
Abstract
A 44-year-old healthy man presented to the emergency department with left hip pain for a week. The physical exam did not point to a specific disease and his serum inflammatory markers were all increased. Point-of-care ultrasound was performed to help guide the management. The patient was able to receive definitive operation in a day.
Case report
A 44-year-old man presented to the emergency department (ED) with left hip pain for 1 week. He was a firefighter on anti-hypertensive but otherwise healthy. The hip pain was vague at first, without causing much trouble to his daily duties, but over the week had increased in severity, despite the patient taking some analgesics from his general practitioner (GP). The pain became persistent while at rest, exacerbated by hip movements and eventually made weight bearing difficult. There was no history of injury and the patient denied any constitutional symptoms, respiratory or gastrointestinal symptoms, neurological deficits or intravenous drug use.
On examination, the patient was afebrile and hemodynamically stable. He walked into the consultation room with antalgic gait, and had difficulty moving himself onto the examination couch. There were no overlying skin changes but the left hip was most tender anteriorly, and was irritable especially when internally rotated. The passive range of motion, albeit tender, was grossly preserved. Examinations of the respiratory and cardiovascular systems, the abdomen, sacroiliac joints (SIJ), spine and knees were unremarkable. Both the lower limbs had normal power and sensation.
The emergency physician (EP) decided to proceed to a focused point-of-care ultrasound (POCUS) examination (Figure 1). It was performed with a curved probe, using an anterior approach with longitudinal alignment to the femur.
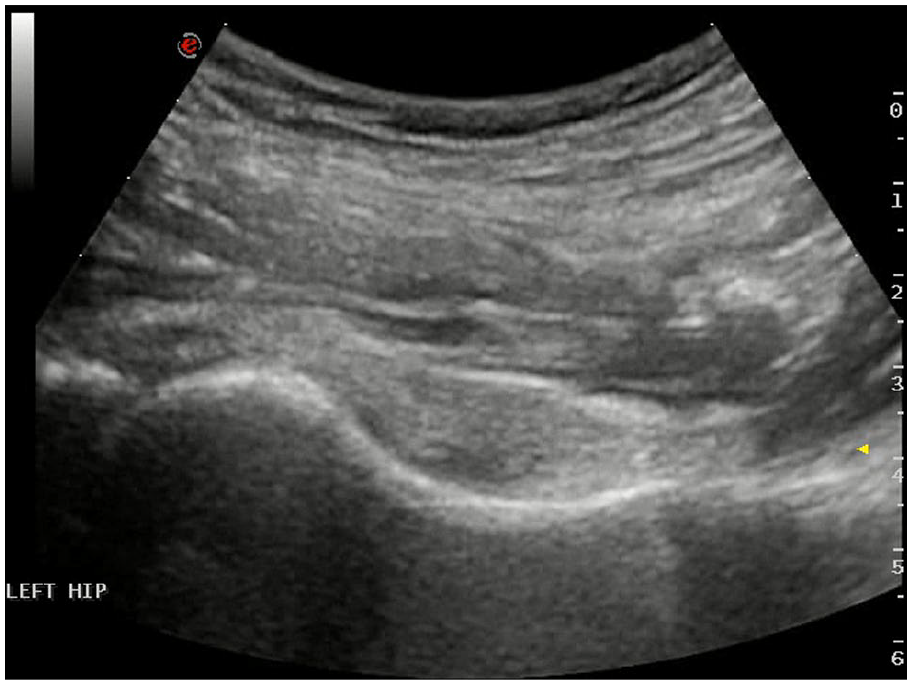
Ultrasound image of the left hip.
Questions:
Please describe the POCUS findings.
What are the differential diagnoses and which of them is the most concerning?
What ED procedure may help in steering the management?
Answers:
The left hip synovium was significantly thickened (Figure 2) when compared with the right (Figure 3), with a small amount of joint effusion (Figure 2), only visible from the anterior approach with internal rotation of the hip. Colour Doppler mode showed increased signal within the synovium, suggesting increased vascularity from inflammation.
The POCUS image is compatible with arthritis or synovitis of any inflammatory or infective nature. Septic arthritis is of singular importance that EPs should have in mind.
With the provisional diagnosis of septic arthritis in mind, the EP also quickly screened the abdomen and the left psoas muscle for any associated collection, which was not seen. As the hip effusion was only a small amount, the EP did not attempt to aspirate it in the ED. Nonetheless, in cases where effusion is of a larger volume, a bedside arthrocentesis, preferably with ultrasound guidance, can be diagnostic and even therapeutic.

Left: original POCUS image; right: annotated image. Note the thick synovium leading to the bulging, convex contour of joint capsule. Only trace amount of hypoechoic effusion is visible from the anterior approach.
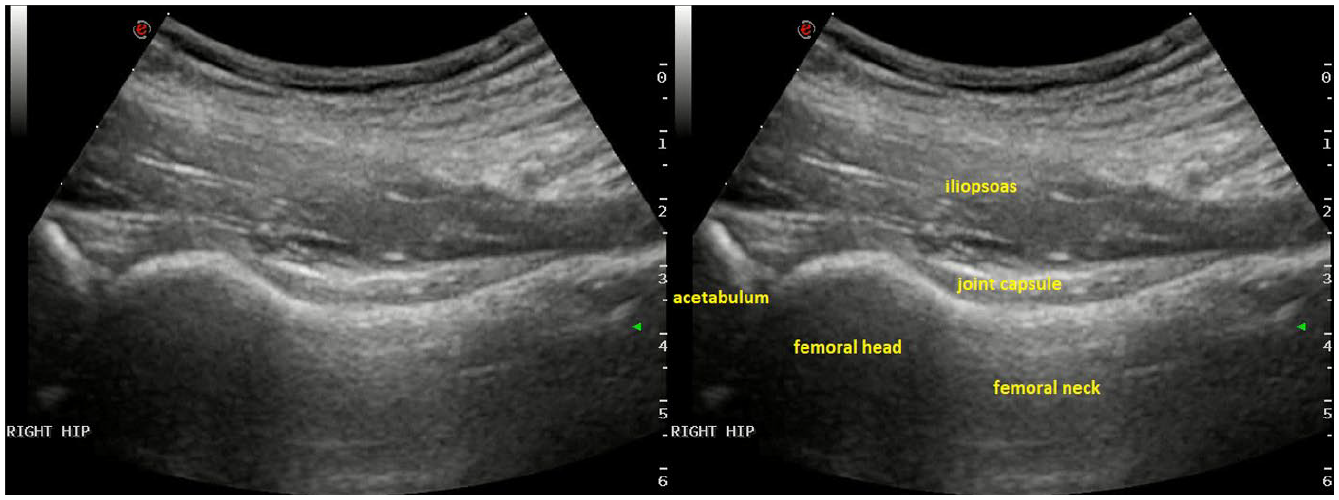
Left: POCUS image of the unaffected side; right: annotated image. Note the convex contour and homogeneity of the joint capsule.
The patient’s white blood cell (WBC), C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were all moderately raised. The x-ray showed contained, smooth spherical femoral heads with no fractures. He was admitted to the orthopaedic ward.
The orthopaedic team agreed that the physical and POCUS findings were compatible with an early septic arthritis, thus they ordered a contrast tomography, which confirmed the effusion and synovial thickening, as well as ruling out any intra-abdominal, SIJ or spinal pathologies. Antibiotics were started and the patient underwent an arthroscopic washout of the left hip the next day. Operative findings include turbid joint fluid and inflamed joint capsule. Analysis of the joint fluid revealed a moderate number of WBC; Gram stain and culture were negative. His antibiotics regime was adjusted by the infectious disease team. Further microbiological workup, including for mycobacterium and human immunodeficiency virus (HIV), was unrevealing.
After the operation and antibiotic therapy, the patient’s WBC, CRP and ESR quickly dropped back to normal range in a few days. He was able to walk unaided as the pain improved, and was able to be discharged with oral antibiotics around 2 weeks post-operatively.
Discussion
Septic arthritis is often difficult to diagnose by symptomology and physical signs alone. 1 It is not uncommon that even arthrocentesis, the gold standard, fails to identify the culprit organism. 2 This disease typically occurs in patients with multiple comorbidities or other risk factors, such as extreme age, diabetes or immunocompromised states. However, it can also affect younger and healthier populations. If its diagnosis or treatment is delayed, septic arthritis can lead to substantial complications, either local, affecting the joint function, or systemic, which could be life threatening.3,4 As more EPs become competent in POCUS, it is now easier to assess a hip joint in more detail, especially for effusion, which by ordinary physical examination alone would be tricky in such a deep structure. However, as exemplified by this case, it is important to keep in mind that effusion, although most well known, is not the only POCUS finding of septic arthritis, 2 and that the manoeuvre of passive internal rotation of the hip may increase the sensitivity of detection of effusion, especially if the amount is small that can pool to the posterior of the joint when the capsule is lax. If the effusion is of a significant volume, ultrasound guided aspiration by an experienced EP is a reasonable option. 5 Yet, if the patient’s presentation is less typical, further investigations including more advanced imaging are key to guiding the management.
Footnotes
Author contribution
All the authors contributed equally to this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Human rights
The data and images were obtained in accordance with the principles outlined in the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.