
Abstract
Background:
Currently, a large burden of hospital admissions is related to minor head trauma and its related imaging studies. One of the challenging issues for emergency physicians is head computed tomography scan.
Objective:
The aim of this study was to determine whether there are clinical risk factors that may reveal the intracranial pathology occurring after discharge in adult patients who underwent computerized tomography because of mild/minor head traumas. We aimed to evaluate the prevalence of abnormal computerized tomography in these patients.
Methods:
Between January 2013 and December 2017 medical records and imaging findings of patients over 18 years of age who had undergone computerized tomography examination in the emergency department of our hospital were evaluated retrospectively. Patients were divided into groups according to age, sex, symptoms and physical examination findings. The relationship between these findings and abnormal computerized tomography findings was evaluated statistically.
Results:
A total of 619 patients who were admitted to the emergency department for the second time because of the same head trauma and underwent control head computerized tomography were included in the study. Abnormal head computerized tomography findings were found in 7.6% (47) of the patients. Clinical risk factors; Glasgow Coma Scale score, vomiting, loss of consciousness, dangerous trauma mechanism and anticoagulant drug use were significantly correlated with the presence of pathology on head CT(p<0.05).
Conclusion:
Patients who are readmitted to the emergency department due to worsening symptoms after the injury and who undergo control head computerized tomography have the risk of traumatic brain injury as much as those who are admitted for the first time. A very early computerized tomography may cause to miss an evolving bleeding. The presence of one or more of the identified risk factors will help clinicians to decide which patient requires computerized tomography.
Introduction
Head trauma is one of the most common causes of emergency departments (EDs) worldwide. More than 80% of the head traumas presenting to the ED are mild/minor head traumas (MHT) which do not cause severe clinical symptoms or findings. 1 Although the recommendations for approaching patients with Glasgow Coma Scale (GCS) scores of 13 and 14 in published protocols are similar to each other, there is still no clear attitude regarding patients with a GCS score of 15. 2 The incidence of intracranial pathology varies between 4% and 8% in patients with MHT whose GCS score is 15. 3 Since a small number of patients have a pathology requiring surgical intervention, the choice of imaging modalities in the evaluation of head trauma and which patients it will be employed is still a controversial and critical question for physicians working in the ED.
Computerized tomography (CT) is the most important imaging way in the evaluation, follow-up, and treatment plan of head trauma. 1 We have encountered changes noticed in the control CTs that were taken due to worsening symptoms of traumatic patients who underwent CT and were followed up or discharged in the early post-traumatic period. In this study, the patient group with MHT whose head CT were taken were evaluated retrospectively. The patients, whose first CTs were normal in the radiological appearances and were discharged from the hospital, were included in the study. We evaluated the control head CTs of these patients admitted to the ED for the second time due to the same head trauma. Our aim is to find out the clinical parameters that may indicate intracranial pathology that is not determined in the first neuroradiological evaluation following the trauma but occurs after discharge and to speculate about which patients should undergo CT. We aimed to evaluate the incidence of abnormal head CT in these patients.
Methods
This is a retrospective cohort study carried out in the ED of a university-affiliated training hospital. This hospital is a level 1 trauma center for both adults and pediatric patients. The number of annual average patients admitted to the ED is 300,000, and trauma patients accounted for 10% of this number. The ethics committee approval of the study was obtained from the ethics committee of Aksaray University (approval no: 2018-102). Between January 1, 2013 and December 31, 2017, the files of all patients over 18 years of age who had undergone head CT scan and admitted to the ED were scanned through the hospital electronic database. Radiological imaging results, discharge epicrisis, requested consultation results, and duration of discharge were evaluated. According to the information obtained from patients’ epicrisis, the patients whose first head CTs were normal but were readmitted to the ED with the same blunt MHT and underwent head CT for the second time after being discharged were included in the study. According to clinical risk factors, abnormal head CT findings of patients who underwent control head CT after discharge were recorded. The demographic characteristics of the patients, symptoms at the time of admission to the ED, trauma type, physical examination findings, CT findings (first and control CT), and GCS scores were evaluated retrospectively. The main criterion for MHT was that the GCS score was 14 or above. CT was accepted as a reference method to show traumatic brain injury (TBI).
