
Abstract
Background:
Similar to many Asian cities, there is no statutory provision for the determination of the duty borne by bystander first aiders when assisting victims in Hong Kong.
Objectives:
The aim of this study was to explore the views of a Good Samaritan Law by first-aid learners in Hong Kong.
Methods:
A cross-sectional survey was conducted among first-aid course participants from the two largest training providers in Hong Kong using a self-administered questionnaire.
Results:
In total, 1223 questionnaires were completed and returned. Only 12.1% (147/1211) of participants have ever heard of Good Samaritan Law. After a short description of Good Samaritan Law was provided, 71.4% (848/1188) agreed or strongly agreed on a Likert-type scale that a Good Samaritan Law is necessary; 95.2% (1148/1223) support the enactment of a Good Samaritan Law in Hong Kong.
Conclusion:
The majority of first-aid learners in Hong Kong supported the enactment of Good Samaritan Law. Overcoming the fear of litigation and improving bystander cardiopulmonary resuscitation rate is a priority for improving survival rates from sudden cardiac arrest in Hong Kong.
Introduction
Fear of litigation is one of the important factors affecting the willingness to attempt bystander cardiopulmonary resuscitation (CPR), and this has been found in local and international studies.1–4 In an attempt to overcome this fear and barrier to promoting bystander CPR, Good Samaritan Laws (GSLs) have been enacted in Australia, United States/Canada and various European countries, 5 and more recently in China. 6 Currently in Hong Kong, there is no statutory provision determining the duty borne by bystander first aiders when assisting victims. First aiders may be held liable, for example, being sued or prosecuted for unintentional injury or wrongful death, if they fail to meet the legal responsibilities to their casualties, although no legal action has ever been initiated against a rescuer in Hong Kong. 7
Across Asia, the reported rate of survival to hospital discharge for out-of-hospital cardiac arrest (OHCA) was from 0.5% to 8.5%. 8 The survival rate for Hong Kong in previous studies ranged from 0.5% to 6.7%, with rate of bystander CPR ranging from 13.7% to 28.8%.9–15 The rate of bystander defibrillation using automated external defibrillators (AEDs) was only 1.4% according to a recent study. 9 In a recent 5-year multistate study in United States, overall survival to hospital discharge was 11.4%, with bystander CPR rate of 42.8%. The subgroup with bystander-witnessed OHCA with a shockable rhythm had a survival of 34%. 16
The American Heart Association recognises the importance of early recognition of cardiac arrest, and early defibrillation and CPR are the keys to the chain of survival, and they made the promotion of bystander interventions one of their priorities. 17 Despite the establishment of the Resuscitation Council of Hong Kong and the promotion of bystander CPR among first-aid organisations in Hong Kong, Chair et al. 18 found that 21% of the public reported to have ‘ever received first aid training’ in a survey in 2014. Among those with CPR training, the willingness to perform CPR on family members was 72% versus 42% for strangers in the street. The authors called for the need to ‘enact laws to increase public awareness of CPR and protect bystanders who perform it’. 18
It is essential that opinions from various stakeholders be heard when considering a new piece of legislation. While the views of the general public and the policy makers would be useful, this study focused on the perspectives from the first-aid learners who has acquired the skills for providing bystander CPR. The aim was to understand any barrier the potential rescuer faces and their perceived need for legal protection. Hong Kong currently has no territory wide initiative for first-aid and CPR training, and therefore those who intend to provide bystander CPR are more likely to have enrolled in a standard first-aid course recognised by the government. 19
Methods
We conducted a cross-sectional survey among first-aid course participants from two major training providers in Hong Kong. The standard first-aid courses from Hong Kong St John Ambulance and Hong Kong Red Cross are both first-aid courses recognised by the Hong Kong government, and include CPR training, use of AED, bleeding and shock, wounds and bandaging, trauma and medical emergencies, and so on. Full or refresher course participants during the period of September to December 2017 were invited to complete a self-administered questionnaire. A translated example of the questionnaire is provided in the supplementary material. Ethical approval was obtained from the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong. As the questionnaire was anonymous and the participation was voluntary, the completion and return of the self-administered questionnaire implied consent for the study.
