
Abstract
Background:
Advanced cardiac life support provides healthcare professionals with knowledge and skills needed in dealing with cardiac emergencies. By incorporating e-learning in advanced cardiac life support courses, it allows for easier accessibility of learning materials and a more personalized learning schedule at a lower overall cost.
Objectives:
This study aims to compare the outcome of e-learning advanced cardiac life support versus conventional advanced cardiac life support among healthcare professionals and determine their attitude on e-learning.
Methods:
A total of 96 candidates attending advanced cardiac life support courses in Hospital Universiti Sains Malaysia between January 2016 and May 2017 were included in the study. In total, 48 candidates were enrolled on each arm. Candidates in conventional advanced cardiac life support undertook a 2-day face-to-face course. Participants in e-learning advanced cardiac life support completed 6 h of online lecture videos prior to 1-day modified face-to-face course. All candidates were assessed by pre- and post-course multiple-choice questions and practical cardiac arrest simulation test. Only post-course and cardiac arrest simulation test marks contribute to the passing or failure of the candidates.
Results:
Candidates in e-learning advanced cardiac life support courses had higher mean scores on the pre-course multiple-choice questions (69.1, SD: 19.1) compared to those in conventional advanced cardiac life support courses (58.6, SD: 16.6, p < 0.001). The cardiac arrest simulation test pass rate on e-learning advanced cardiac life support was higher than conventional advanced cardiac life support courses although statistically not significant (95.8% vs 87.5%; p = 0.134). The overall pass rate was 93.8% for e-learning advanced cardiac life support versus 83.3% in conventional advanced cardiac life support (p = 0.099). A majority of the candidates had positive attitude towards e-learning.
Conclusion:
E-learning advanced cardiac life support courses demonstrated better results in terms of knowledge compared to conventional advanced cardiac life support, with equivalent skill scores. Shorter course duration, lesser cost and participants’ satisfaction were the added benefits. Further study can be done to explore the utilization of e-learning materials among healthcare professionals and its other advantages.
Introduction
Advanced cardiac life support (ACLS) refers to a set of clinical interventions for urgent treatment of cardiac arrest and other life-threatening medical emergencies. 1 It provides a uniform approach to management, which includes manual defibrillation, advanced airway, drug therapy and peri-arrest and post-resuscitation treatment. 2 ACLS knowledge and skills are important to healthcare professionals as it has been proven to improve the outcome of cardiac arrest patients. 3
Most tertiary hospitals in Malaysia offer ACLS training to cope with the increased demand of trained personnel in dealing with cardiac emergencies. However, not many can have the opportunity to attend an ACLS course due to its lengthy duration and cost. The number of courses is also limited depending on the availability of qualified instructors. Theoretical knowledge and performance skills degrade quickly in the span of 3–12 months 4 even though ACLS certification lasts for 2 years. Hence, suggestions have been made to reduce the duration of certification and increase the number of refresher courses. However, this may place a huge burden on the healthcare system to run a large number of ACLS courses yearly.
The ACLS course which incorporated e-learning, or e-learning advanced cardiac life support (e-ACLS), was introduced in our setting, in view of the above-mentioned situation. E-learning is an evolution of distance learning, which has taken advantage of the cutting-edge tools to materialize in the context of technologies for structuring education. 5 Also known as electronic educational technology, it has gained a lot of fame in the past decade. However, its use has been restricted to basic sciences rather than in clinical settings. 6
A previous study showed that e-ACLS had a comparable outcome with the conventional method of full-time learning with instructors and reported greater satisfaction among participants. 7 By reducing the face-to-face aspect, the monetary cost of facilitating an ACLS course was drastically reduced by almost 50%. 8 Cheaper ACLS courses allow more healthcare professionals to be trained to provide better cardiac care. Since the number of instructors can be reduced, more refresher courses can be provided to enhance retention of ACLS knowledge. Frequent accessibility to online learning materials was also proven to improve long-term memory retention 9
Our aim in this study is to introduce e-ACLS among our healthcare professionals and compare its effectiveness, as well as to determine participants’ attitude towards e-learning. With accessible and standardized e-ACLS module, it is hoped that more ACLS-trained healthcare professionals can be produced, thus improving the standard of cardiac care in Malaysia.
Methods
A prospective interventional study was carried out in a teaching hospital in Kelantan, Malaysia from January 2016 to May 2017. There were two phases in this study.
