
Abstract
Background:
We generally keep relatives out of the area while a critical intervention so they cannot observe the management. Recent studies recommend witnessing of the resuscitation by arguing that it supports the patient’s relatives’ beliefs that everything that could be done had been done.
Objective:
We investigated the influence of family witness on the anxiety of patients’ relatives and on the healthcare team.
Methods:
This study was planned as a prospective observational study. The critical patients who were managed in the resuscitation room with or without intubation were included in the study. The State-Trait Anxiety Inventory survey form was given to patients’ relatives. Healthcare providers were given a survey, including a visual analog scale of anxiety.
Results:
The mean visual analog scale score of healthcare providers was 4.37 ± 2.5. The mean visual analog scale score of allied health personnel was similar to resident doctors but lower than consultant doctors. The anxiety of healthcare providers was higher during witnessed management. In the witnessed management group, the anxiety of healthcare providers was higher in patients who received cardiopulmonary resuscitation. The mean State-Trait Anxiety Inventory anxiety score of patients’ relatives was 50.2 ± 10.3. In witnessed management, the mean anxiety score was 49.5 ± 11.3; in non-witnessed management, the score was 51.0 ± 9.3. The anxiety of patients’ relatives was not higher, but rather slightly lower during witnessed management of patients.
Conclusion:
In our study, the anxiety of healthcare providers was higher in family-witnessed management. It was argued that consultant physicians were more anxious because they have more responsibility about the patients. With witnessed management, the anxiety of patients’ relatives could be reduced, but it is more ominous for healthcare professionals.
Introduction
The relatives of critically ill patients are an indivisible part of patient management. 1 Acknowledging this point and creating an approach that includes the patient’s relatives in medical management are important parts of the medical management of the patients.2,3 We generally keep relatives out of the resuscitation area so they cannot observe the management. Recent studies recommend witnessing of the resuscitation by arguing that it supports the patient’s relatives’ beliefs that everything that could be done had been done. It also eases the acceptance of death and grieving process for many and does not interrupt or adversely affect medical efforts during resuscitation.4–9 Doyle et al. 7 concluded that a lay person may wish to be with family members who may be dying, even though resuscitation efforts are being made, and that it is reasonable to inquire about this wish. This condition resulted in a new approach called “family-witnessed resuscitation (FWR),” which can be described as keeping the patient’s relatives inside the resuscitation room during cardiopulmonary resuscitation (CPR).10–12 The concept of FWR was first described in the 1980s in North America, but it was not brought to clinical practice until 1994 in Europe.5,12,13 Even after Doyle et al. allowed FWR in their clinic and reported the radical studies, additional studies remained limited to small surveys or anecdotes.14,15
There are mixed feelings about FWR within the healthcare system. The healthcare staffs in support of FWR believe that it is a fundamental right of the patient’s relatives.4,6,9 Despite the studies that showed the benefits of FWR, this practice is still controversial among the health professionals. One of the biggest concerns of employees is that FWR will have a negative impact on family members. 16 Yanturali et al. 13 reported that the healthcare staff that does not support FWR generally believes that this process will increase the anxiety of the resuscitation team. The results of a study investigating the impact of FWR on post-traumatic stress disorder symptoms indicated that the family’s existence is associated with more positive psychological outcomes on families and that the relatives of patients do not interfere with employees or cause conflicts between health staff and family members. 17 Similarly, there is evidence to show that families want to stay with their relatives during CPR.18–20
In this study, we investigated the influence of families witnessing the management in resuscitation rooms on the anxiety of the relatives and healthcare professionals. We wanted to learn whether family witnessing decreases the anxiety of the patients’ relatives and healthcare professionals or not.
Methods
We performed this prospective randomized-controlled open-label, single center, interventional study in the emergency department of Bagcilar Education and Research Hospital, Istanbul, Turkey, after approval from the local ethical committee. We included the first 100 patients that were admitted to the resuscitation room of the emergency department whose relatives signed the informed consent and agreed to participate to the study.