Questionnaire design
The questionnaire has three sections, with a total of 19 questions focusing on aspects of bystander CPR, understanding and attitudes on GSL, and participants’ characteristics. The response to questions on attitudes and beliefs are in the form of a 5-point Likert-type scale. The last question was an open-ended question on ‘other comments regarding the Good Samaritan Law’. The qualitative response was coded and summarised, and direct quotes are provided where appropriate.
Statistical analysis
We used SPSS version 23 (IBM SPSS Statistics for Windows, New York, US) for statistical analyses. Percentages were used to present all categorical data as proportions. The chi-square test was used for comparison of the group who support versus the group who do not support the enactment of GSL in Hong Kong. Binary logistic regression was performed to adjust for the effect of potential confounding variables. P-values of <0.05 were considered significant, and all tests were two-sided.
Results
Out of the 1248 questionnaires distributed, 1223 questionnaires were completed (98% response rate); 66.9% (818) were course participants from Hong Kong St John Ambulance, and 33.1% (405) from Hong Kong Red Cross. Participants’ characteristics are presented in Table 1. The majority were female (54.2%, 651/1202), aged 21–30 (45.3%, 545/1203), with an undergraduate degree (40.9%, 493/1205) and from non-healthcare backgrounds (89%, 1050/1180); they were undertaking a full first-aid certificate course (75.9%, 925/1219) and had never provided CPR in real-life situation before (96.5%, 1174/1217).
Characteristics of all participants and percentage indicated support for Good Samaritan Law enactment.
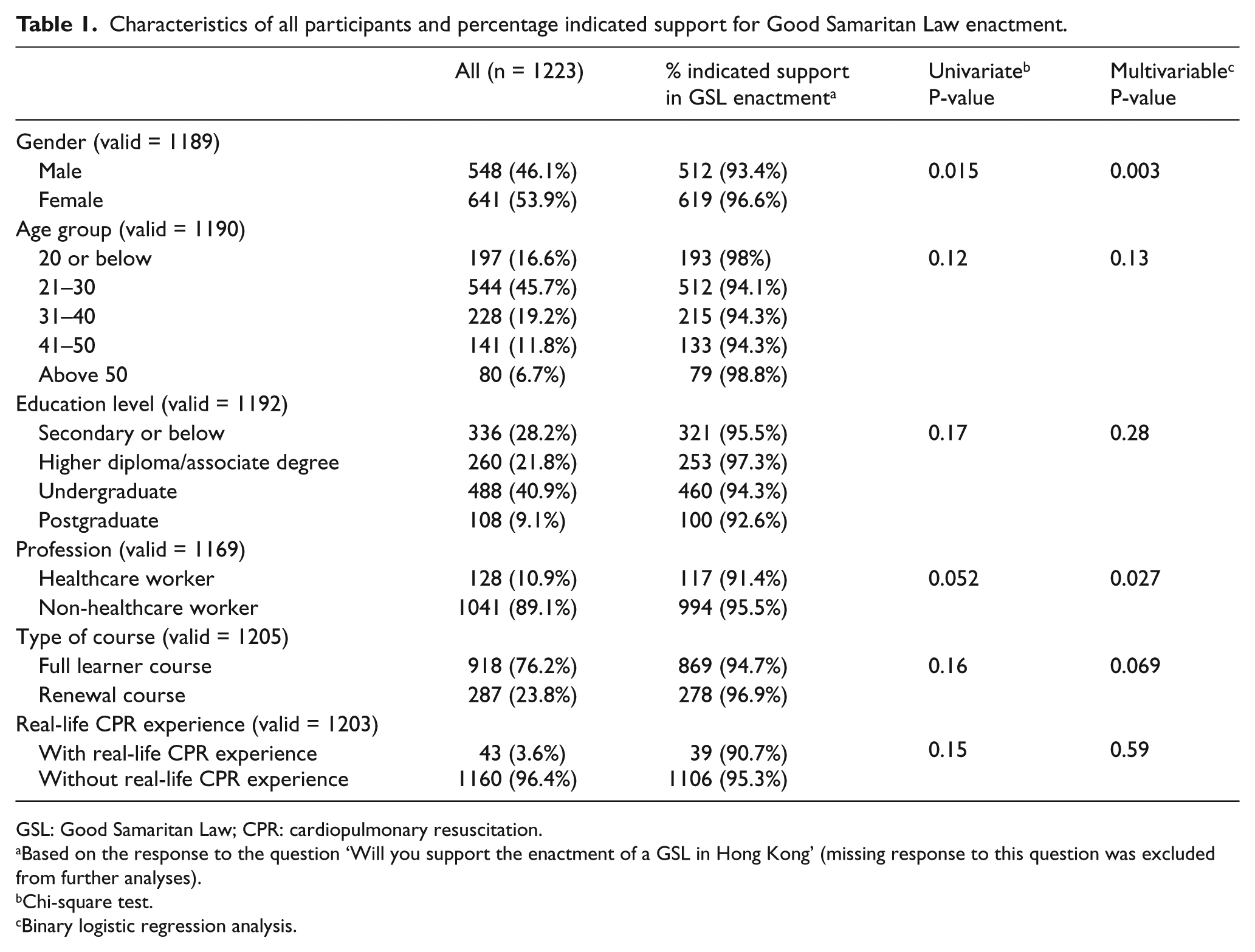
GSL: Good Samaritan Law; CPR: cardiopulmonary resuscitation.
Based on the response to the question ‘Will you support the enactment of a GSL in Hong Kong’ (missing response to this question was excluded from further analyses).
Chi-square test.
Binary logistic regression analysis.
Attitude to providing bystander CPR
The majority of participants agreed that a first aider is morally obliged to respond to an emergency (85%, 1034/1217 scored 4 or 5 (agree or strongly agree) on the Likert-type scale). While in a hypothetical situation of an unknown adult with suspected cardiac arrest requiring bystander CPR, 63.5% (773/1207 scored 4 or 5 on the Likert-type scale) would likely respond by providing bystander CPR. This was followed by the