Phase 1: designing the assessment tools and e-learning modules
Theoretical multiple-choice questions (MCQs) and practical cardiac arrest simulation test (CAS test) were selected from our ACLS data bank as the assessment tools, to ensure that the examinations conducted in this study are similar to the standardized ACLS assessment. Three sets of theoretical questions were prepared, each consisting of 30 best of five questions. The three sets were randomly selected for pre- and post-course assessment and remedial for those who failed. Practical CAS test was designed to assess the candidates’ ability in patient assessment, airway management, electrical therapy and basic life support. The MCQs and CAS test questions were content validated by senior lecturers and specialists of Emergency Medicine Department, Hospital Universiti Sains Malaysia (HUSM). In the meantime, e-learning modules were produced by the Emergency Department team and uploaded online. For this study, only those who joined the e-ACLS group had access to the modules during the study period.
Phase 2: intervention
Two conventional advanced cardiac life support (c-ACLS) courses followed by two e-ACLS courses were conducted to reduce contamination bias among our subjects. Participants were given a choice to undergo the courses according to their preferences, since the courses were not fully sponsored. Therefore, participants’ selection bias could not be avoided. However, post hoc analysis to control the confounding factors was done later.
The c-ACLS participants were given ACLS manuals 4 weeks prior to the 2-day course. Pre-course MCQs were given on the course day followed by 1½-day face-to-face lectures and practical sessions with instructors. Post-course MCQs and practical CAS test were conducted at the end of day 2. The candidate had to pass both the post-course MCQ and CAS test to be considered pass. The pre-course MCQ results did not contribute towards the final assessment. The passing mark for the post-test theory questions was 60%, as decided based on experts’ opinion following the validation process. If a candidate failed, the number of attempts for each assessment and the respective marks were recorded. A maximum of two attempts for each assessment were allowed.
The e-learning ACLS groups were given access to online ACLS modules 4 weeks before the course, apart from the ACLS manuals. The online modules consisted about 6 h of recorded lectures and moulage scenarios accessible at their own convenience. The topics covered included electrocardiogram (ECG) interpretation, basic life support, ACLS algorithm, fluid and drug therapy, electrical therapy, airway management, post-resuscitation care and ACLS moulage scenarios. Each video lasted 10–20 min, with certain topics broken to several parts, to ensure better attention span and participant’s engagement. They underwent a modified 1-day face-to-face course which consisted of pre-course MCQs, refresher lectures and practical session followed by post-course MCQs and practical CAS test on the same day. Since the online module did not include practical training, similar practical session as in conventional course was carried out. Similar methods of assessment were conducted as in the c-ACLS group. Additional questionnaires to assess the attitude towards e-learning were given to the e-ACLS group on the same day. The questionnaire was adapted from a validated questionnaire by Pierce and Fox, consisting eight components on e-learning (seven positive-ended questions and one negative-ended question towards e-learning). 10 The suitability of the questions in our population was tested by face validation. Participants were allowed to withdraw from any part of the study without any unfavourable circumstances.
We maintained the same assessors and assessment tools for both c-ACLS and e-ACLS groups. However, the assessors were not blinded to the mode of the course since the duration of e-ACLS courses was reduced.
Statistical analyses were carried out using Statistical Packages for Social Science (SPSS), version 22.0. Descriptive analyses were expressed as frequencies, means with standard deviation and percentages. Statistical significances were calculated using independent t-test between groups and paired t-test within groups for continuous variables. A p-value < 0.05 is considered as statistically significant for all statistical analyses in this study.
Results
A total of 98 candidates were recruited from two c-ACLS and two e-ACLS courses. However, only 96 participants were included in the study with 48 candidates on each arm, as two of the candidates withdrew from the study. The mean age in the c-ACLS was 33.2 years (SD: 6.6) versus 30.2 years (SD: 5.4) in e-ACLS. Table 1 shows that the socio-demographics factors of all the participants in both arms which include gender, race and designation (doctor vs paramedic) were highly comparable. A previous experience in managing ACLS cases was also similar. Chi-square test showed that the differences were not significant. However, more participants in c-ACLS (40%) had previous ACLS course attended, compared to 10% in e-ACLS group.
Socio-demographic data of c-ACLS and e-ACLS participants.