Before the study, we explained the study protocol to all healthcare staff in the emergency department. We prepared 100 envelopes including either “witnessed” or “non-witnessed” and after equally mixing the envelopes they had been placed in a box. When a patient was admitted to the resuscitation room, we took an envelope from the box to specify if it would be “witnessed” or “non-witnessed.” When the procedure was to be a witnessed intervention, one of our staff briefly asked the patient’s relatives, “We have a study about witnessed intervention. Do you want to watch the medical intervention?” If the patient’s relatives did not agree to be included in the study, the envelope was put back into the box. When the procedure was to be a non-witnessed intervention, one of our staff briefly asked the patient’s relatives, “We have a study about patients who have been admitted to resuscitation room. Do you want to participate in the study?” If the patient’s relative did not agree to be included in the study the envelope was put back into the box. In Figure 1, we reported the number of included and excluded patients. One of the non-witnessed cases was excluded after we completed the study due to missing data.
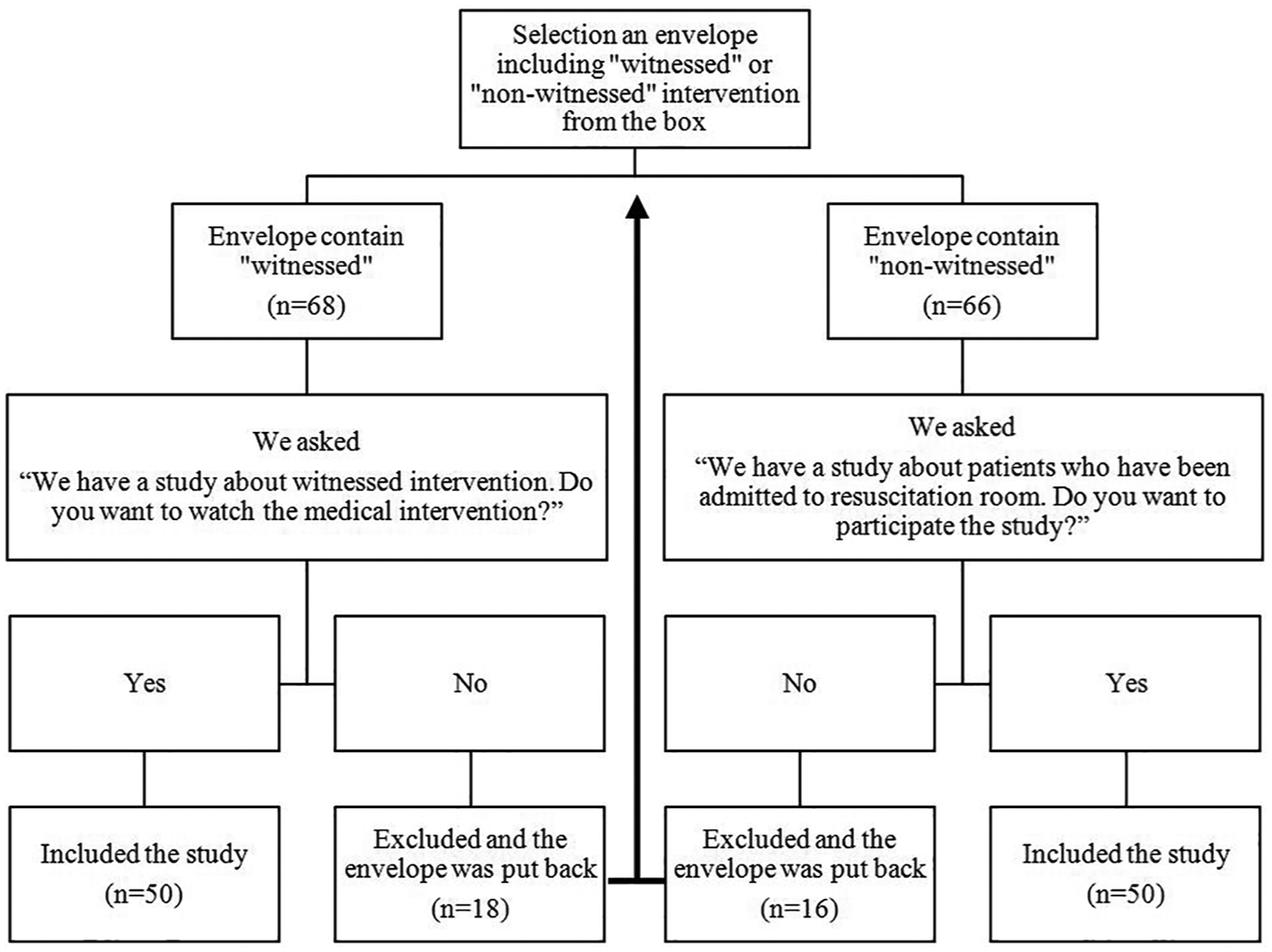
The selection and number of included and excluded participants.
