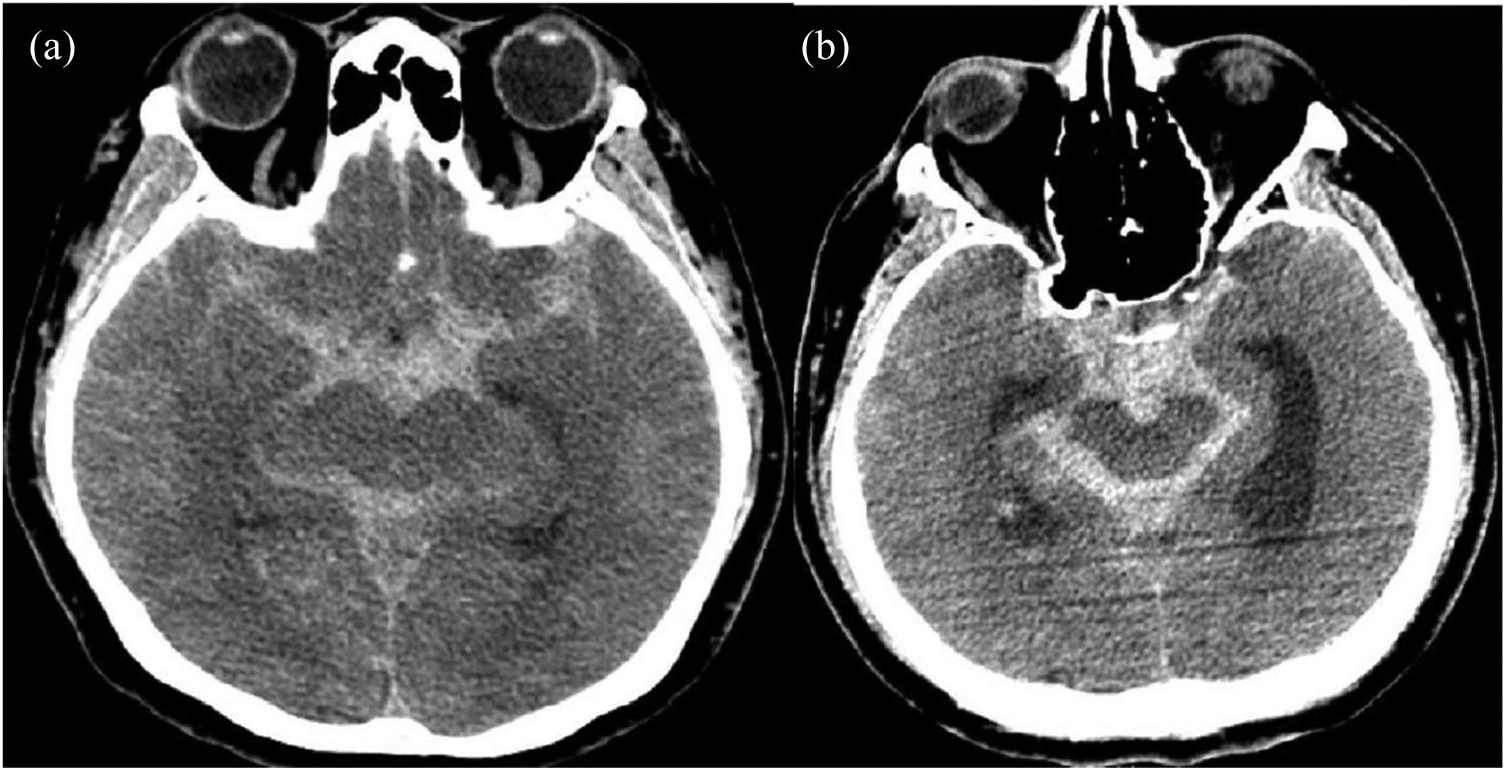
Brain CT scans showing SAH: (a) case 1 and (b) case 2.