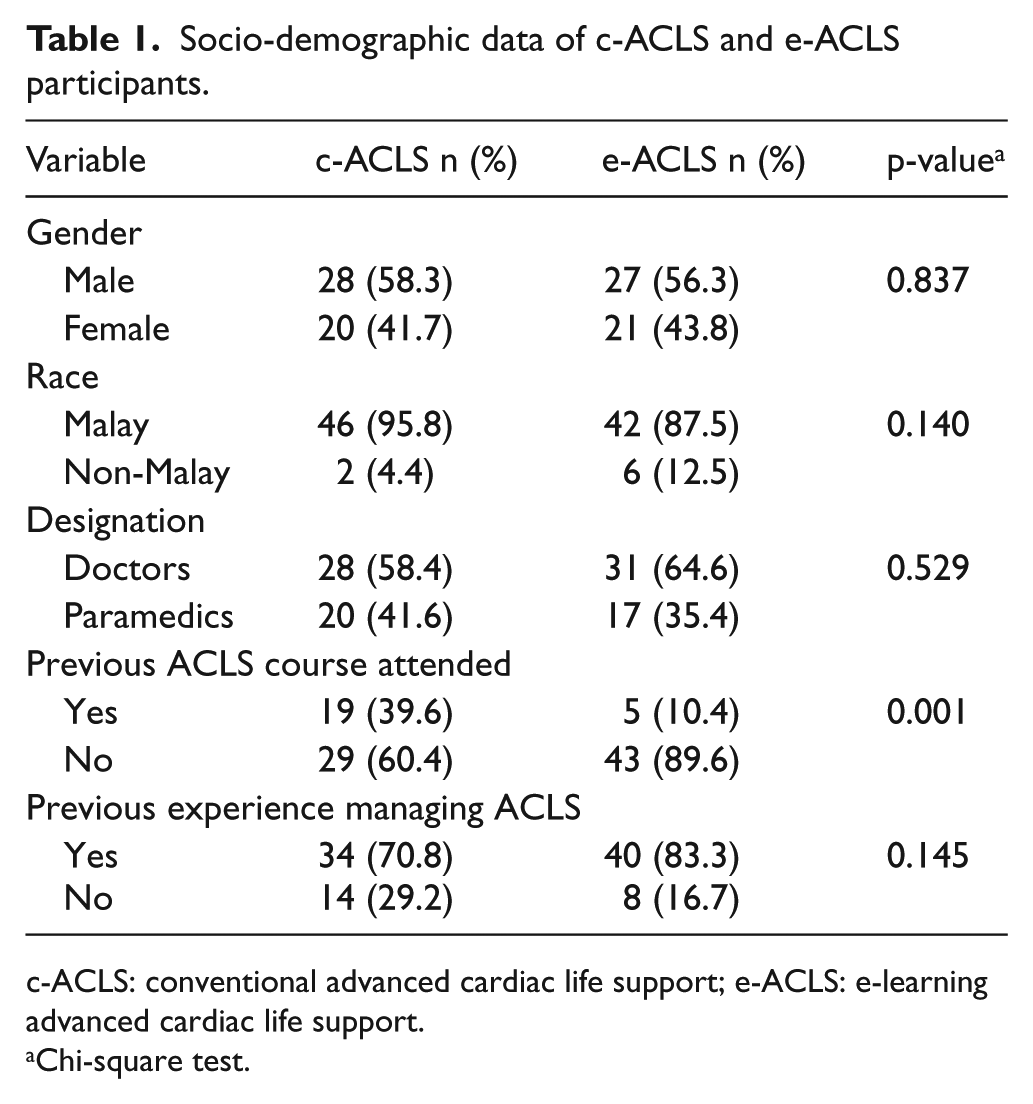
c-ACLS: conventional advanced cardiac life support; e-ACLS: e-learning advanced cardiac life support.
Chi-square test.
Candidates’ overall results are portrayed in Table 2. From the study, it was observed that the mean pre-course MCQ marks in e-ACLS participants was higher than those in c-ACLS group (69.1 (SD: 19.1) versus 58.6 (SD: 16.6)), and the difference was significant with p-value < 0.001. The mean post-course MCQ marks was also significantly higher for the e-ACLS group at 78.9 (SD: 12.0) compared to 70.6 (SD: 13.9) for c-ACLS (p-value < 0.001). Both groups showed an increase in the mean post-course marks compared to the pre-course marks using paired t-test analysis. The differences were significant for both groups (mean difference: 12.0, p-value < 0.001 in c-ACLS group and mean difference: 9.8, p-value < 0.001 in e-ACLS group).
Assessment results for c-ACLS and e-ACLS participants.
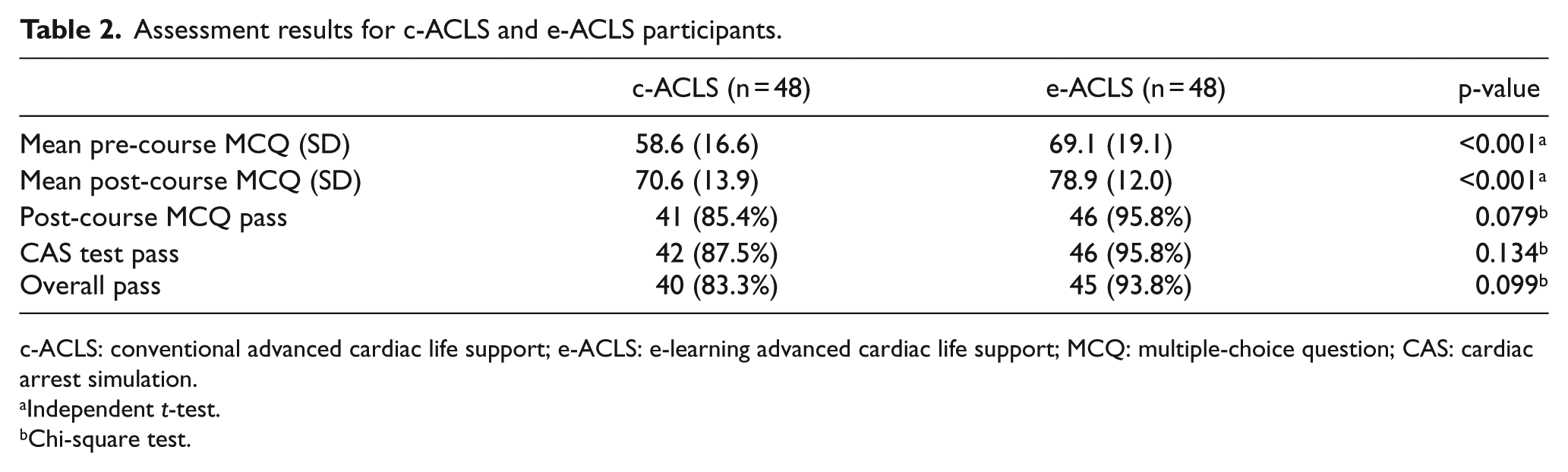
c-ACLS: conventional advanced cardiac life support; e-ACLS: e-learning advanced cardiac life support; MCQ: multiple-choice question; CAS: cardiac arrest simulation.
Independent t-test.
Chi-square test.
The practical CAS test results showed that more candidates passed in e-ACLS (95.8% vs 87.5% in c-ACLS), but the result was not significant (p-value = 0.134). Although the overall course passing rate was higher in e-ACLS (93.8% vs 83.3%), the difference did not reach statistical significance (p-value = 0.099).
Based on the questionnaire to assess the attitude on e-ACLS among healthcare professionals (which consists of seven positive-ended questions and one negative-ended question), most candidates favoured e-learning (Table 3). A majority (96%) agreed that viewing the videos was essential; 58% felt that e-learning could replace face-to-face teaching, while 85% believed that e-learning should be used as adjunct to conventional instructor teaching.
Score on attitude towards e-learning among e-ACLS participants (n = 48).
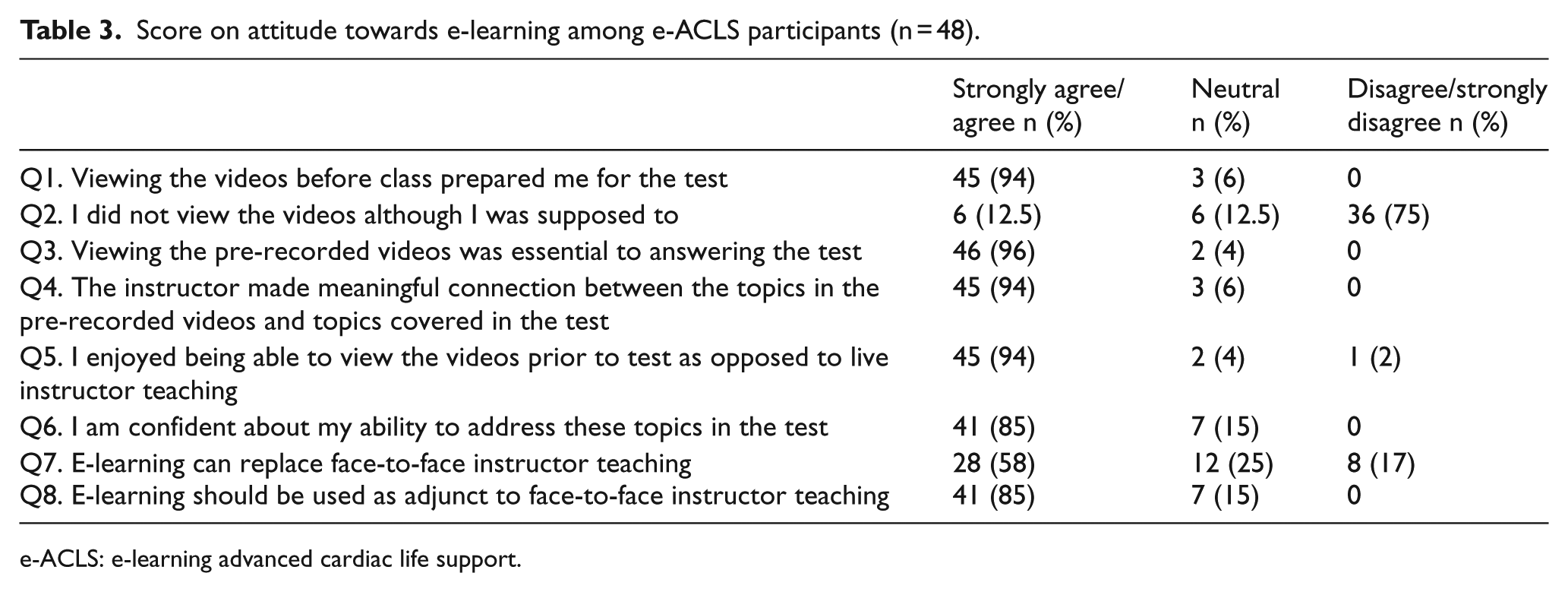
e-ACLS: e-learning advanced cardiac life support.
Discussion
Although the utilization of e-learning for education is gaining popularities nowadays, adapting it in clinical settings is still in its infancy. However, our experience in incorporating e-learning in our ACLS courses which include teaching clinical assessment and interventions in urgent treatment of cardiac arrest shows mainly promising results.
The candidates in e-learning group showed higher pre- and post-course marks on ACLS knowledge. Evidently, the advantage of having e-learning modules on top of ACLS manuals helped them in performing better for the course. The modules also prepared them for the face-to-face classes with the instructors. This finding was also demonstrated in an observational study by Thorne et al., 7 whereby pre-test marks of the e-ACLS candidates were significantly higher than conventional ACLS candidates. Similar finding was observed in a systematic review by the International Liaison Committee on Resuscitation (ILCOR) in 2010, which showed that candidates having prior e-learning study modules were prepared equally or better than conventional learning on the theoretical aspects of resuscitation. 11
In our study, the e-ACLS group had comparable practical test results to their c-ACLS counterparts, with 95.8% and 87.5% passing rates, respectively. This shows that despite shorter course duration, the participants were still able to perform for their practical assessment. Adequate time was able to be allocated for practical session, since most of the theoretical knowledge was delivered online beforehand. The practical session was needed since certain aspects in ACLS training such as team dynamics and teamwork skills were not emphasized in online modules. However, on the contrary, a study carried out by Perkins et al. 8 demonstrated that candidates in e-ACLS courses had lower simulation test pass rates. Another study by Christenson et al. 12 demonstrated that candidates who were trained solely on e-learning ACLS were more likely to compromise their practical resuscitation capabilities. Few factors could contribute to this, such as candidates having lesser discussion time and inadequate interaction with their instructors to clarify their doubts pertaining to ACLS. 7 In this study, candidates received about the same amount of practical session as those attending c-ACLS courses, and this was proven to be sufficient for them to gain adequate ACLS knowledge and skills. The overall passing rates were also similar between the two groups. This shows that, despite limited instructor–candidate face-to-face time, e-ACLS course is as effective as the conventional ACLS in preparing candidates for the post-course theoretical and practical exams.