same hypothetical situation but with a child where 61.3% (737/1203 scored 4 or 5 on the Likert-type scale), and an elderly person where 54.7% (660/1206 scored 4 or 5 on the Likert-type scale), would likely respond by providing bystander CPR. When asked to rate their confidence in providing CPR, 59.6% (721/1209) of participants rated they were confident (scored 4 or 5 on the Likert-type scale). Table 2 shows the distribution of the responses.
Attitude of participants to providing bystander cardiopulmonary resuscitation.
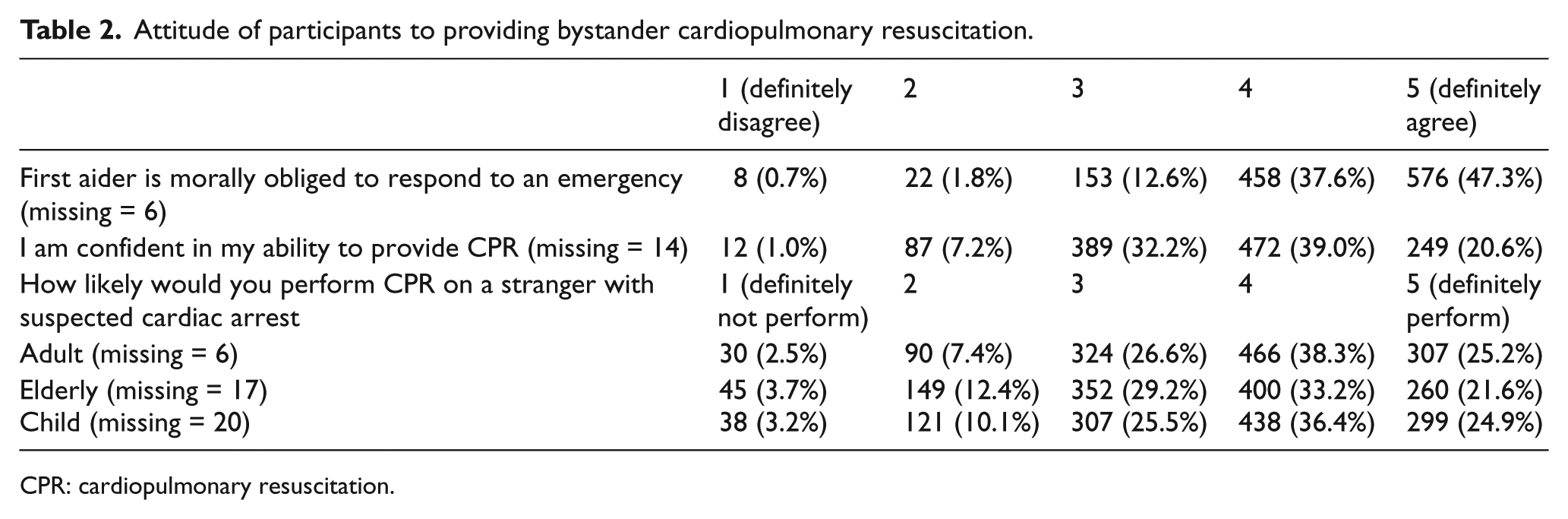
CPR: cardiopulmonary resuscitation.
Understanding of GSL and opinion on GSL enactment in Hong Kong
Only 12.1% (147/1211) of participants have ever heard of the concept of a GSL, and 40.1% think they understand the GSL (57/142 scored 4 or 5 on the Likert-type scale) among those who have heard of it.
A short description (‘GSL offers legal protection to people who give reasonable assistance to those who are in an emergency’) was provided in the questionnaire before subsequent questions on GSL enactment. Figure 1 shows the participants’ response to whether GSL is necessary in Hong Kong, 71.4% (848/1188 scored 4 or 5 on the Likert-type scale) agreed that GSL is necessary; 95.2% (1148/1223) supported the enactment of a GSL in Hong Kong.
