
Abstract
Background:
While there are intrinsic differences in the pros and cons between plain radiographs and computer tomography, the role of pelvic radiographs in polytrauma management is diminishing as computer tomography scans are becoming more accessible. Previous studies found varying results in the inter-observer agreement in pelvic radiograph interpretations.
Objectives:
To evaluate inter-observer agreement of classifying pelvic fractures in major trauma patients by emergency physicians, and the inter-method agreement between plain radiographs and computer tomography scans.
Methods:
Three hundred sixty-nine patients with pelvic trauma were recruited from the trauma registries of four designated trauma centres in Hong Kong, each having one set of anteroposterior pelvic radiographs and pelvic computer tomography scans. Pelvic radiographs were classified by two emergency physicians using Young–Burgess classification, and pelvic computer tomography scans classified by an experienced radiologist. Disagreed pelvic radiographs were evaluated by a senior emergency physician to make a final decision before comparing with computer tomography scans. Cohen’s kappa was used to measure the inter-observer and the inter-method agreements, in the groups ‘mechanism of injury’, ‘stable versus unstable fractures’ and ‘complete classification’.
Results:
Inter-observer agreements of plain radiograph classification for ‘mechanism of injury’, ‘stable versus unstable fractures’ and ‘complete classification’ were moderate to substantial (κ = 0.72, 0.60 and 0.55, respectively). Inter-method agreement for the three groups between plain radiographs and computer tomography were fair to moderate (κ = 0.42, 0.59 and 0.38, respectively).
Conclusion:
The inter-method agreement between plain pelvic radiographs and computer tomography scans was fair in classifying pelvic fractures, and moderate in detection of unstable pelvic fractures. If the patient is haemodynamically unstable or when computer tomography is unavailable, it is reasonable to obtain plain radiographs to screen for unstable pelvic fractures to expedite early intervention. A review in the education approach and material of Young–Burgess classification may improve inter-observer agreement.
Introduction
Background