Discussion
SAH-related cardiac manifestations inducing ECG and serum cardiac enzyme troponin abnormalities have been reported previously. ECG changes are observed in 44.8% of patients with SAH, including T-wave inversion, ST-segment depression, prolonged QT, and large U and high R waves.5,6 However, SAH-related ST-segment elevation has rarely been reported. Neurogenic cardiac injuries due to catecholamine effects, systemic circulatory effects, neurogenic stunned myocardium (NSM) syndrome, and neuroinflammation have been proposed. 7
NSM syndrome illustrates that myocardial injury is induced by a catecholamine surge after a sudden onset of acute brain injury, which is a result of an imbalance in the autonomic nervous system.3,8,9 Catecholamine surge leads to coronary vasospasm and subsequent ischemia via an increase in myocardial demand and direct toxic effects on the myocardium, resulting in mitochondrial dysfunction and cell death. NSM syndrome presents predominantly as myofibrillar degeneration or myocytolysis and is distinct from myocardial necrosis. 10 The occurrence of NSM syndrome may increase the risk of life-threatening events, and treatment should generally focus on the underlying neurologic disorder. Fortunately, NSM syndrome is a totally reversible disorder if the patient is resuscitated successfully. Therefore, if we can differentiate the ECG patterns of SAH-induced change from real myocardial infarction producing, and treat the specific disease, the patient would obtain the most benefit.
ECG changes occur most commonly in the first few days after injury and are often transient, because repolarization normalizes as the neurological insult resolves. Yamashina et al. 11 reported that the female gender, a preserved left ventricle ejection fraction (>50%) according to ECG, and ST-segment elevation without reciprocal change favor SAH-related ST-segment elevation over ACS. ST-segment elevation over leads II, III, and aVF, and over V2 and V3, respectively, was observed in our two patients (one male and one female). No reciprocal ST-segment depression was observed, and the ST-segment elevation resolved 7–10 min later.
It remains a challenge for ED physicians to distinguish SAH from ACS in post-resuscitation cases. When a post-resuscitation ECG shows ST-segment elevation, we are possibly prone to misdiagnose this as acute myocardial infarction (AMI) and treat immediately with antiplatelet and anticoagulant agents, and may even consult a cardiovascular specialist for percutaneous coronary intervention. This misdiagnosis not only delays a proper diagnosis, but may also have lethal consequences in SAH patients. Cases such as these alert frontline ED physicians to the possibility of SAH in cardiac arrest cases and the potentially lethal consequence of inappropriate treatment.
Although it is difficult to distinguish SAH from ST-elevation myocardial infarction (STEMI) using ECGs, identification of a reciprocal change in ST-segment elevation may be a subtle hint, as was the case in our patients. Further research to clarify the ECG differences between SAH and STEMI is needed. In our cases, serial ECGs provided further information that assisted in distinguishing SAH from STEMI. Potentially, acquiring more information regarding SAH-induced OHCA from the patient’s family and EMS may improve the accuracy of diagnosis. Parameters such as the female gender, a young age, and lack of comorbidities, headache or neurological signs prior to cardiac arrest, plus asystole or pulseless electrical activity as the initial rhythm, are common characteristics among SAH-induced OHCA patients. 1 In recent years, sonograms have played an important role in diagnosis in patients such as these, and the diameter of the optic nerve sheath may also imply a diagnosis of SAH. 12 In this report, we presented two cases of SAH-induced OHCA with ST-segment elevation on ECG. By sharing these two cases, we urge clinicians to consider SAH as a cause of cardiac arrest. On suspicion of SAH, immediate brain CT is required, even if ST-segment elevation is present.
Footnotes
Acknowledgements
Thanks to the great work of EMT, they completed pre-hospital resuscitation, so that we can successfully rescue the patients and share these cases here.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The authors have tried but failed to obtain consent, because when the data were collected, the patient’s personal information was not reserved, so the authors did not know the patient’s identity. We can be sure that the specific patient information will not be disclosed in this article, and no one will be recognized.