The state anxiety of the relatives was evaluated with Spielberger’s “The State-Trait Anxiety Inventory” (STAI). 21 The STAI inventory has 20 items for assessing trait anxiety and 20 for state anxiety; we only used the state anxiety form (STAI TX-I). In addition, we recorded whether the patient had been admitted for a traumatic or non-traumatic condition, whether CPR was applied, the duration of resuscitation, the age of the patient, and the ages of the patient’s relatives.
We recorded the job of the healthcare staff (whether consultant physician, resident doctor, or nurse) and we used the visual analog scale (VAS) to evaluate the anxiety of the healthcare staff. We did this by asking them to specify the severity of anxiety they felt, on a scale of 1 to 10, during the intervention. We also recorded their age, work experience, and opinion about family witness (FW).
Family-witnessed intervention procedure
We remodeled the resuscitation room by opening a window that was 100 cm in length and 50 cm in height (Figure 2), including a lid that could be opened or closed inside the resuscitation room. The patients’ relatives who agreed to be included in the study and wanted to watch the intervention waited in front of the window. We opened the window lid every 10 minutes for 1 minute to show the intervention. After the intervention was completed, we asked the participants to complete the questionnaire, including age, sex, job information, and the STAI TX-I form.
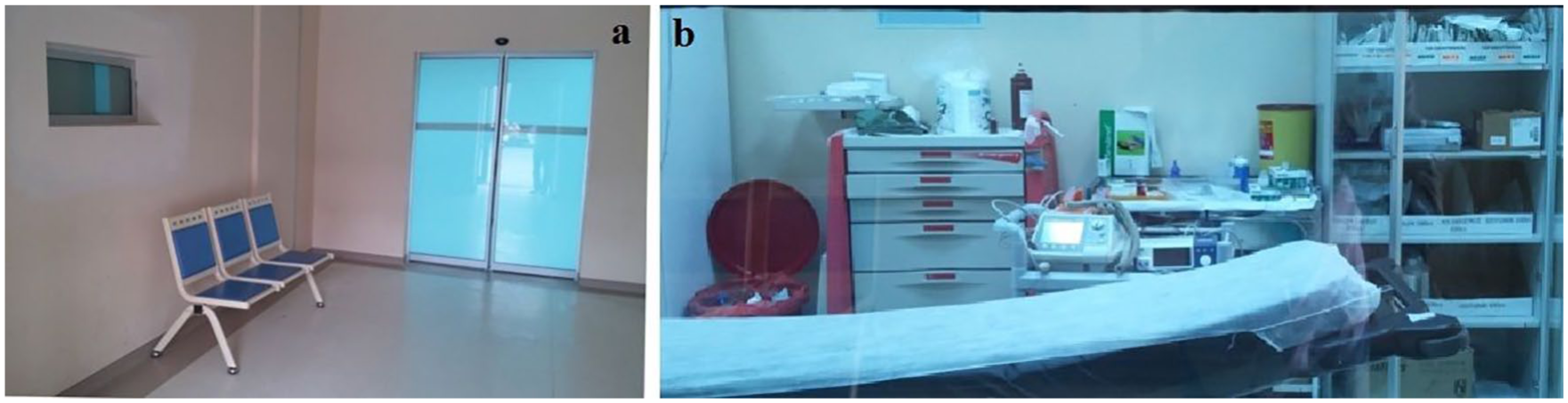
(a) The waiting area of the patients’ relatives and window (left side) for watching inside the resuscitation room and (b) the interior view of the resuscitation room from window
Non-witnessed intervention procedure
After the intervention was completed, we asked the relatives in the study if they wanted to complete the questionnaire, including age, sex, job information, and the STAI TX-I form. After they completed the study form, we allowed the patients’ relatives to watch the additional interventions if they wanted.