Pelvic fracture is one of the most challenging conditions to manage in the emergency department (ED). The mortality rate of pelvic fractures has been reported to be 8% to 16%. 1 , 2 Early detection of unstable pelvic fractures is pertinent to the survival of polytrauma patients. The advanced trauma life support (ATLS) guideline used to suggest mandatory plain pelvic radiograph as part of the ‘trauma series’ radiographs. 3 The World Society of Emergency Surgery (WSES) proposed the use of pelvic radiograph and extended-focused assessment with sonography for trauma (E-FAST) in the ED in haemodynamic and mechanic unstable patients with pelvic trauma to identify the injuries to expedite early mechanical stabilisation, early angioemobilization, pre-peritoneal pelvic packing and resuscitation endovascular balloon occlusion of aorta (REBOA), if the patient was found to have peritonism on physical examination, positive E-FAST or positive diagnostic peritoneal aspiration. 4
In the 1980s, Young and colleagues 5 , 6 devised a classification system of pelvic ring injuries based on the injury mechanism (Figures 1 & 2), using pelvic radiographs with anteroposterior (AP), pelvic inlet and outlet views, followed by a classification-driven treatment protocol. Other classification systems have been proposed since, such as the Tile classification system 7 or the Academic of Orthopaedics and Orthopaedic Trauma Association (AO/OTA) classification, 8 but none is used with the same frequency and uniformity as the Young–Burgess system.9–11 Studies also showed the Young–Burgess system has a superior inter-observer reliability compared with Tile or AO/OTA system.9–11 Young and Burgess did not initially include the concept of pelvic ring ‘stability’ in their system. Eastridge et al. 12 and later Manson et al. 13 found out that by dividing pelvic fractures into stable and unstable types, the unstable fractures classified under this system predict a higher mortality rate, abdomen injury rate, chest injury rate and higher transfusion rate.
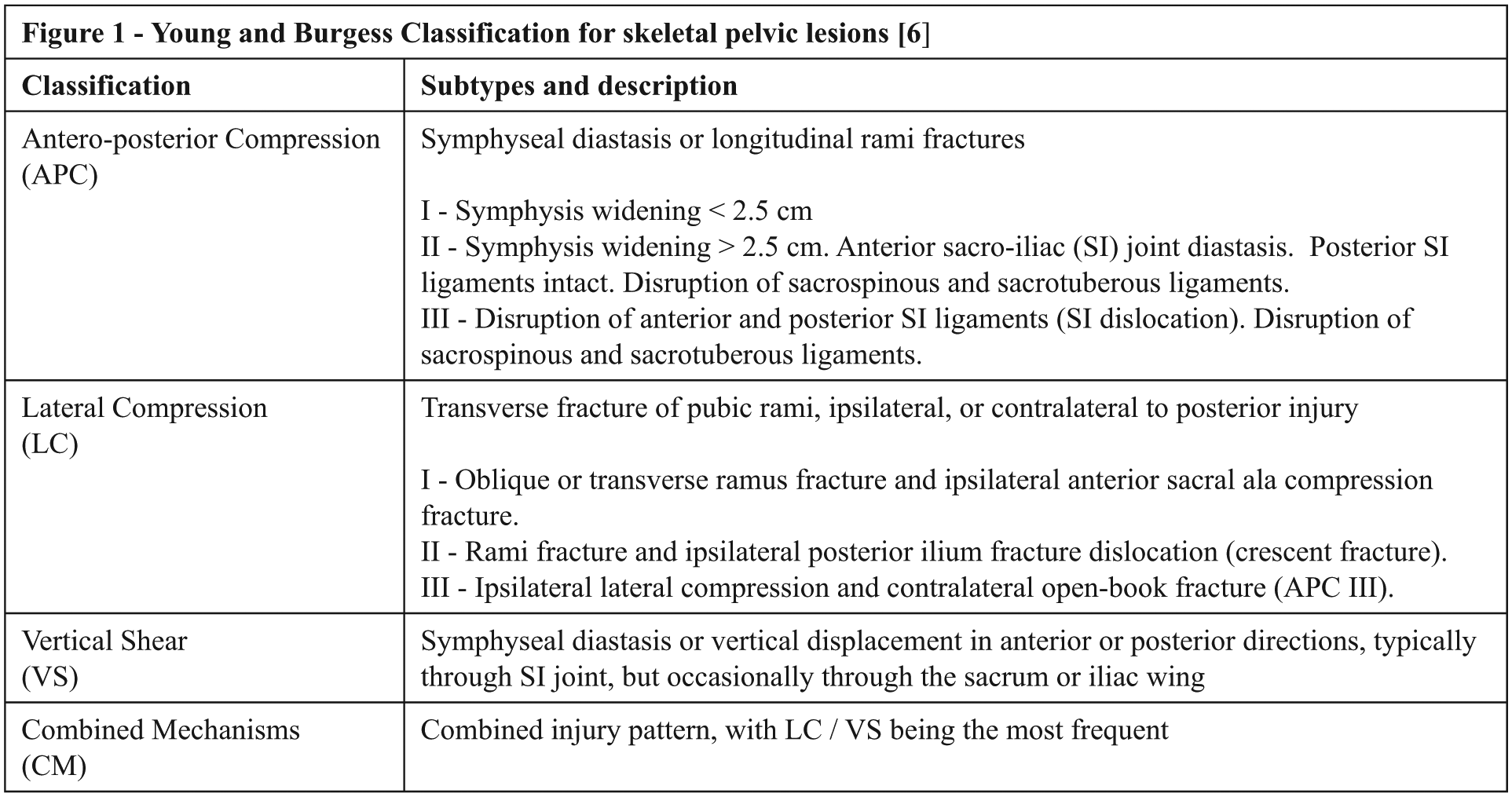
Young and Burgess classification for skeletal pelvic lesions. 6
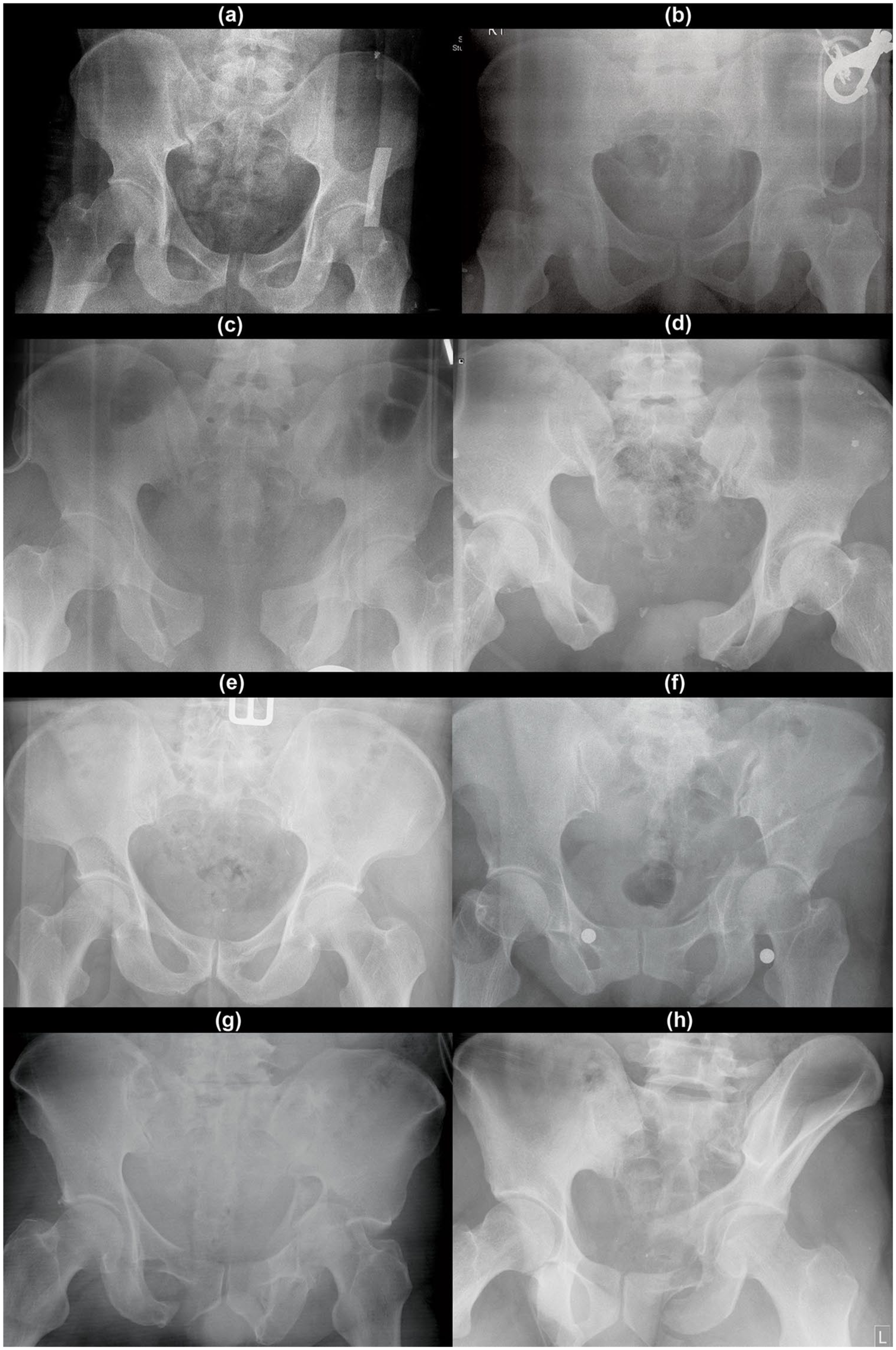
Typical radiographic appearances of each fracture type classified by the Young–Burgess system, 6 which were identified in our data set. (a), (b) Anteroposterior compression (APC) Type I; (a) showing the typical widened pubic symphysis appearance, (b) showing longitudinal ramus fracture, (c) APC II, (d) APC III, (e) lateral compression (LC) type I, (f) LC II, (g) LC III and (h) vertical shear (VS).