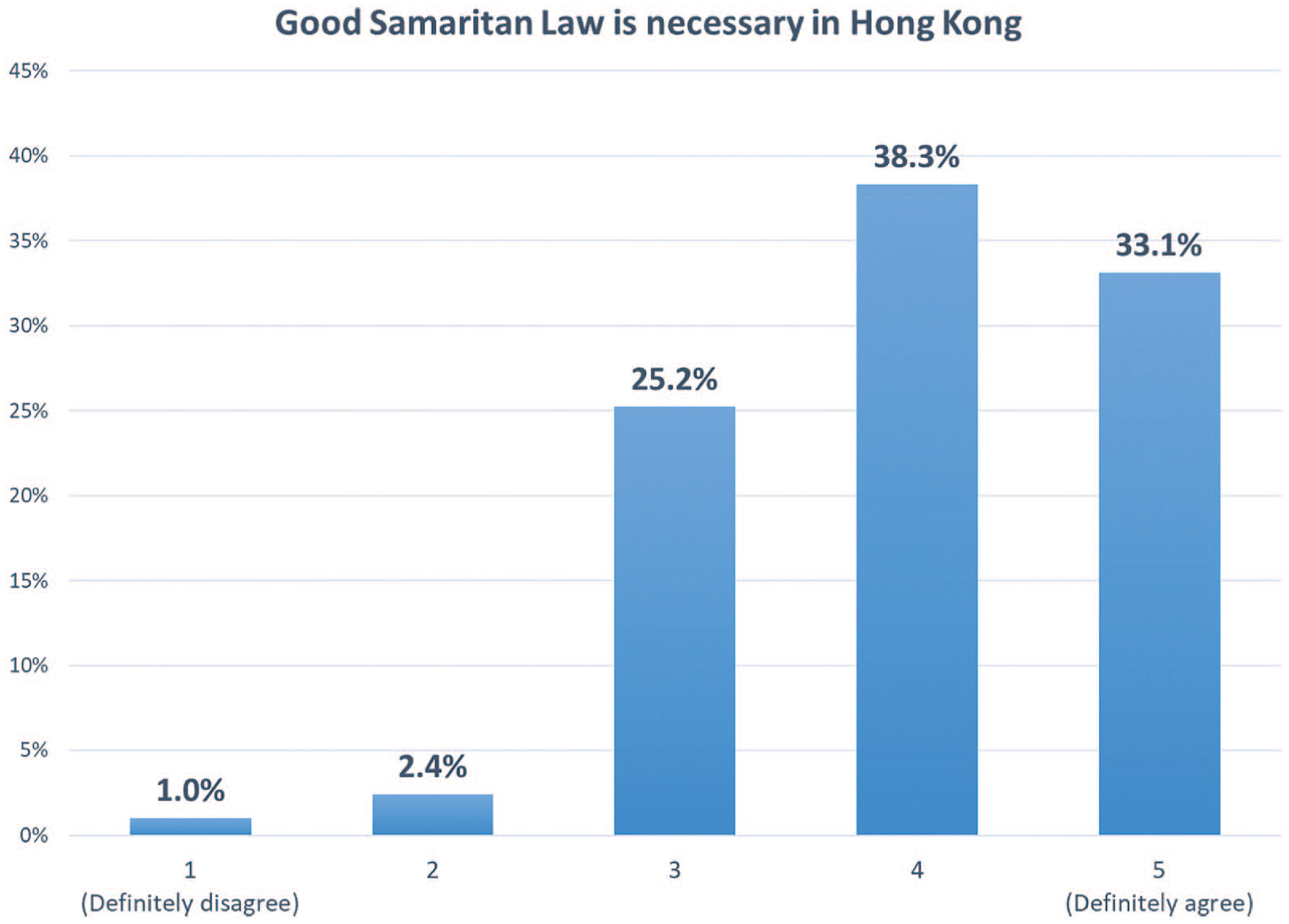
Participants’ response to whether Good Samaritan Law is necessary in Hong Kong.
Female gender and non-healthcare workers were significant factors associated with support for GSL enactment in Hong Kong in the multivariable analysis (Table 1). Among those who support GSL enactment, 57% (643/1129 scored 4 or 5 on the Likert-type scale) said GSL enactment would change their willingness to perform bystander CPR (Figure 2). The number of missing entries are provided in the respective tables.
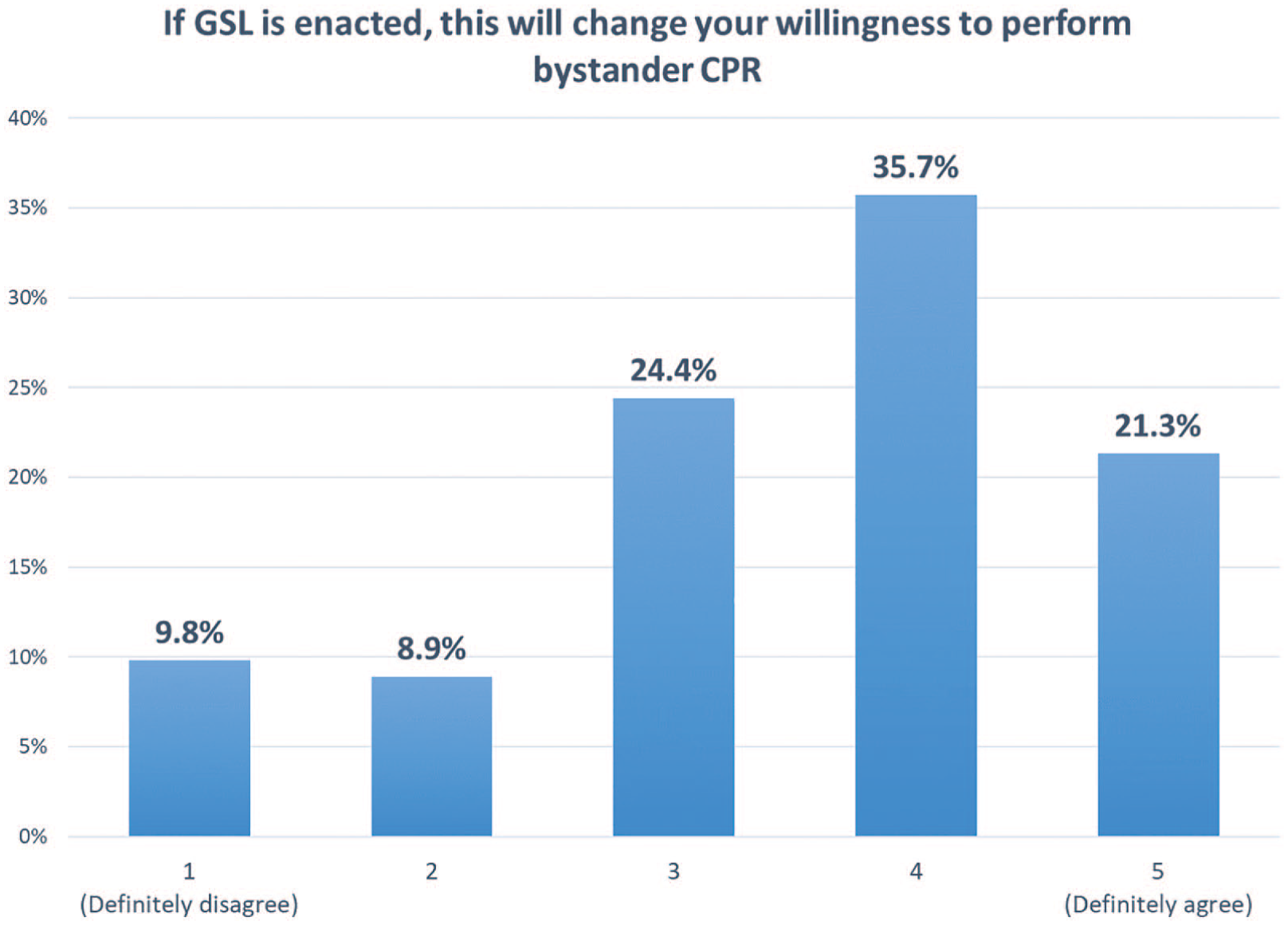
Participants’ response to whether their willingness to perform bystander CPR will change if Good Samaritan Law is enacted (among those who support enactment of GSL, n = 1129).
Reason(s) for not supporting GSL
Among those who do not support GSL, the most common reason was the potential adverse effects of non-standard bystander CPR that they may perform as a volunteer and the potential consequences on the victims (n = 24). The second was that GSL enactment may impinge on existing legislations and lead to legal disputes (n = 18). That the general public in Hong Kong has a weak sense of providing bystander CPR (and therefore GSL would not be effective) was the third most common reason (n = 13). Other reasons include ‘none of my business’ (n = 4) and ‘not familiar with the law’ (n = 3).
Barriers to providing bystander CPR
The lack of ability and confidence in performing CPR was the most frequently cited barrier for bystander CPR (n = 31). Infection risks to the provider (n = 15), pressure of performing CPR in public (n = 9), unwillingness to perform CPR on strangers (n = 9) and the perceived risk of a victim’s family demanding compensation (n = 1) were the other barriers raised.
Qualitative comments regarding GSL
Seventy-three participants provided an optional response to ‘other comments regarding GSL’. Individual comments were coded into three broad categories of ‘in favour of GSL enactment’, ‘against or concerns regarding GSL enactment’ and ‘recommendations regarding GSL’.
The function of the law was stated in comments in favour including ‘the need to protect the bystanders who offer help, so that people in need can receive CPR’ and GSL ‘can promote public bystander CPR awareness and intention’. The lack of GSL was also stated as a factor that ‘contributed to the low survival rate for out of hospital cardiac arrest in Hong Kong’.