All statistical analyses were calculated by SPSS 17.0 for Windows (New York, USA). The continuous variables were expressed as mean ± SD. The categorical variables were expressed as n (%). The normal distribution was determined by Kolmogorov Smirnov test and histogram. The differences of continuous variables that are not normally distributed between groups were calculated by the Mann–Whitney U test for two groups and the Kruskal–Wallis Test for more than two groups. The Student’s t test was used for normally distributed data and the chi-square test was used for categorical variables. The correlations of the continuous variables were calculated by Pearson correlation and r value between 0 and 0.3 (mild correlation), 0.3 and 0.7 (moderate correlation), and 0.7 and 1 (high correlation); p ≤ 0.05 was regarded as significant with a 95% confidence interval. After the intervention was completed, we asked the relatives in the study if they wanted to complete the questionnaire, including age, sex, job information, and the STAI TX-I form. After they completed the study form, we allowed the patients’ relatives to watch the additional interventions if they wanted.
Results
The mean age of the patients was 66.5 ± 17.9 (median = 70; range = 4–90 years). The mean age of patients’ relatives was 40.6 ± 10.9 (median = 40; range = 22–65 years). The mean age of the patients in both the witnessed and non-witnessed groups was similar (p = 0.745). Also, the mean age of the patients’ relatives was similar in both groups (p = 0.989). Males made up 60.6% of the patients, the gender distribution was similar in both groups (p = 0.592).
The mean anxiety VAS score of the healthcare staff was 4.37 ± 2.5. The mean anxiety VAS score of nurses was 4.1 ± 2.1, 4.5 ± 2.9 in resident doctors, and 6.4 ± 3.6 in consultant physician. The anxiety VAS scores were similar between nurses and resident doctors (p = 0.782). The mean anxiety VAS score of consultant physicians was greater than nurses, but it was not statistically significant (p = 0.085). The anxiety VAS scores of resident doctors and consultant physicians were similar (p = 0.403). The mean anxiety VAS scores for both genders of the healthcare staff were similar (p = 0.166).
If we evaluate the mean anxiety VAS scores separately in the witnessed and non-witnessed groups, the mean anxiety VAS score was 5.1 ± 2.8 in the witnessed group and 3.5 ± 1.8 in the non-witnessed group. The mean anxiety VAS score was greater in the witnessed group (p = 0.007).
There were only two pediatric patients whose ages were 4 and 7 years old, so we did not compare pediatric patients with others. The anxiety VAS score had no correlation to the age of the patient, age of medical staff, CPR duration, and age of patient relative (p values were 0.460, 0.569, 0.846, and 0.971, respectively), but there was a mild negative correlation to the experience of the medical staff (p = 0.049, r = –198), while the experience increases with the decrease in anxiety VAS score. When we looked at these correlations in two groups separately, similar results were observed. In the witnessed group, the anxiety VAS score had no correlation to the age of the patient, age of medical staff, CPR duration, or age of patient’s relative (p values were 0.315, 0.684, 0.053, 0.104, and 0.967, respectively). In the non-witnessed group, the anxiety VAS score had no correlation to the age of the patient, age of medical staff, CPR duration, or age of patient relative (p values are 0.778, 0.085, 0.375, 0.430, and 0.989, respectively).
After the FW, we asked the medical staff for their opinion about FW. In 42.0% of the witnessed interventions, the medical staff had positive opinions about FW. However, in 58.0% of these interventions, the medical staff indicated their discomfort during the witnessed intervention. The opinion about FW had a moderate and positive correlation to discomfort during the medical intervention (p < 0.001; r = 560). So, we argued that the bias of the medical staff about FW may be a factor that influences the discomfort of them during medical intervention.