According to the medical history at the admission to the ED, vomiting, headache, change in consciousness, abnormal behavior, seizure (post-traumatic seizure or seizure suspicion), retrograde amnesia which lasts more than 30 minutes, scalp hematoma, anticoagulant drug intake (warfarin, clopidogrel, fractionated, or unfractionated heparin), dangerous trauma mechanism (vehicles’ crash into a pedestrian, being thrown away from a motor vehicle, falling: >1 m, or fall from five steps), alcohol, or drug poisoning were identified as risk factors. The time between injury and admission to the ED, reported head CT results by radiologist, neurosurgical intervention, and whether there was death or not were recorded.
Patients with other system injuries except head trauma were regarded as multi-body trauma. Patients under 18 years, multiple trauma patients, patients whose trauma history is not primary or clear (e.g. after epileptic seizure, syncope), patients with a GCS score of <14, penetrating injuries, gunshot wounds, the patients who had intracranial pathology in the CT taken at admission, whose CT scan was not of diagnostic quality due to artifacts, who had focal neurological deficit at the time of admission, and the patients who were pregnant were excluded from the study.
Primary outcome was the presence of traumatic intracranial injury in the second head CT of the patients readmitted. Traumatic intracranial injury in head CT includes any intracranial bleeding (epidural, subdural, intracerebral, and subarachnoid), pneumocephalus, contusion, or cerebral edema. Secondary outcome was to investigate the relationship between the determination of pathological findings in head CT and age, sex, trauma mechanism, complaints, physical examination findings, GCS score, and presence of additional conditions (anticoagulant intake, drug intoxication, and alcohol intake) of the patients. In addition, estimating the need for surgical intervention was the other outcome point. Neurosurgical results were defined as invasive intracranial pressure measurement by any method, craniotomy, burr hole procedure, hematoma discharge and dura repair. If the patients died of head trauma, they were recorded as dead.
Statistical analysis
The analysis of the study data was performed by SPSS for Windows version 15.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used for demographic and clinical features in the MHT (mean (standard deviation (SD)) and n (%)). The statistical significance of the risk factors that may have an impact on the detection of pathology in the head CT was evaluated by Pearson’s Chi-Square or Fisher’s exact test. Odds ratio and 95% confidence intervals (CIs) for each variable were calculated. Univariate and multivariate logistic regression analyses were performed on statistically significant clinical risk factors to determine whether the parameters predicted correctly the presence of pathology in head CT. Statistically non-significant parameters were excluded in the regression model. As a result, multivariate logistic regression model included GCS score, age, anticoagulant drug use, loss of consciousness (>5 s), and dangerous trauma mechanism. According to the Hosmer and Lemeshow test, multiregression analysis model was found suitable. Results for p < 0.05 were regarded as statistically significant.
Results
We retrospectively reviewed the records of a total of 11,845 patients who presented to our ED with MHT between 1 January 2013 and 31 December 2017. Intracranial imaging revealed that 11,237 MHT patients were determined with no pathology and discharged. Out of these patients, a total of 634 patients who were admitted to the ED for the second time due to the same head trauma and who received control head CT after discharge were included in the study. Fifteen patients with incomplete data were excluded and finally 619 patients were included in this study. Of the cases, 170 were female (27.5%) and 449 (72.5%) were male. The ages of the cases ranged from 19 to 78 years, with a mean age of 38.65 ± 15.65 years (Table 1). The cases over 60 years old consisted of 13.4% of the patients (n: 83). The mean duration of admission to the ED for the second time was 23.10 ± 9.5 h.
Demographic characteristics of patients (n = 619).