However, as computer tomography (CT) scans are becoming increasingly accessible, the role of pelvic radiograph in emergency trauma care is brought into questioning. Studies had shown that the sensitivity of pelvic radiograph was 50% to 60%, 14 , 15 with a high false negative rate up to 32%. 16 Kessel et al. 17 reported that pelvic radiograph has a low sensitivity (64.4%) when compared with CT angiogram, with multi-planar reconstructions of abdominopelvic CTA further identified 35.6% (n = 72) of fractures which were missed on the initial pelvic radiograph. Systematic reviews have also reported that pelvic radiographs alone does not predict mortality, haemorrhage or need for angiography. 18 However, both imaging modalities have different intrinsic roles in clinical management. Despite the inferior sensitivity when comparing with CT, plain radiographs provide an overview and can be easily performed at bedside. CT scans invariably require transporting the patient to the CT facility, and may take up a considerable amount of time. It is also extremely difficult to perform resuscitation within the CT suite. All of these constraints may compromise the patients’ condition.
There were previous studies assessing the inter-observer reliability in classifying pelvic ring fractures by pelvic radiographs and CT scans among trauma surgeons or orthopaedic surgeons using the Young–Burgess system, to varying results.9–11 On the other hand, inter-observer reliability in evaluating pelvic trauma in major trauma patients by the emergency physicians has not been studied before. While each specific type of pelvic ring fractures may warrant the trauma surgeons to employ different definitive operative strategies, pelvic radiographs allow emergency physicians to make important clinical decision, especially when the patient is unstable and unfit to undergo CT scans.
Objective
The first objective of this study was to determine the inter-observer agreement in the interpretation of pelvic radiograph between emergency physicians. The second objective was to determine the inter-method agreement between plain pelvic radiographs and CT scans, in classifying pelvic fractures.
Methods
Settings and participants
This is a retrospective, observational study. Patients were recruited from the data set obtained for the ‘Dynamic MTP score’ study 19 and secondary analysis of those patients with pelvic radiograph was performed. Polytrauma patients with injury severity score (ISS) ⩾ 9 and age > 12 years were recruited from the trauma registries of four designated trauma centres in Hong Kong (Tuen Mun Hospital of New Territories East Cluster, Princess Margaret Hospital of Kowloon West Cluster, Queen Elizabeth Hospital of Kowloon Central Cluster and Queen Mary Hospital from Hong Kong West Cluster), from 1 January 2005 to 31 December 2012. Patients with burn injury, drowning, chronic renal failure, known chronic anaemia (haemoglobin ⩽ 7 g/dL), or traumatic cardiac arrest were excluded. Patient with pelvic injuries having one set of positive pelvic radiograph and pelvic CT scan were identified and recruited for secondary analysis in this study.
Study design and data analysis
Inter-tester agreement
All pelvic radiographs were reviewed independently by two emergency physicians (Reviewer 1 and Reviewer 2) from two different institutions, both having more than 15 years working experience in the ED. Each emergency physician classified the pelvic radiographs using the Young–Burgess classification system. Fractures that were not being classified in the Young–Burgess system including isolated acetabular fractures, sacral fractures, fracture iliac wing were classified under ‘not classifiable (NC)’.
The inter-observer agreement on the three groups, (1) mechanism of injury, (2) stable versus unstable pelvic fracture and (3) complete Young–Burgess classifications, were analysed by Cohen’s kappa statistics. 20 The ‘mechanism of injury’ was defined by the four categories of mechanism of injury in Young–Burgess classification: 6 ‘anteroposterior compression’ (APC), ‘lateral compression’ (LC), ‘vertical shear’ (VS), ‘combined mechanism’ (CM), plus ‘not classifiable’ (NC), making up to five categories in this study (Figure 1). ‘Stable fractures’ were defined as APC I and LC I, plus NC in this study, with the rest (APC II, APC III, LC II, LC III, VS and CM) as ‘unstable fractures’.
Kappa values were classified according to the Landis and Koch’s method (< 0 = poor, 0.00–0.20 = slight, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = substantial, 0.81–1.00 = excellent). 21 The minimal number of subjects required to be included for the valid application of weighted kappa is approximated by 2k2. 22 Based on the number of categories in Young–Burgess classification plus one extra category of ‘not classifiable’, the minimal number of subject that must be included was 162. Descriptive statistics were used to summarise the results.