The anxiety VAS score of medical staff was similar whether CPR was performed or not if the intervention was non-witnessed (p = 0.989), but if the medical intervention was witnessed, the anxiety VAS score was higher if CPR was performed (p = 0.026). The box-blot graph of the anxiety VAS scores of medical staff according to performing CPR and witnessing is expressed in Figure 3.
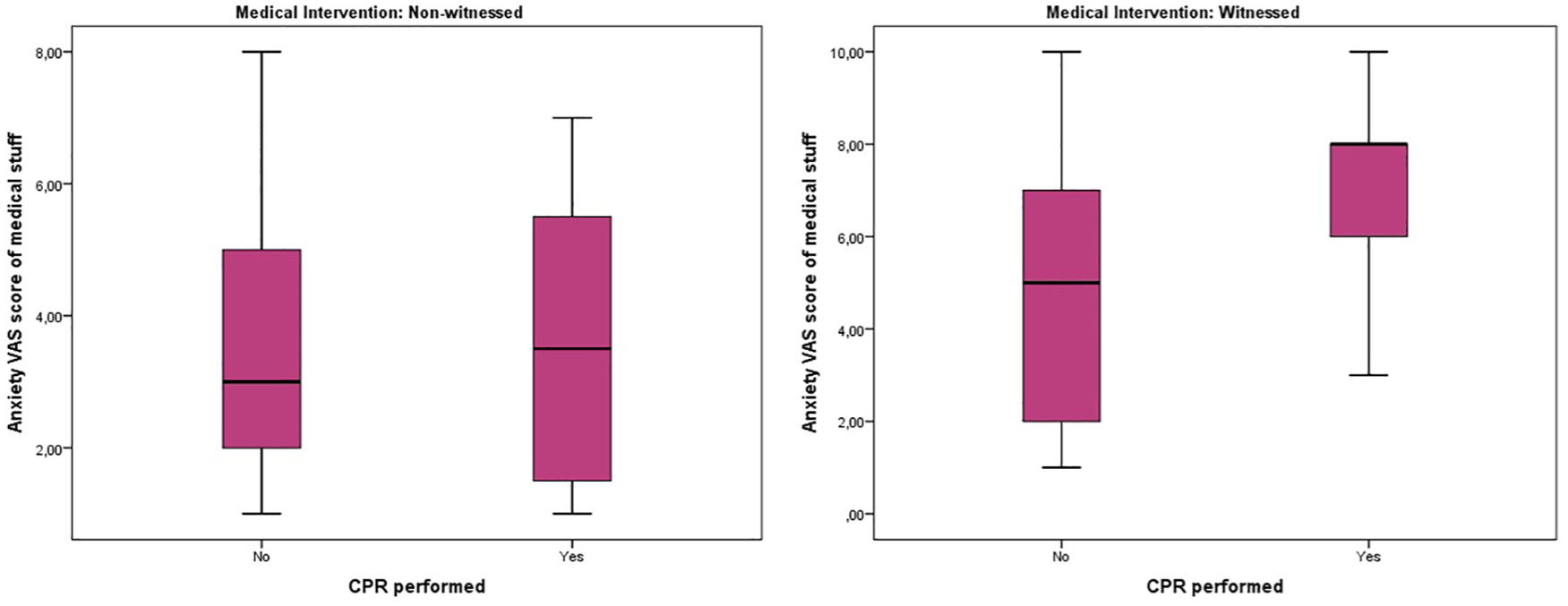
The box-blot graph of anxiety VAS score of medical stuff according to performing CPR and witnessing.
The mean state STAI point of the patients’ relatives was 50.2 ± 10.3. In witnessed intervention, it was 49.5 ± 11.3, and in non-witnessed intervention, it was 51.0 ± 9.3. The STAI score of the groups were similar (p = 0.452).
The STAI score had no correlation to the age of the patient, age of medical staff, CPR duration, VAS score of medical staff, and age or gender of patient relative (p values were 0.352, 0.635, 0.741, 0.485, 0.453, 0.800, and 0.058, respectively). We asked the patients’ relatives in the non-witnessed group if they wanted to watch the additional interventions, 71.4% of them wanted to watch the intervention.