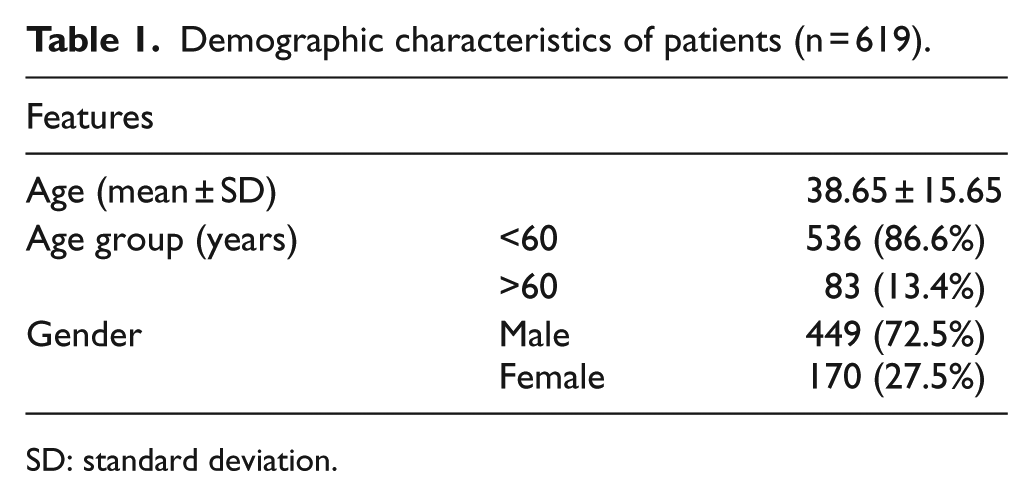
SD: standard deviation.
There was a significant relationship between age, vomiting, loss of consciousness, GCS score, dangerous trauma mechanism, and anticoagulant drug use and the presence of pathology in head CT (p < 0.05). Incidence of traumatic injury in head CT was significantly higher in those over 60 years (p < 0.001), loss of consciousness (p < 0.001), dangerous trauma mechanism (p: 0.026), and GCS scores 14 (p < 0.001; Table 2). Traumatic injury was determined in 7.6% (n: 47) of all patients. Of the patients, 1.7% underwent neurosurgical treatment. While 57.4% of the patients with traumatic injury were under 60 years of age, 42.6% were over 60 years. GCS score was 14 in 42.6% of the patients diagnosed with traumatic injury in CT and GCS score was 15 in 57.4% of the patients. The most common abnormal head CT finding in all ages was epidural hematoma (3.1%; Table 3). Neurosurgical treatment was performed in six patients (0.9%) accompanied by epidural bleeding and in five patients (0.8%) who developed subdural hematoma. No additional neurosurgical treatment was required during follow-up of the cases operated.
Investigation of the effects of demographic characteristics, symptoms and findings of patients, who underwent CT scan for head trauma, on determining abnormalities in head CT.
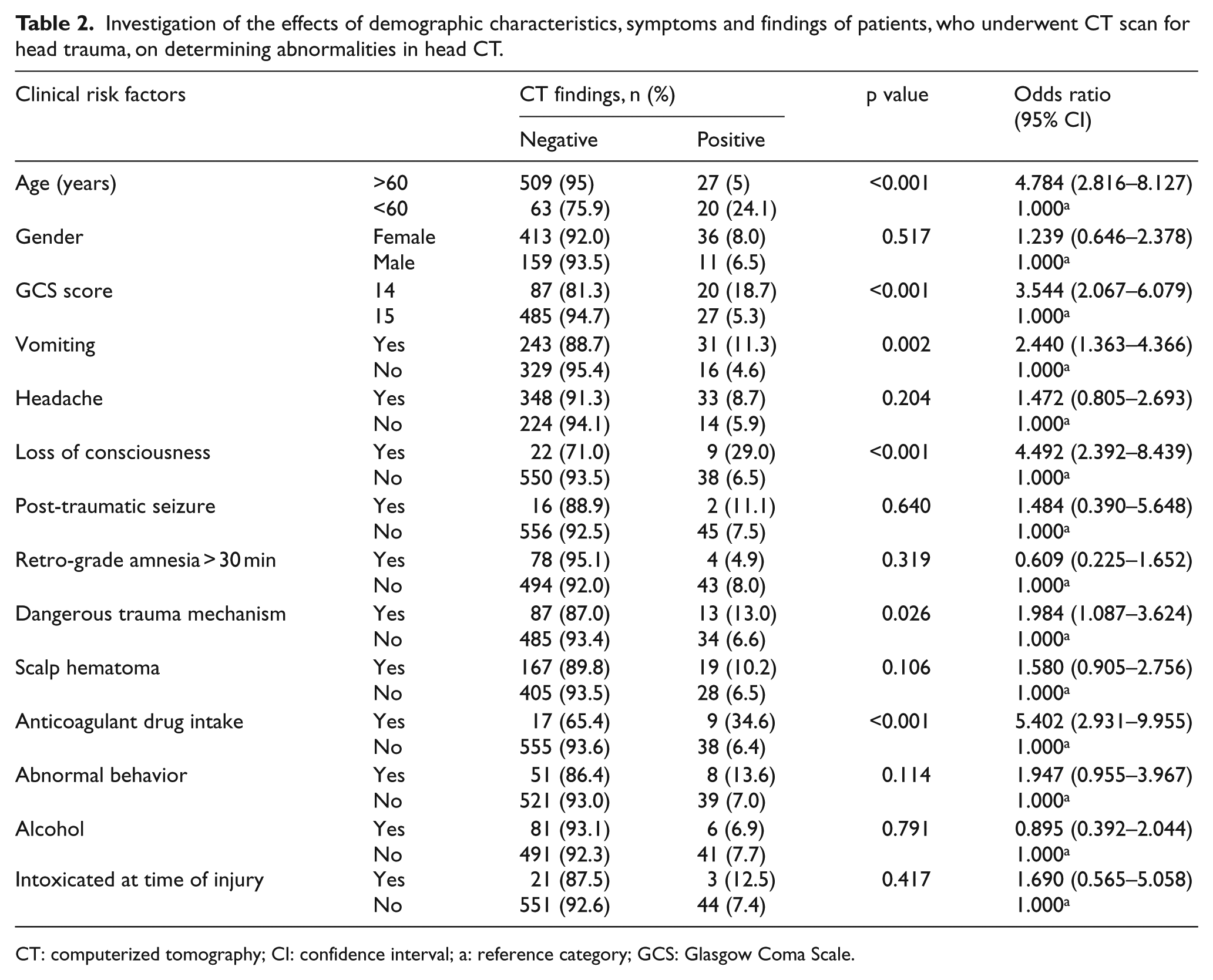
CT: computerized tomography; CI: confidence interval; a: reference category; GCS: Glasgow Coma Scale.
Abnormal findings of head CT.
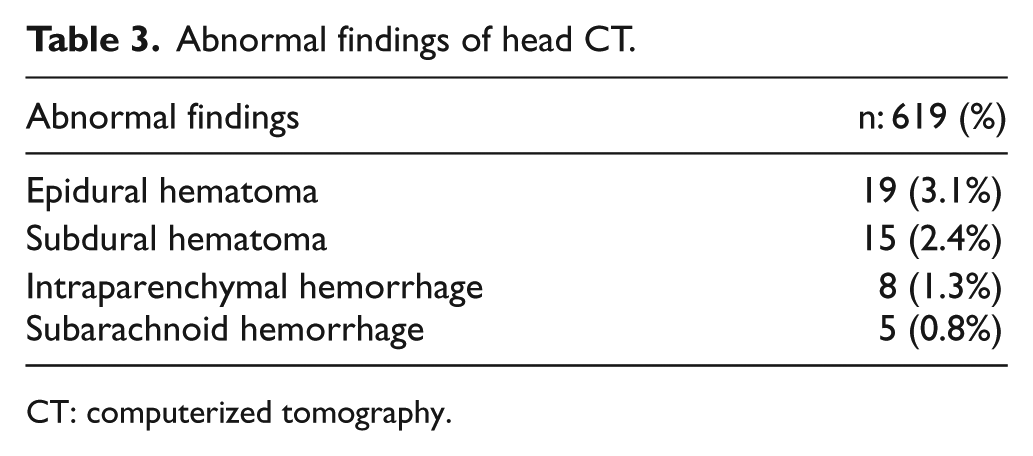
CT: computerized tomography.
Headache, post-traumatic seizure, retrograde amnesia, gender, presence of trauma related to intoxication, and use of alcohol were found to have no statistically significant difference in revealing traumatic injury in CT (p > 0.05). Univariate and multivariate regression analyses were performed for the clinical risk factors determined to have significant relationship between the presence of traumatic injury in head CT such as age, GCS, dangerous trauma mechanism, unconsciousness, and anticoagulant drug use. In particular, the presence of GCS 14, being over 60 years old, use of anticoagulants, loss of consciousness, and the presence of a dangerous trauma mechanism increase the likelihood of traumatic injury in CT. The related test results are given in Tables 4 and 5.
Univariate regression analysis of parameters that may be related to the pathology in head CT.
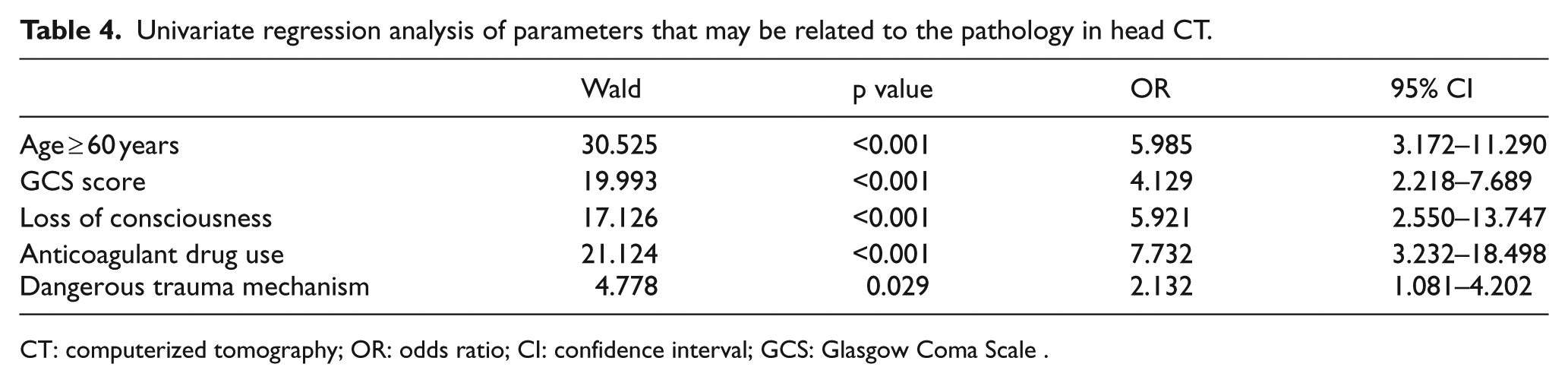
CT: computerized tomography; OR: odds ratio; CI: confidence interval; GCS: Glasgow Coma Scale .
Multivariate regression analysis of parameters that may be related to the pathology in head CT.
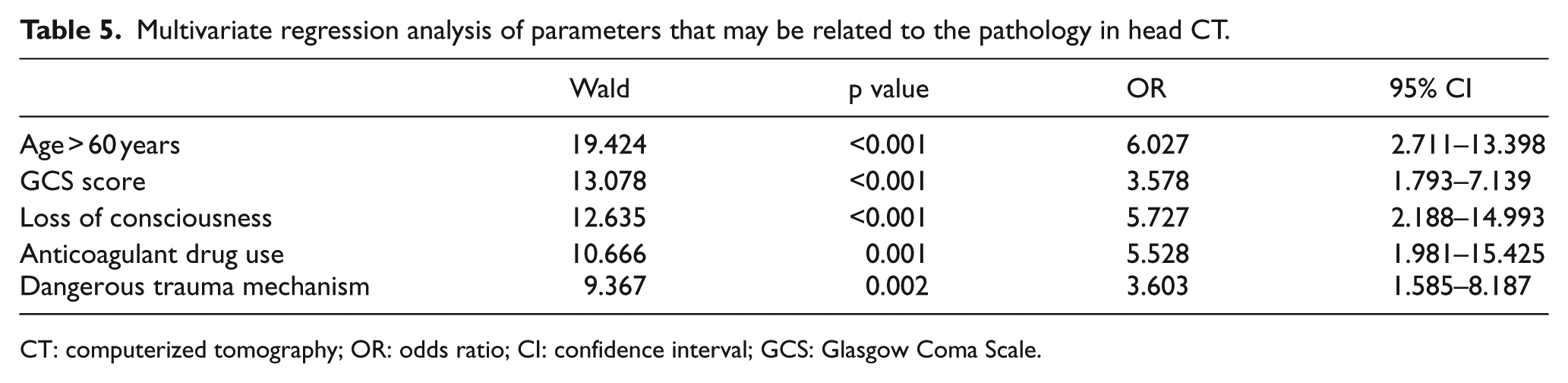
CT: computerized tomography; OR: odds ratio; CI: confidence interval; GCS: Glasgow Coma Scale.
Discussion
MHT is one of the most important public health problems frequently encountered in ED. 4 Although the number of patients is very high, intracranial pathology is detected only in a very small group of these patients. For this reason, many studies have tended to identify subgroups with higher risk, based on clinical parameters. 5 In the literature, studies have been published on which patients should undergo CT scan and protocols have been proposed in patients with MHT.6,7
There is no study in the literature on patients who were readmitted to the ED and underwent control head CT for MHT. In this study, we detected intracranial pathology in control CTs taken due to worsening symptoms after discharge in 7.6% (n: 47) of the 619 patients with MHT who had undergone CT and discharged before. Neurosurgical treatment was performed in six patients (0.9%) accompanied by epidural bleeding and in five patients (0.8%) who developed subdural hematoma. In a study conducted by Falmirski et al., 8 abnormalities were determined in CT in 6% of the patients with MHT. Borczuk 9 found the incidence of pathology in CT in patients with mild clinical signs and symptoms as 8.2% in their study on 1448 patients. In this study, abnormal CT findings similar to those reported in the literature were also detected in the patients who underwent CT for the second time for the same head trauma as in the first admission of the cases with MHT.3,8,9
Management of patients with a GCS score of 15 is still a controversial subject. 2 However, there is no clear consensus among the authors on the need for CT for patients with GCS scores of 14–15.10–13 Therefore, the objective is to determine the risk factors associated with intracranial pathology and to demonstrate the indications of CT in patients with GCS scores of 14–15. In this study, intracranial pathology was detected in 27 (5.3%) patients with a GCS score of 15 at the time of readmission and who underwent control CT and in 20 (18.7%) patients with a GCS score of 14. Abnormal head CT in patients with a GCS score of 14 was significantly higher than those with 15 (p < 0.001). According to the results of this study, we suggest that patients should be evaluated with CT according to the accompanying symptoms and findings in patients with a GCS score of 15 at admission.
Symptoms and signs of headache and vomiting were detected more frequently in the patient group determined with intracranial pathology. There was a significant relationship between the presence of pathology in head CT and clinical risk factors; GCS (p < 0.001), vomiting (p = 0.002), loss of consciousness (p < 0.001), dangerous trauma mechanism (p = 0.026), anticoagulant drug use (p < 0.001), and being above 60 years (p < 0.001). In this study, the other symptoms and findings were not found as statistically significant risk factors.
The most common complaints of patients following head trauma include headache and vomiting. They investigated whether these complaints would be accepted as a risk factor or not. While some studies2,14 reported that they had no significance, in some studies 15 it was reported that a higher proportion of intracranial lesions were observed in patients with this type of complaints. In this study, a significant relationship between vomiting and intracranial pathology in CT was determined.
Kutlay et al. 16 examined 7 delayed epidural cases and 48 cases reported in the literature. They reported that these hematomas occurred between the third hour and sixth day following the trauma. Poon et al. 17 detected late epidural hematoma in 22 patients in the study including 73 patients in whom they investigated traumatic epidural hematoma and reported the incidence rate as 30%. For the diagnosis of late epidural hematoma, an epidural hematoma should not be detected in the first head CT. 18 In this study, although first CT scans of 19 (3.1%) patients were normal, an epidural hematoma was detected in the control CTs taken at readmission. The symptoms of epidural hematoma depend on the type and rate of bleeding, the presence and location of cerebral injury, time of post-traumatic head CT scan (a very early CT may cause to overlook an evolving bleeding).19,20 In patients with MHT, observation is important in those with GCS scores of 14–15 in the case of a late epidural hematoma. We also detected subdural hematoma in 15 (2.4%) patients. Subdural hematoma was detected in 14 (93.3%) patients over the age of 60 years. Although the first head CT was normal, bleeding revealed in control CT could be attributed to the fact that as the brain volume is reduced in elderly patients, hematoma volume will not cause any push and neurological deficits in the brain unless the volume of the hematoma reaches large dimensions, and the patients may generally be admitted to the hospital in the later period as the leaks and tears in the bridging veins will fill the area during the later period.21,22
In the studies conducted by Gutman et al. 23 and Borczuk, 9 it was reported that being over 60 years of age was a risk factor. Mower et al. 24 reported that intracranial pathology was rarely observed in patients under 65 years of age without scalp hematoma, fracture, coagulopathy, and persistent vomiting in a study of CT scans of more than 13,000 mild to moderate head trauma patients. When the patients included in this study were examined, it was seen that there were signs and symptoms requiring CT according to the risk factors defined in the literature.
Patients using anticoagulants (warfarin, clopidogrel, etc.) are considered to be at risk more in terms of traumatic intracranial hemorrhage (TIH). Recent studies have reported the incidence of TIH as 6.2%–29% in patients with anticoagulants and who have been exposed to MHT. This means that in such cases, we should probably pull the head CT scan level down slightly. 25 Many guides have stated that it is necessary to observe the patient for a certain period of time for monitoring even if there is no pathological finding in the first CT of the patients with head trauma and using anticoagulants and control head CT should be taken if necessary.25,26 There are even studies recommending routine control CT. One of these studies is the study conducted by Joseph et al. 26 with 1606 cases in 2014. In the study, recurrent and/or delayed bleedings have been reported especially in patients receiving clopidogrel. The authors recommend routine control CT scan for patients with head trauma and using anticoagulant. In this study, the detection of abnormal pathological findings in nine (34.6%) patients using anticoagulant supports these studies. A significant relationship was found between the use of anticoagulant drugs and the presence of pathology in head CT (p < 0.001). Even if there were no pathological findings in the initial CT of the patients with head trauma and using anticoagulants, we determined that the patient should be kept under observation for a certain period of time and control cranial CT should be taken if necessary.
This study has some limitations. First, this study is retrospective and all cases with MHT between January 2013 and December 2017 were not included in the study, but only patients, who were readmitted to hospital because of suffering from trauma and underwent head CT, were evaluated. Second, CT was accepted as the reference method to show TBI. In patients who had no pathological findings in CT, abnormalities can be detected in magnetic resonance imaging (MRI). The number of patients was limited because the files with no desired data were included in the study, which is the other limitation of the study.
Conclusion
The presence of one or more of the identified risk factors may help clinicians to decide which patient requires CT. Patient should be kept under observation even if the first CT is normal for delayed TIH and control CT should be considered if clinical changes occur. As a result, although tomography has high sensitivity in detecting hemorrhage, as in this study, sometimes radiological images in older patients, especially with epidural and subdural hemorrhages due to anticoagulant use can be seen later than clinical symptoms. A very early CT may cause to overlook an evolving bleeding. Patients with one or more risk factors are at increased risk for the development of intracranial pathology. In this regard, repeated control radiological examinations should be planned if there is a history of clinical risk factors, especially vomiting, loss of consciousness, dangerous trauma mechanism, and anticoagulant use.
Footnotes
Author contributions
H.M. and K.K. researched literature and conceived the study. E.T.S. was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. H.M. wrote the first draft of the manuscript. All the authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author.
Informed consent
For this retrospective study, formal consent is not required.
Ethical approval
Aksaray University School of Medicine, Aksaray Education and Research Hospital Scientific Research Evaluation Committee approval was obtained for this study (approval number: 2018/102).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.