Inter-method agreement
For the inter-method reliability of the classification of pelvic fractures, an independent radiologist with more than 10 years of experience was invited to review all of the pelvic CT films of the patient identified with pelvic fractures. Pelvic fractures were classified under the Young–Burgess system in the same manner as plain radiographs. The CT findings were compared with the agreed pelvic radiograph diagnoses made by the emergency physicians. In the case of disagreement in the X-ray diagnoses, a senior emergency physician with a special interest and experience in polytrauma management was invited to make a decision upon the types of pelvic fracture.
The inter-method agreement by Cohen’s kappa were analysed on (1) mechanism of injury, (2) stable versus unstable pelvic fracture and (3) complete Young–Burgess classifications as the plain radiographs.
All reviewers were blinded to patient information including name, diagnosis, treatment and outcome. The reviewers worked independent of each other, and no time constraint was imposed.
Outcome
The primary outcome would be the inter-observer agreement for pelvic radiograph interpretation by the emergency physicians, and inter-method agreement between pelvic plain radiographs and CT scans.
Results
Our search within the trauma registries of the four participating hospital identified a total of 5151 patients fulfilling the inclusion criteria of (ISS) ⩾ 9 and age > 12 years within the study period. 86 patients were excluded with the exclusion criteria, 36 excluded for pre-hospital cardiac arrest and 38 excluded for missing crucial data. Of the 4991 patients included for analysis, 508 were identified with pelvic fractures. 92 patients were excluded due to poor radiographic quality or no pelvic radiograph performed. A further 47 patients were excluded as there were no pelvic CT scans performed, or CT scans were arranged only after operative management on the pelvis. Three hundred sixty-nine patients were eventually included in the study. The mean age was 45.2 ± 19.5 years, median 42 years (range: 12–90 years) and 210 (56.9%) were male. Of all the patients, six (1.4%) were put on pelvic binder before X-ray, a further 10 patients (2.6%) were put on pelvic binders before CT scan.
The distribution of the pelvic radiograph classification by the two reviewers, X-ray final decisions and classification by CT scans using the Young–Burgess system are summarised in Table 1. All fracture types were chosen at least once by each group. The most commonly picked mechanism of injury was LC (51.5% for Reviewer 1, 58.8% for Reviewer 2, 48.2% for X-ray final decisions, 58.5% for CT scans), followed by NC (35.2% for Reviewer 1, 31.4% for Reviewer 2, 31.9% for X-ray final decisions, 19.2% for CT scans). The least picked was CM (0.3% for Reviewer 1, 0.3% for Reviewer 2, 1.6% for X-ray final decisions, 3.3% for CT scans) and APC III (1.6% for Reviewer 1, 1.9% for Reviewer 2, 1.4% for X-ray final decisions, 0.8% for CT scans).
Distribution of pelvic fractures classified using the Young–Burgess system. 6
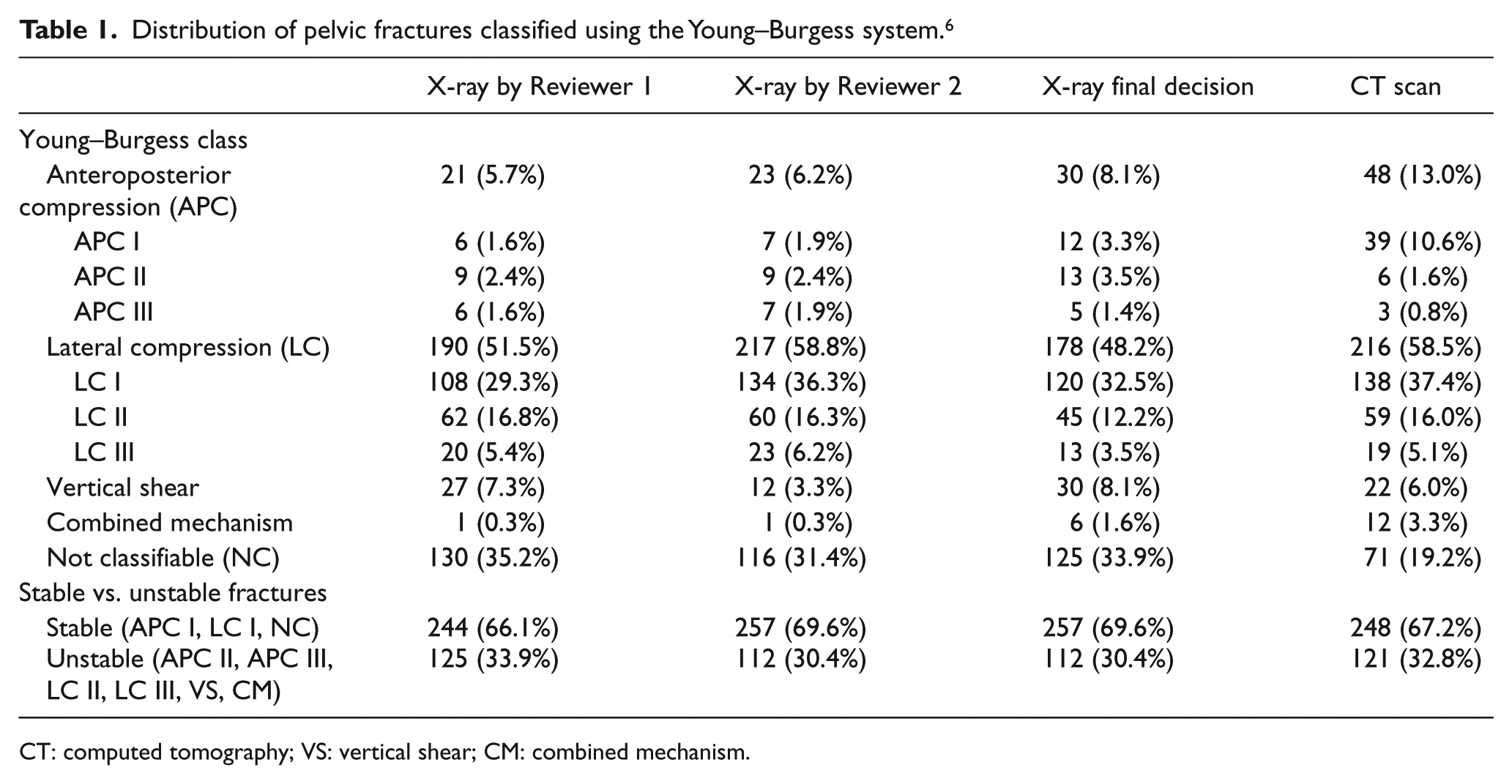
CT: computed tomography; VS: vertical shear; CM: combined mechanism.