The STAI score of patients’ relatives were similar if CPR was performed or not performed in both the witnessed and non-witnessed group (p values were 0.383 and 0.700). The box-blot graph of state anxiety STAI score of patients’ relatives according to performing CPR and witnessing is expressed in Figure 4.
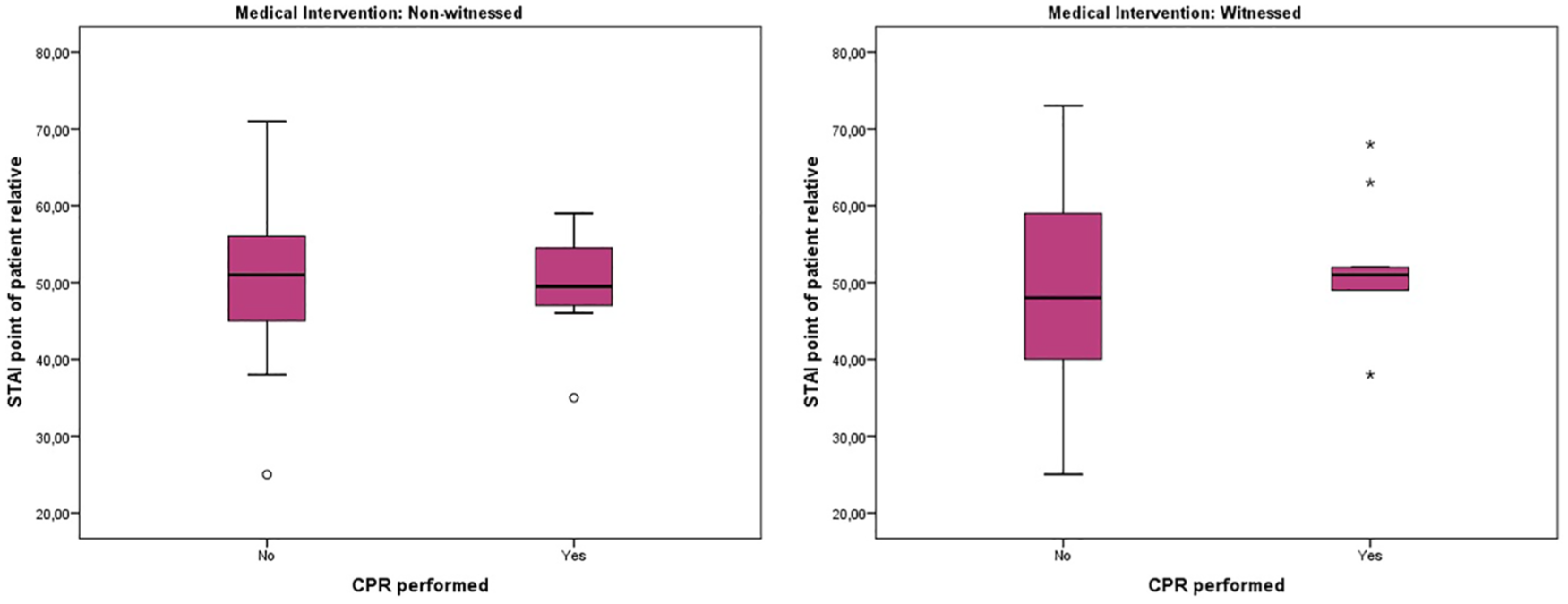
The box-blot graph of state anxiety STAI point of patient relatives according to performing CPR and witnessing.
Discussion
The concept of FWR startles healthcare professionals; the main concern is the risk that it can increase the stress of the resuscitation team. 13 Despite the studies that indicate that families want to be more involved in the care of critical patients, 22 health workers are more distant from FWR.16,23 Boyd and White 24 reported that FWR did not increase the stress of medical staff. There are available studies that indicate positive effects of FWR on mourning and mental health of patients’ relatives. 25 In our study, the anxiety VAS score of medical staff was similar if CPR was performed or not performed if the intervention was non-witnessed, but if the medical intervention was witnessed, the anxiety VAS score was higher if CPR was performed. So, we can argue that the resuscitation increases the anxiety in FW.