An argument raised in those against the law was that first aiders are already adequately protected in the current legal system without GSL. It was also commented that ‘the lack of GSL will not stop me from doing what is right’. On the contrary, the perceived poor public knowledge on CPR was a reason stated, and ‘only the eligible should perform CPR’. It was stated that ‘more harm can be done if CPR performed incorrectly’, and rib fractures in incorrect CPR was also mentioned.
An ethical issue was raised of how to stop people from abusing the law and intentionally doing harm to other people, while protecting those who try to do good and help. It was said to be ‘hard to know people’s intentions’. It was felt that GSL is too difficult to implement, more details of the legal implications of the GSL enactment, how to define ‘reasonable assistance’ and whether GSL can also protect from civil liability and claims for compensation. It was also commented that the name (or the Chinese translation of the name) is misleading.
Suggestions included the need to promote the importance of first aid and CPR at the same time as GSL promotion, and improve the level and standard of CPR performance. It was commented that the government should take the lead in improving the public knowledge, providing a white paper and leading public consultations. The importance of promotion and improved understanding of GSL was mentioned by several individuals, and various channels for promotion included the television, schools, forming interest groups, committees, and putting this topic into the curriculum for liberal studies in secondary schools. A suggestion was also made to provide different levels of first-aid certificates recognised by the government.
Discussion
This is the first GSL survey among first-aid course participants in Hong Kong. We found a low understanding of GSL but a high rate of support for GSL enactment in Hong Kong. Equally importantly, we confirmed that there were real concerns for first-aid course participants in performing bystander CPR in real-life situations. Even though 85% of participants agreed that a first aider is morally obliged to provide aid, only around 55% said that they would attempt CPR on an elderly person with suspected cardiac arrest in the street.
These findings were supported by previous studies that the fear of litigation was higher for CPR performed on strangers (21.6%) versus on family members (13.8%) 3 but differed in terms of rendering assistance to children versus adults. Savastano and Vanni 4 found the fear of litigation to be less for children (4.2%) versus adults (18.1%). While these fears were real, first aiders should be aware that for a victim of sudden cardiac arrest, there is nothing worse than not attempting CPR in these circumstances. Broadening CPR training and providing assurance to increase participation are equally important as improving the quality of the CPR performed. 17
A systematic review published in 2008 reviewed 2409 articles and included 252 papers to understand and improve low bystander CPR rates. 20 Even though the effect of GSL was not specifically mentioned in the paper, the fear of litigation was confirmed to be one of the reasons for not learning CPR. In another paper looking at Good Samaritan behaviours by physicians in North Carolina, it was found that doctors with greater perceived knowledge of the GSL were more likely to have intervened during a recent opportunity. 21 We did not find studies that looked at changes in survival rates before and after GSL enactment, but here we will provide two examples of how GSL legislations have been enacted overseas to tackle low survival rates for OHCAs.
Using the example of an AED programme, evidence has shown that the availability of AED machines alone does not guarantee its use in saving lives. 22 In the United States between 1995 and 2000, all 50 states passed laws and regulations concerning lay rescuer AED programmes. 23 The Cardiac Arrest Survival Act was signed into federal law in 2000. Many states have then re-examined the lay rescuer AED statutes and passed legislation to remove variations and impediments to encourage the development of lay rescuer AED programmes. The AHA recommended the Good Samaritan limited immunity (immunity limited to simple negligence) for rescuers and programme facilitators as one of the four key components in AED legislation. 23
A 2010 documentary review of laws in the 50 states recommended that comprehensive Public Access Defibrillation (PAD) legislation should cover all 13 PAD programme elements. 24 The authors suggested that these critical elements are necessary to sustain and ensure AED functionality or they may be at risk of failure. These elements included (1) Placement, (2) Training, (3) Maintenance and testing, (4) EMS/ medical coordination (further split into four elements), (5) Continuous quality improvement and planning (split into two elements) and (6) Good Samaritan civil immunity (split into four elements). Regarding the Good Samaritan civil immunity, four types of immunity exists for (1) the untrained and trained lay rescuers, (2) AED acquirers including the person or entity providing the AED site placement, (3) programme directors including the licenced physicians and medical authorities and (4) the owner, manager or renter of the premises where the AED is installed. 24 Research has also found that schools demonstrated a significant increase in medical emergency response plans and on campus defibrillators after state legislation had been passed. 25
A more recent example is the Good Samaritan Drug Overdose Act in Canada
26
which provides exemption from possession of substance charges. It is stated that No one who seeks emergency medical or law enforcement assistance because that person, or another person, is suffering from an overdose is to be charged or convicted under subsection 4(1) if the evidence in support of that offence was obtained or discovered as a result of that person having sought assistance or having remained at the scene.
Similar legislations have been passed in the United States in response to the growing problem of deaths from narcotics overdose, including New York 27 and Washington State. 28 , 29
Among drug users in New York, Hansen et al. found that ‘participants fearing criminal penalties delayed calling 911 or abandoned overdose victims after calling 911, risking victim morbidity and fatality’. A survey from Seattle which interviewed 251 police officers and 28 paramedics found that knowledge was low and opinions of the Drug Overdose–Naloxone–Good Samaritan Law were mixed. The authors concluded that even though the exemption from possession of substance charges may have impacted on the law enforcement aspects, police officers from the study were concerned about the issue of opioid overdose and were willing to implement agency-wide training. 29
In a recent study looking at the lay bystander’s perspectives on what facilitates CPR and the use of AED in real cardiac arrests, one of the major themes identified was the leadership and feeling a moral obligation to act (sense of collective responsibility). 30 It is important for us in Hong Kong to reconsider how such sense of collective responsibility can be built, and whether legislations can affect the public behaviour and the perceived norm.
Limitation
Although we have included the two largest providers of standard first-aid course and more than 1200 responses, sampling bias may have resulted from the convenience sampling employed. This sample may not be representative of all first-aid course participants in Hong Kong, the untrained bystanders or the general population of Hong Kong.
The response to the GSL related questions may have been compromised due to the poor understanding of the subject by the participants. Only 12.1% of the participants reported to have ever heard of the concept of a GSL, and the rest of the participants reported on the results based on the description of GSL in one sentence. However, this study represents the first significant attempt to gain an important understanding of this topic given the lack of knowledge of GSL in Hong Kong. We postulate that the understanding of GSL may even be lower for the general public.
Finally, our analysis has taken into account all information available with regard to missing data. The effect of missing data was likely to be small given most questions have less than 3% missing responses.
Conclusion
Few first-aid learners in Hong Kong have ever heard of GSL; however, the need for protection and legal immunity for lay rescuers were recognised as important. Based on the findings of the study, we recommend public consultations on the use of legislation for legal protection of bystander rescuers, together with comprehensive public education programme on the importance of bystander CPR. Overcoming the fear of litigation and improving bystander CPR is a priority for improving survival rates from sudden cardiac arrest in Hong Kong.
Footnotes
Acknowledgements
We thank all respondents for their participation in the survey. We sincerely thank Hong Kong St John Ambulance and the Hong Kong Red Cross for their great assistance in the dissemination of the questionnaire.
Author contributions
K.K.C.H. and A.S. conceived the study and designed the study. K.K.C.H. and C.Y.L. conducted the study and performed data collection. K.K.C.H., C.Y.L., A.S. and C.A.G. managed the data, including quality control. K.K.C.H., C.Y.L. and C.A.G. provided statistical advice on study design and analysed the data. K.K.C.H. and C.Y.L. drafted the manuscript, and all authors contributed substantially to its revision. All authors approved the version to be published and take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Informed consent
As the questionnaire was anonymous and the participation was voluntary, the completion and return of the self-administered questionnaire implied consent for the study.
Ethical approval
Ethical approval was obtained from the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong.
Supplemental material
Supplemental material for this article is available online.