Although the candidates were not randomized prior to the assessment, both groups showed similar demographic parameters. Using chi-square test, the parameters such as gender, race, designation and previous experience in managing ACLS cases showed no significant difference. However, more participants in the c-ACLS had attended ACLS courses previously (39.6% in c-ACLS vs 10.4% in e-ACLS). Based on a study by Thorne et al., 13 participants with previous ACLS course experience performed better in their ACLS tests. However, in our study, those in the e-ACLS group had higher mean marks and passing rates, even though more participants had no previous experience in attending ACLS course. Therefore, the difference seen was minimal.
Since our participants are from working classes, having e-learning–based courses would provide as an advantage as it gives freedom in choosing the most appropriate time for them to engage with the teaching sessions. It also gives flexibility to the candidates in deciding which materials or modules to learn. They can choose topics to focus on and replay certain topics, and this would enhance retention of knowledge. This flexibility feature of e-ACLS allows candidates with different learning requirements to plan their own study method that fits them. 14 Thus, it is more of candidate-centred rather than instructor-centred.
On the contrary, reducing lecturer–candidate face-to-face time lessens the burden and time spent by ACLS instructors. This enables the instructors to conduct more ACLS courses. Hence, more healthcare professionals can be trained. This directly translates in improving the healthcare provided for cardiac arrest patients. At the same time, reduced duration of e-ACLS courses also reflects a cheaper cost in facilitating ACLS courses, which again enables more ACLS courses and training to be conducted.
In addition, we received mainly positive responses from our participants on e-ACLS courses. In a survey to determine their attitude towards e-learning, majority agreed that e-learning should be used as an adjunct to face-to-face instructor teaching. More than half agreed that e-learning could replace face-to-face sessions with the instructors. Despite watching a pre-recorded lecture, many admitted that the instructors were able to deliver the topics and made connections with the topics covered in the assessment. However, about 13% of the participants did not watch the videos beforehand. This is probably because this method of conducting ACLS courses is still unfamiliar to them. Hence, more exposure towards e-learning courses is needed to ensure better acceptance from the participants. Furthermore, by implementing methods to trace the time spent watching the videos as well as providing rewards when they complete the video sessions, we can also improve the view.
There is a tremendous rise in demand among healthcare professionals towards e-learning ACLS. With all the benefits of e-learning approach, there is a strong reason to incorporate e-learning into our existing and upcoming ACLS programmes. This dissemination of e-learning ACLS translates to the improvement in the quality of patient care in cardiac emergencies.
Limitation
It was not determined whether the candidates had accessed all the learning materials prior to the course or the time spent on the video sessions. Further study can be done to explore the utilization of e-learning materials among healthcare professionals and further understand their attitude towards online education.
Conclusion
Evidently, the e-ACLS course is better in providing knowledge and has comparable results in preparing the candidates with CAS skills compared to conventional course. It also has many other benefits such as reduced course duration, cost and burden on the instructors. As a result, more courses can be organized, and thus more candidates can be trained. At the same time, candidates have the flexibility in studying the modules according to their preferences and learning requirement, giving them opportunity to plan and study what they need. In our study, it is also evident that candidates preferred e-learning and agreed that it should be used as an adjunct to face-to-face instructor teaching. As such, it is reasonable to recommend that e-learning ACLS should be further utilized to fortify our cardiac care.
Footnotes
Acknowledgements
The authors would like to acknowledge Universiti Sains Malaysia for funding this project via its short-term grant.
Author contributions
A.A.A., J.N., T.H.T.K., A.Y.M.N. and A.R. participated in study design and intervention. A.A.A., J.N., T.M.A.T.H. and J.B. were involved in data collection, analysis and the writing of the paper. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universiti Sains Malaysia short-term grant.
Availability of data and materials
Unpublished data or material from the study is available upon request from the corresponding author via email.
Ethical approval and informed consent
Ethics approval was obtained from Human Research Ethical Committee, Universiti Sains Malaysia (ref: USM/JEPeM/14100389). Written informed consent for participation and permission to use the data for publication were obtained from the participants.
Human rights
The authors had ensured there was no violation of human rights concerning to the study.