Jabre et al. 26 compared psychological outcome of family members whom witnessed and not witnessed the resuscitation of a relatives in their study, which was a randomized-controlled study. He concluded that witnessed family members had fewer common complaints like post-traumatic stress disorder, depression, anxiety, and complicated mourning than unwitnessed group. However, we investigated that the anxiety VAS score of medical staff was higher during FW compared with a non-witnessed investigation. Similar to our study, Compton et al. 25 reported that medical staff felt uncomfortable during resuscitation, especially in urban hospitals. Pasquale et al. 27 reported that healthcare professionals stated that resuscitation watched by family members of a patient can be stressful. On the contrary, DeWitt 28 reported that presence of family members could prolong unnecessary resuscitation. Fulbrook et al. 29 stated that nurses worried about misunderstanding of their behaviors as careless, indifferent, or disrespectful by witnessed family members while managing such a stressful situation. Another common problem is FWR-related medico legal issues. The literature supports the opinion of these as ungrounded fears and FWR causes less legal issues than private resuscitation process. 30
In a survey study about acceptance of FWR, 80%–86% of the intensive care unit healthcare professionals do not allow this procedure in adult patents and pediatric patients, since family members would be a distraction to the resuscitation team. 31 In a study which assessed healthcare professionals’ experiences and attitudes toward FWR, 55.6% of participant doctors and approximately one-third (31.4%) of participant nurses stated that presence of a family member during CPR is not beneficial for the patient. 32
In our study, after non-witnessed intervention, our medical staff supported FW at a percent of 55.1, but after witnessed resuscitation, this was 42.0% with the remaining 58% not in support of FW. Also, 42.0% of the medical staff indicated that they felt discomfort during witnessed resuscitation. McClenathan et al. 31 reported that 80% of doctors and 57% of nurses did not support FWR in their study. In the same way, Badir and Sepit 33 reported that 83.1% of the nurses thought there was no need to keep the patient relatives inside during resuscitation, 69.1% did not want them to stay inside. In addition, 78.8% of the doctors did not want the patients’ relatives to stay inside during resuscitation. Pasquale et al. 27 reported that 17.5% of trauma surgeons and 63.6% of emergency nurses had a favorable impression of the presence of patients’ relatives during resuscitation. In the study of Waldemar and Thylen, 32 less number of nurses compared to doctors (20.5% as against 41.2%) thought that presence of a family member affects the healthcare provider’s concentration negatively. In the same study, approximately half of the doctors (53.9%) and one-third of nurses (34.5%) stated that FWR should not be the routine procedure. The frequency of discomfort of our staff was slightly lower than in previous studies. This could be a result of the format of the practice. In previous studies, generally, patients’ relatives waited inside the resuscitation room, but we kept them outside the resuscitation room, only allowing them to see the intervention through a window. So, medical staff felt more comfortable because there was no risk of being interrupted by a relative.
Mortelmans et al. 34 interviewed with CPR survivors and 72% of participants preferred presence of a family member during resuscitation. Our study revealed that the anxiety of the patients’ relatives was slightly lower in witnessed intervention, but it was statistically not significant. So, we can say that witnessed intervention does not increase the anxiety of patients’ relatives. Similarly, Pasquale et al. 27 reported that the anxiety of patients’ relatives was lower in witnessed intervention. According to our study, anxiety STAI points of relatives were similar in both the witnessed and non-witnessed group, even if CPR was applied to the patient.
Anxiety and stress during FWR could be arised from insecurities of personnel while performing under stressful situations. 35 In our study, the anxiety VAS scores were similar between nurses and resident doctors, but consultant physicians’ VAS score was greater than nurses and it was not statistically significant. Omran et al. 36 stated that nurses who had less years of experience in the profession had more favorable attitude toward FWR and were more positive than doctors and participants. In our study, the anxiety VAS scores of resident doctors and consultant physicians were similar. The mean anxiety VAS scores for both genders of the healthcare staff were also similar.