The inter-observer agreements for pelvic radiographs interpreted by Reviewers 1 and 2 were substantial (κ = 0.72) for ‘the mechanism of injury’ (Table 2). Agreements for ‘stable versus unstable pelvic fractures’ and ‘complete agreement’ were moderate (κ = 0.60 and 0.56, respectively). The inter-method agreement between X-ray final decisions and CT scans was less satisfactory. The agreement for ‘stable versus unstable fractures’ was moderate (κ = 0.59), while the agreements for ‘mechanism of injury’ and ‘complete agreement’ were fair (κ = 0.42 and 0.38).
Inter-observer and inter-method agreement.
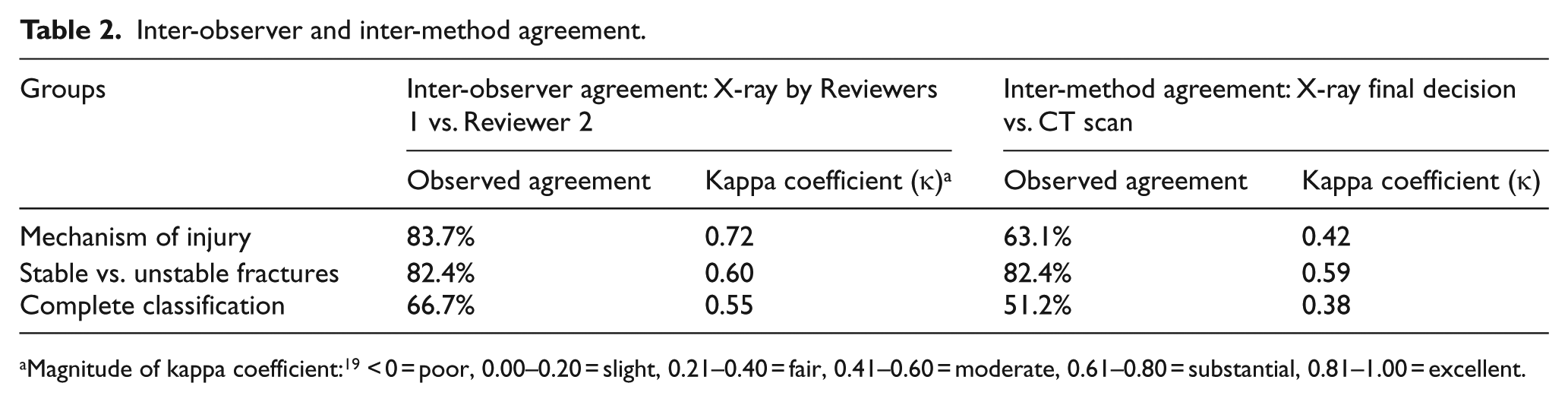
Magnitude of kappa coefficient: 19 < 0 = poor, 0.00–0.20 = slight, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = substantial, 0.81–1.00 = excellent.
Discussion
Our findings of the distribution of pelvic fracture types were compatible with the original series by Young and Burgess (APC = 15%, LC = 57%, VS = 6%, CM = 22%). 6 Our series only included AP films, which was compatible with the everyday clinical scenario in the ED. Young and Burgess devised the system using AP, inlet and outlet views, but stated that 94% of the diagnoses can be correctly made using plain AP pelvic radiographs alone. Subsequent studies that looked at the inter-observer agreement of plain radiographs found varying results.9–11 Gabbe et al. 10 evaluated the inter-observer agreement between three experienced orthopaedic surgeons interpreting pelvic radiographs in 100 patients using the Young–Burgess classification, and found the agreement was low, with kappa κ = 0.17–0.19 for ‘mechanism of injury’, κ = 0.17–0.21 for ‘stable versus unstable fractures’ and κ = 0.06–0.14 for complete agreement. Koo et al. 9 found that the inter-observer agreement improved with experience in the 30 pelvic radiographs they reviewed, with pelvic/acetabular surgeons achieving substantial agreement (κ = 0.85), substantial agreement with orthopaedic traumatologists (κ = 0.68) and moderate agreement (κ = 0.52) for senior trainees.
The plain radiographs agreements in all categories in this study were superior to that of Gabbe et al. The agreement was inferior to that between pelvic/acetabular surgeons and orthopaedic trauma surgeons with Koo et al., but compatible with the findings among senior trainees. The discrepancy could be explained partly by selection bias and the study design. Both Koo et al. and Gabbe et al. included only patients suffering from pelvic ring fractures, while our study included patients with fracture types other than the pelvic ring. All three views of plain radiographs (AP, inlet and outlet) were available to Koo et al., while no outlet view were available to Gabbe et al., and only AP view for our reviewers. Among the three studies, this study had the largest number of subjects, thus more likely to include a wider variety of pelvic fracture types, and a larger number of severe fracture types which have lower prevalence in trauma patients.
The agreement between plain radiographs and CT was fair to moderate. One of the most striking findings is the large number of films being classified as NC by plain radiographs. The rationale of including positive radiographs other than those with pelvic ring fractures was that, emergency physicians frequently assess films of a much larger population of stable and mildly injured patients, hence, we test the reliability between emergency physicians to pick out the more seriously injured among the less fatal ones. Both Reviewers 1 and 2 classified more than 30% of fractures as NC (35.2% by Reviewer 1% and 31.4% by Reviewer 2). The CT diagnosis shows a much smaller number of NC fractures (19.2%). Majority of the 62 fractures that was agreed by plain radiographs as NC were classified by CT as LC I (n = 33, 53.2%) and APC I (n = 16, 25.8%). Fractures in the sacral region were well known to be difficult in assessment by the AP pelvic radiographs, which could contribute to the under-detection of sacral fractures, in turns the under-classification of LC I fractures. On the other hand, as NC was not a group of fractures originally classified within the Young–Burgess system, it is not possible to attribute this difference only for misinterpretation or the relatively low sensitivity of X-ray. LC I and APC I encompass all of the stable ring fractures involving the pubic rami. 6 A search among existing literature and educational materials revealed that there were a number of publications 4,23–25 focused on the widening of pubic symphysis as the key differentiating feature of APC fractures, but may not have stressed that longitudinal fractures of pubic rami should also be included. Commonly found schematic diagrams of Young–Burgess classification also failed to illustrate pubic rami fractures in the APC group. It was thus possible that the under-recognition of LC I or APC I fractures could be a result of an inconsistency in existing educational materials or the training received by the reviewers. It was the author’s belief that the essence of Young–Burgess system, was the understanding of pelvic ring fractures based on the presumed mechanism of the injury by recognising the morphology of the fractures, rather than the exact fracture patterns identified, in order to guide further management.
Complete agreement was low for fractures that were agreed to be unstable. Of those 84 fractures agreed by both plain radiographs and CT scans as unstable fractures, only 34 were agreed on the Young–Burgess class (observed agreement = 40.5%). The most common disagreement were LC II and VS (n = 18, 52.9%). Both LC II and VS involved only one side of the pelvic ring, with a longitudinal fracture that might traverse through the posterior portion of the iliac wing or sometimes even the sacrum. It was most difficult to differentiate between LC II and VS when the displacement was less pronounced (Figure 3). Another difficult pattern was CM. CM was classified only in one patient by plain pelvic radiograph but in 12 patients by CT scans. The low agreement in diagnosing CM was most likely due to the fact that CM fractures were complex patterns that could not be pinned down by one mechanism of injury, making it the most difficult pattern to be recognised (Figure 4).
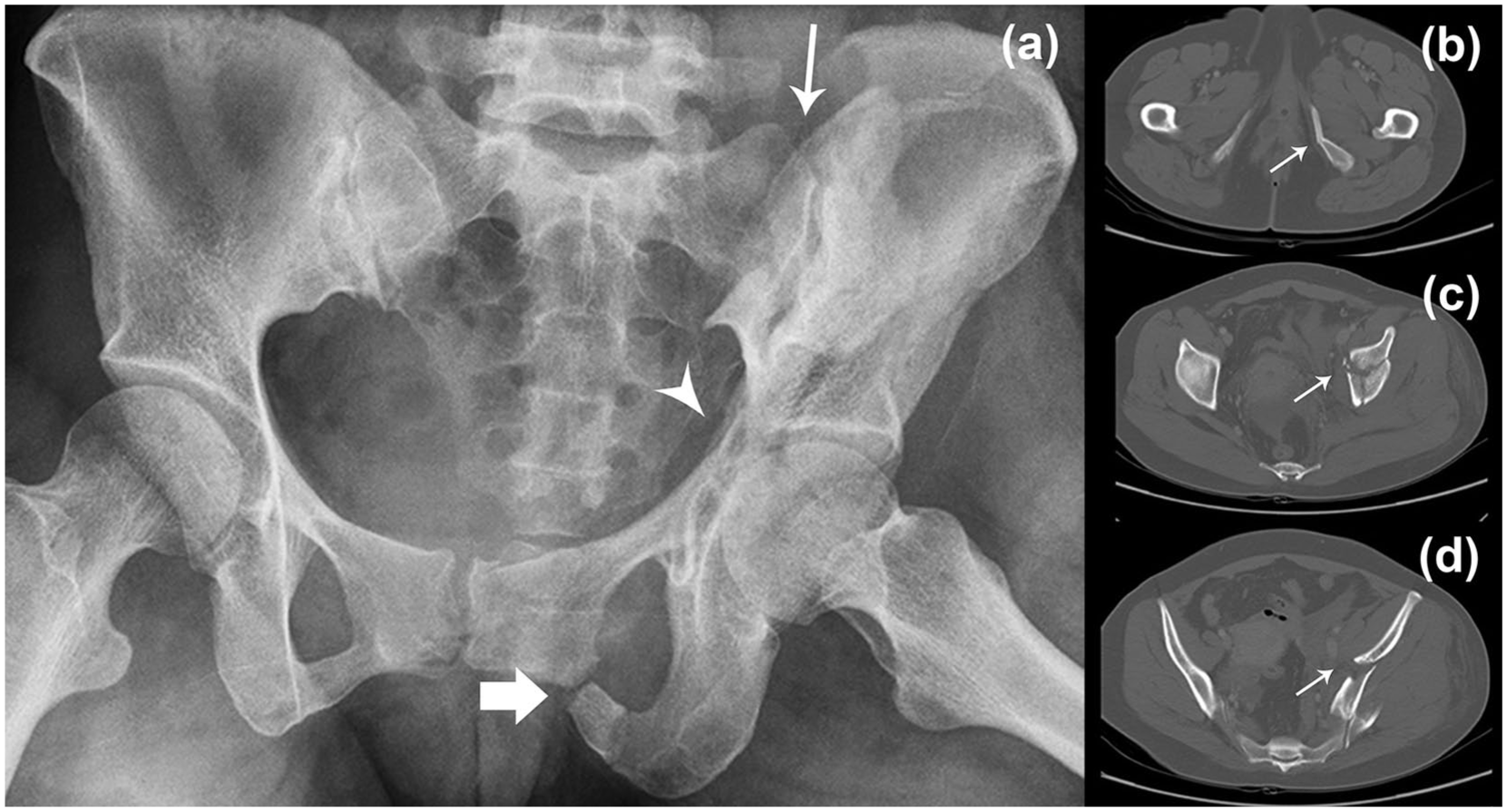
(a) Pelvic radiograph which Reviewers 1 and 2 and CT scan could not agree on whether it was a VS or LC II fracture. Fractures that could be delineated from this radiograph were fractured left superior and inferior pubic rami (broad arrow), fractured acetabulum (arrowhead) and linear fracture of the left iliac wing with sacroiliac joint disruption. Note that the fractured left hemipelvis did not show a pronounced vertical or AP displacement, which added to the difficulty in its classification and (b–d) showed selections from the CT scan of the same patient at pubic rami, acetabulum and iliac wing level respectively, with the thin arrow show corresponded fractures identified on the plain radiograph.
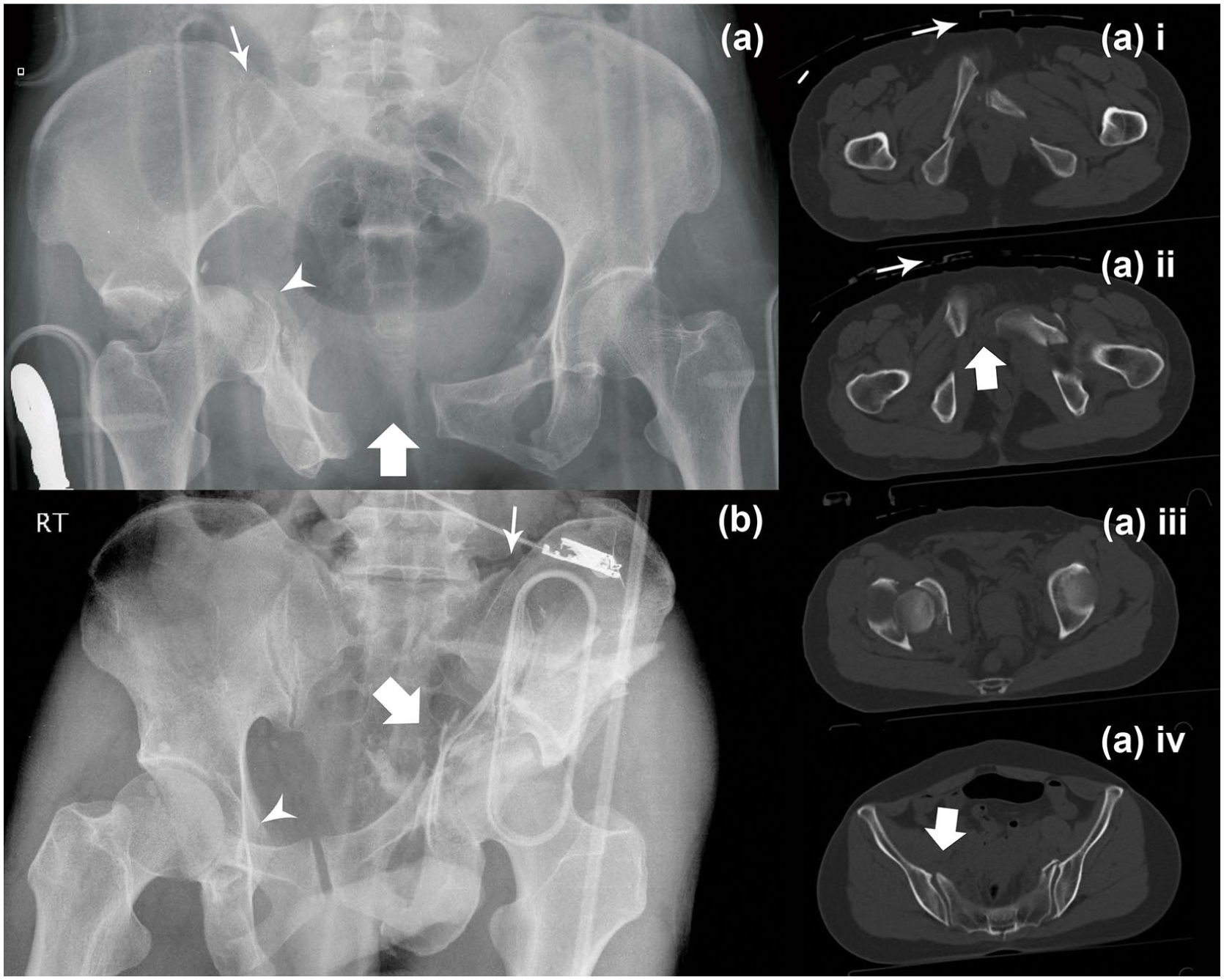
(a) Pelvic radiograph of a pelvic fracture, which the reviewers were able to agree on its classification as ‘combined mechanism’ (CM). Note the grossly widened symphysis (broad arrow) and right sacroiliac joint (SIJ; thin arrow), which was attributed by an anteroposterior compression (APC) force. Fractured right acetabulum was also identified (arrow head), which was attributed by a lateral compression (LC) force, making it a combined APC III and LC II fracture. (a) i, ii, iii, iv were selections of the CT scan of the same patient at different levels. Thin arrows on (a) i and ii showed a pelvic binder that was most likely placed on the patient after the radiograph was taken and before CT scan was performed. Note the widening of the symphysis (broad arrow, (a) ii) and right SIJ (broad arrow, (a) iv) was less pronounced than the pelvic radiograph and (b) showed a pelvic radiograph that the reviewers and CT scan failed to agree on whether it should be classified as a VS, LC III or CM fracture. This showed a complex fracture pattern with fractured right superior and inferior pubic ramus (arrow head), fractured left acetabulum (broad arrow) and fractured left iliac wing with left SIJ disruption (thin arrow).
Pelvic binders were placed in 6 patients before plain radiographs and 10 more before CT scans were obtained. The observed agreement for these plain radiographs were 33.3%. The agreement between plain radiographs and CT post-binder placement was 10%. There were two instances which APC II fractures were downgraded to APC I in CT scan after binder placement. Although it was well-known that pelvic binders would lead to under-recognition of unstable fracture patterns, future studies should include a larger sample with pelvic binders to study its effect on inter-observer reliability.
Limitations
A major limitation of this study is the small number of reviewers participating in the image interpretation, mainly as a result of limited resources available to the research team. A larger number of reviewers trained in different institutes may represent the general situation among emergency physicians. Employing only one radiologist to interpret the CT scans may also have led to significant single observer bias. During the conception of this study, it was postulated that CT scans interpreted by an experienced radiologist could be used as a ‘gold standard’ for plain radiographs. The responsible radiologist commented that a significant learning curve was required in order to be familiarised with the Young–Burgess system. Radiologists were trained to interpret images, but it was the orthopaedic or trauma surgeons’ expertise to categorise pelvic fractures to postulate treatment strategies. As a result, the inter-method agreement might be confounded by a component of intra-observer variability, and on top of that, a component of inter-observer variability as well, when the pelvic radiographs and CT scans were interpreted by different reviewers.
Selection bias in this study could be resulted from the fact that patients who died upon arriving at the ED or in traumatic cardiac arrest were excluded, as these patients could very possibly have severe pelvic fracture patterns, resulting in the low prevalence of unstable fracture types in our database. Another source of selection bias was that the subjects recruited in this study were obtained from the Dynamic MTP study data set, which excluded patients with chronic renal failure and chronic anaemia. Patients with negative radiographs were not included, and hence, the inter-observer agreement on negative images were not assessed.
Conclusion
The inter-method agreement between plain pelvic radiographs and CT scans was fair in classifying pelvic fractures, and moderate in detection of unstable pelvic fractures. Being an easily accessible and relatively low-cost investigation, if the patient is haemodynamically unstable or when CT is unavailable, plain pelvic radiograph can still be considered as a screening tool for unstable pelvic fractures to expedite early intervention. It is reasonable to forgo plain radiograph and go directly to pelvic CT if it is readily available. A review with the aim to improve the consistencies between educational materials, training or guidelines on the Young–Burgess classification may improve inter-observer agreements. Intra-observer agreement should also be tested in future studies.
Footnotes
Acknowledgements
We would like to acknowledge Dr Mina Cheng, Dr Chak Wah Kam, Dr Gilberto Leung and Dr Siu Man Li who worked on the original data set. The pelvic images reviewed in this article were retrieved from the archives of the Department of Radiology of Queen Mary Hospital, Queen Elizabeth Hospital, Tuen Mun Hospital, and Princess Margaret Hospital, Hong Kong.
Authors’ contributions
Dr J.C., Dr M.L.C.Y. and Dr O.F.W. designed and conceptualised the study. Dr J.C. and Dr M.Y. did literature search, statistical analysis and first draft of the manuscript for intellectual content. Dr M.C. assisted in literature search and statistical analysis. Dr O.F.W., Dr C.T.L. and Dr K.L.T were responsible for evaluation of the plain radiographs, ethical approval and acquisition of the original data set and revision of the manuscript for intellectual content. Dr C.K.K.W. were responsible for the interpretation of the CT scans.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data
The data sets generated and/or analysed during the current study are available. It has been uploaded during the submission process.
Informed consent
Written informed consent was not necessary as no patient data were included in this study.
Ethical approval
Ethical approval was not sought for the present study because this is a subgroup analysis of previously published data. Ethical approval was obtained from the ethical review board of the four trauma centres for the prior data set (approval reference: KC/KE-13-0243/ER-1, KW/EX-14-089(75-01), UW 15-550, NTWC/CREC/1161/13). This study was completed in accordance with the Helsinki Declaration.
Human rights
Human rights are protected. Patient particulars that may lead to the identification of an individual were excluded in the data analysis as well as publication of the findings.