The fact that families are not near their relatives during CPR may create a perception that something is being hidden from them. Family witnessing can help ensure the transparency of this process. 19 Not to be a part of the resuscitation could lead to guilt in family members because they cannot be together with their loved ones at their most vulnerable moments. In the study of McLaughlin et al., 37 80% of 135 people who lost a family member stated that they want to be there during resuscitation or at least they wish to have the option to be there. In our study, we asked the patients’ relatives in the non-witnessed group if they wanted to watch the additional interventions, 71.4% of them wanted to watch the intervention. In Leske et al.’s 38 study, participating in the FWR option reduced anxiety and stress and increased family welfare.
In conclusion, witnessing resuscitative intervention did not increase the anxiety of patients’ relatives. It even decreased the anxiety of the relatives, but it increased the anxiety of the healthcare providers. Also, further studies can be done that compare keeping the patients’ relatives inside the resuscitation room with keeping them outside and letting them watch in an appropriate waiting area.
Limitations of the study
We could not perform any anxiety tests before the procedure because of time limitation. Also, anxiety level could have varied with health issues and other individual characteristics of patient’ relatives. In our study, the fact that the relatives of the patients were not taken into the resuscitation room is one of the important limitations, and also the patients’ families were informed only at the beginning of the intervention. The most serious concern while planning the study was the safety of health workers. FW is not a routine procedure in our country. Therefore, the relatives of the patients were not taken into the intervention room and were only able to monitor their relatives’ interventions through a window. Another limitation is that pediatric and adult patients are not evaluated separately. The number of pediatric patients admitted during the study period was very low and was not statistically significant.
Footnotes
Acknowledgements
The manuscript is not under publication or consideration for publication elsewhere.
Authorship
All of the authors declare that they have all participated in the design, execution, and analysis of the paper, and that they have approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data could be sent on demand.
Informed consent
We performed this prospective observational study in the emergency department of Bağcılar Education and Research Hospital, Istanbul, Turkey, after approval from the local ethical committee. After we started the study, we included the first 100 patients that were admitted to the resuscitation room of the emergency department whose relatives signed the informed consent a degreed to participate in the study. Before the study, we explained the study protocol to all healthcare staff in the emergency department. We prepared 100 envelopes including either “witnessed” or “non-witnessed” equally, mixed the envelopes and put them in a box. When a patient was admitted to the resuscitation room, we took an envelope from the box to specify if it would be “witnessed” or “non-witnessed.” When the procedure was to be a witnessed intervention, one of our staff briefly asked the patient’s relatives, “We have a study about witnessed intervention. Do you want to watch the medical intervention?” If the patient’s relatives did not agree to be included in the study, the envelope was put back into the box. When the procedure was to be a non-witnessed intervention one of our staff briefly asked the patient’s relatives, “We have a study about patients who have been admitted to resuscitation room. Do you want to participate in the study?” If the patient’s relative did not agree to be included in the study the envelope was put back into the box. In ![]() , were ported the number of included and excluded patients. One of the non-witnessed cases was excluded after we completed the study due to missing data.
, were ported the number of included and excluded patients. One of the non-witnessed cases was excluded after we completed the study due to missing data.
Ethical approval
We performed this prospective observational study in the emergency department of Bağcılar Education and Research Hospital, Istanbul, Turkey, after approval from the local ethical committee.
Human rights
This study was conducted in accordance with the Declaration
Patient disclosure and approval form
This study, which is planned as a specialist thesis in Bağcılar Education and Research Hospital Emergency Medicine Clinic, invests the effect of the resuscitation protocol on the anxiety of the patient’s relatives. Witnessed resuscitation means that all resuscitation procedures are performed near the patient’s relatives. In this study, it is asked to fill the Spielberger State Anxiety Inventory (STAI), which consists of 20 questions and measures the immediate anxiety state of the patient’s relatives, among the relatives who are admitted to the resuscitation room. The patient’s relatives will be able to follow the resuscitation procedure through the glazed window to the room if they want to. Indicate whether or not you agree to participate in the study by marking one of the “I want to join/do not want” boxes and filling in the information below.
□ I want to join
□ don’t want
Name:
Surname:
Date:
Sign: