
Abstract
Introduction:
Transorbital low-velocity penetrating head injuries are uncommon but important. Minor skin wounds may herald intracranial injury with high morbidity and mortality.
Case presentation:
A fencing coach was pierced by a sabre between his nose and right eye resulting in orbital roof fracture and frontal lobe laceration. With prompt recognition of these injuries under multidisciplinary management, he attained uncomplicated recovery.
Conclusion:
The emergency physician should maintain a high index of suspicion for intracranial injury in patients presenting with history of penetrating head injury. Understanding orbital anatomy, injury mechanisms and patterns can facilitate timely management to prevent potentially sight-threatening and life-threatening complications.
Introduction
Penetrating head injury is a rare condition with incidence of 0.4% 1 in all head injuries. Transorbital penetrating injuries constitute up to 24% of penetrating head injuries in adults and 45% in children. 2 These injuries carry high mortality and morbidity. The extent of damage is related to the anatomy of the orbit, mechanism of injury, characteristics and trajectory of the penetrating foreign body. Complications include injury to visual pathway, neurovascular structures, vascular disruption and infection. In this article, we present an unusual case of penetrating cranio-orbital injury and discuss its clinical features, diagnosis and management.
Case report
A 36-year-old fencing coach was injured by a sabre that penetrated between his nose and right eye. A mask was not worn at the time. Along with a crackling sound, he believed that the penetrating depth was 1.5 cm. He complained of headache, nausea, right eye pain and blurring of vision.
On examination, he possessed full Glasgow Coma Score, orientation, stable vital signs and intact neurology. Inspection of his right eye showed periorbital ecchymosis with chemosis, mechanical ptosis, downwards dystopia and proptosis. There was a 1 cm oblique linear laceration below the right medial lower eyelid without margin involvement (Figure 1(a)). Extraocular eye movement was full with no diplopia. Pupils were equal and reactive to light with no relative afferent pupillary defect. Visual acuity (VA) was 0.7 on his right and 1.0 on his left. Anterior chamber was clear with no hyphema. Fluorescein stain test of the right eye was negative.
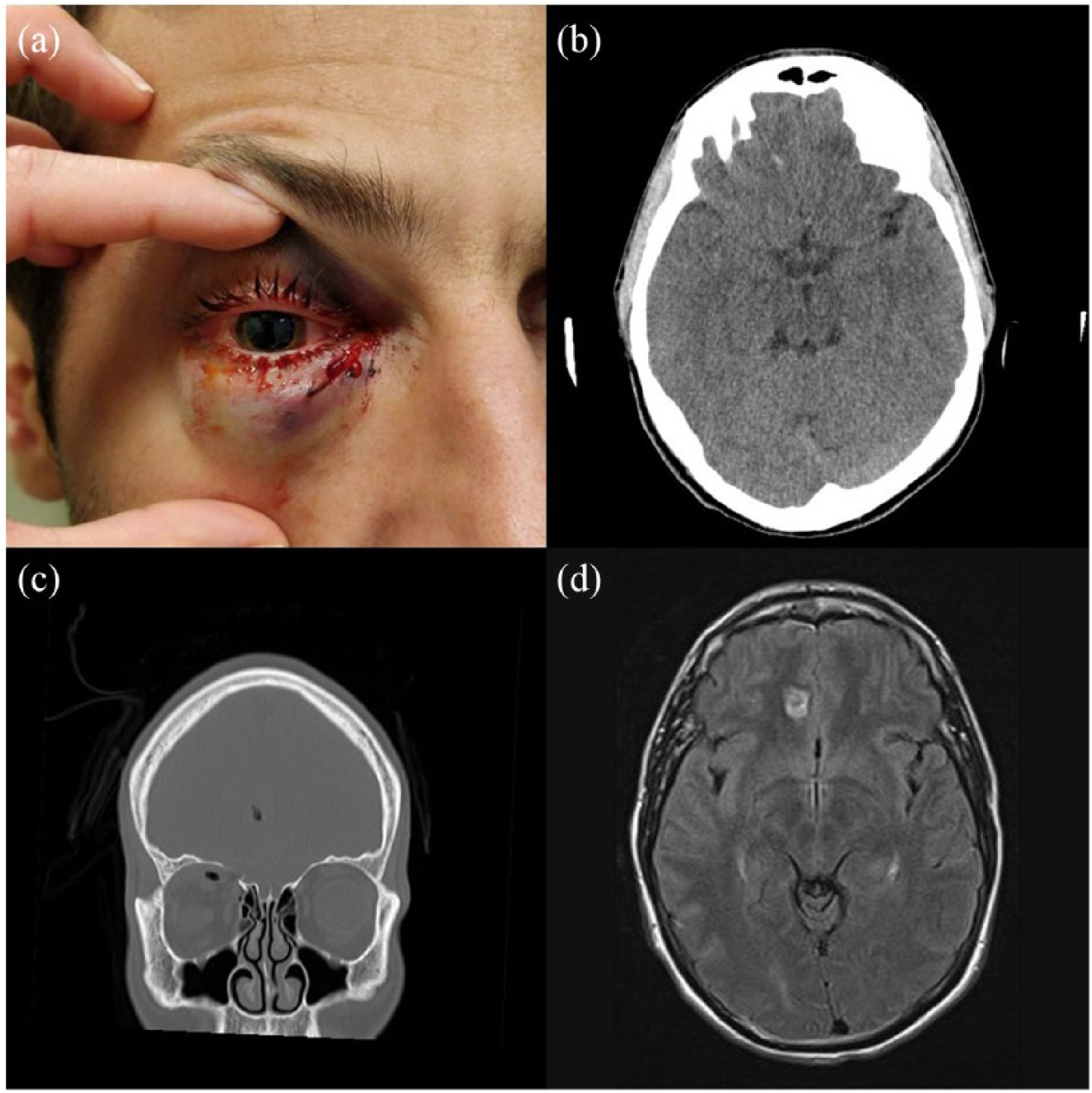
(a) Photograph depicting patient’s right eye with periorbital ecchymosis and oblique linear laceration at the medial lower eyelid. Pupil was dilated for fundoscopy. (b) Axial CT scan showing linear track of hyperdensity extending towards right medial inferior frontal lobe. (c) Coronal CT scan showing intact globe, proptosis, retrobulbar haematoma and orbital roof fracture with pneumo-oculi and pneumocephali. (d) Coronal FLAIR sequence MRI showing cerebral laceration reaching right cingulate gyrus.
Computed tomography (CT) scan of the orbit showed fracture of the right medio-superior orbital wall with pneumo-oculi and a hypoglobic and proptotic intact globe due to the presence of superior extraconal retrobulbar haemorrhage. CT brain showed a linear track of pneumocephalus and hyperdensity of blood from the orbit extending intracranially to the right medial inferior frontal lobe (Figure 1(b) and (c)).
An ophthalmologist was consulted, and globe injury was ruled out. There was no optic disc swelling, vitreous haemorrhage, retinal detachment or commotio retinae. Intraocular pressure (IOP) of the right eye was 22 mmHg by non-contact tonometry. Nose blowing and sneezing were advised against. The patient was started on timolol 0.5% eye drops and a meningitic dose of prophylactic ceftriaxone. He was then transferred to the neurosurgical unit.
Magnetic resonance imaging (MRI) brain confirmed the diagnosis of penetrating injury traversing the right orbital roof into the right medial frontal lobe with cerebral laceration involving the right medial frontal gyrus and reaching the right cingulate sulcus. There was no retained foreign body (Figure 1(d)).
After admission, his right eye supraduction and abduction were noted to be limited, and right IOP had increased to 35 mmHg. The laceration was repaired, and anti-glaucoma and antibiotic eye drops were prescribed. Subsequently, his extraocular movement improved and right IOP came under control. CT brain on day 9 showed reduced soft tissue swelling with no pneumocephalus. There were no neurological symptoms or signs throughout. He completed a 10-day course of ceftriaxone and was discharged with topical eye drops.
At 2 weeks follow-up, he complained of no pain or diplopia. His wound and bruising had healed. His right eye VA was 0.8 and IOP was 9 mmHg. The case was closed as he returned to his home country.
Discussion
In the present day, penetrating head injuries in the civilian population by fencing rods are almost unheard of. In a study of sports injuries in elite fencers training at the Korea National Training Centre between 2008 and 2015, 3 only 5% of injuries occurred in the ‘head and neck region’ with none involving the head and face as compared to the lower extremity (47.2%), upper extremity (26.4%) and trunk (21.4%). Injury rate was significantly higher in males than in female fencers; and higher in sabre than in epee or foil. A study of the 2008 Olympic Games demonstrated the incidence of injury in fencing to be as low as 2.5% when compared to over 30% for soccer. 4
Here, we report a rare case of penetrating cranio-orbital injury. Due to the unique anatomy of the pyramidal orbit, penetrating foreign bodies can reach intracranial contents via the five natural openings even in the absence of bony orbit fracture or globe injury 5 (Figure 2(a)).
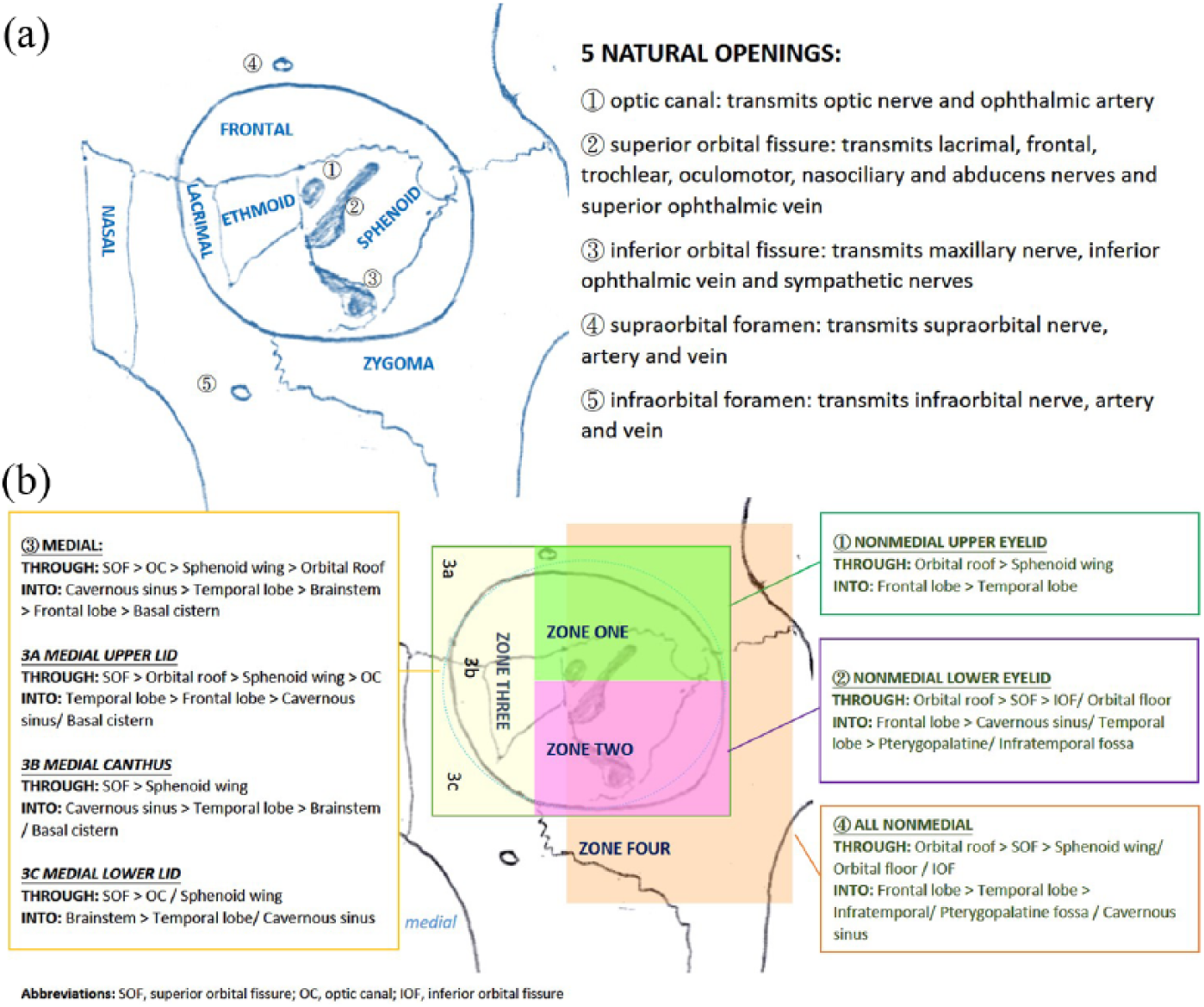
(a) Anatomy of the orbit. (b) Common pattern of injury according to the site of foreign body penetration.
As in our case, the most frequent route of entry of penetrating foreign bodies is via the orbital roof. 2 The superior orbital plate of the frontal bone is relatively fragile and becomes exposed when patients reflexively extend their heads backwards. This is followed by the superior orbital fissure and optic canal as foreign bodies are directed by the bony anatomy to the natural openings which offer least resistance.
Mechanism and patterns of injury
Based on history and physical examination, the clinician may predict specific structures affected. First, the injury sustained by our patient, in which the orbital roof and medial frontal lobe were traversed, is classified as low-velocity injury (non-missile, <100 m/s). Low-velocity penetrations are directed by the bony orbit to exit from anatomical fissures to reach the carotid artery, cavernous sinus, suprasellar cistern, temporal lobe and brainstem. They tend to occur in young men in cases of aggression, self-harm and accidents. 6 These carry better prognosis as laceration and maceration tend to result in localised haemorrhage. On the contrary, high-velocity injuries such as explosions and gunshots commonly result in more significant bony fracture. 7
Second, the site of entry may be used to deduce the intracranial structures affected. Turbin et al. 2 proposed a classification system to predict specific patterns of injury according to the site of eyelid entry (Figure 2(b)). Consistent with our case, a medial site of entry (zone 3) results in frontal lobe injury.
Imaging
Clinical presentation of penetrating cranio-orbital injury may be dramatic, especially in the case of a protruding foreign body. However, patients may present with a seemingly simple periorbital laceration. Our patient presented with nothing more than an innocuous eyelid laceration. In some cases, a retained foreign body may present as epilepsy or headache even years after the initial event. 8 Early recognition of occult intracranial injury is pivotal to provide prompt treatment.
The role of imaging is to delineate the size and shape of the penetrating object, its trajectory, the extent of damage and its anatomical relationship with surrounding structures.
Plain X-ray may have limited use in detecting skull fractures and metallic foreign bodies, but it cannot provide further information on intracranial structures.
CT is the first-line investigation to be performed. However, CT can miss up to 40% of abscesses and 42% of foreign body initially. 2 Detection of wooden fragments is particularly challenging as its density is close to intracranial or orbital air and soft tissues. 9 Dedicated bone windows, repeated imaging or image review may be needed.
MRI is more sensitive in detection of organic foreign bodies but cannot be used if a metallic foreign body is suspected. Its use is also limited in emergency cases and unstable patients.
Imaging of cerebral vessels is indicated in case of suspected vascular injury. Indications for an early angiographic evaluation include fracture of the greater wing of the sphenoid and cranial nerve deficit, both of which suggest possible injury to the middle cranial fossa or the cavernous sinus. 10 This may be in the form of CT or MR angiography.
A contrast MRI brain with diffusion-weighted imaging (DWI) was performed for our patient on Day 2 of admission to delineate the trajectory of penetration with relation to intracranial anatomy. It allowed better evaluation of periorbital soft tissue injury, specifically retro-orbital haematoma and thickening of the extraocular muscles. It also ruled out injury to the bilateral internal carotid, vertebral and basilar arteries and proximal portions of major cerebral arteries.
Management and complications
Initial management should follow advanced trauma life support (ATLS) principles of primary survey and resuscitation. A multidisciplinary approach should be adopted.
Infectious complications are common, in the form of meningitis in 64%–70% of cases and brain abscess in 48%–52% of cases. Anti-tetanic serum is required in all cases. Aggressive parental broad-spectrum antibiotics covering Staphylococcus, Bacillus and Clostridium that cross the blood–brain barrier are recommended. 10
Symptomatic epilepsy occurs in 30%–50% of patients with penetrating skull and brain injuries. Administration of anticonvulsants is indicated during the first week after traumatic brain injury, while prophylactic administration of anticonvulsants during the later period is not justified. 11
If a retained foreign body is suspected or confirmed, early surgical exploration by a multidisciplinary team is essential. Oral maxillofacial surgery, neurosurgery, ophthalmology and neuro-anaesthesiology should be involved. Removal of the foreign body under direct visualisation is recommended, followed by closure or repair of the subsequent defect.
Orbital compartment syndrome should be suspected in patients who complain of sudden decrease in VA with pain, proptosis, relative afferent pupillary defect and ophthalmoparesis. 12 The emergency physician should be prepared to perform emergency lateral canthotomy and/or cantholysis at the bedside for patients with IOP > 40 mmHg and relative afferent pupillary defect except in cases of suspected globe rupture.
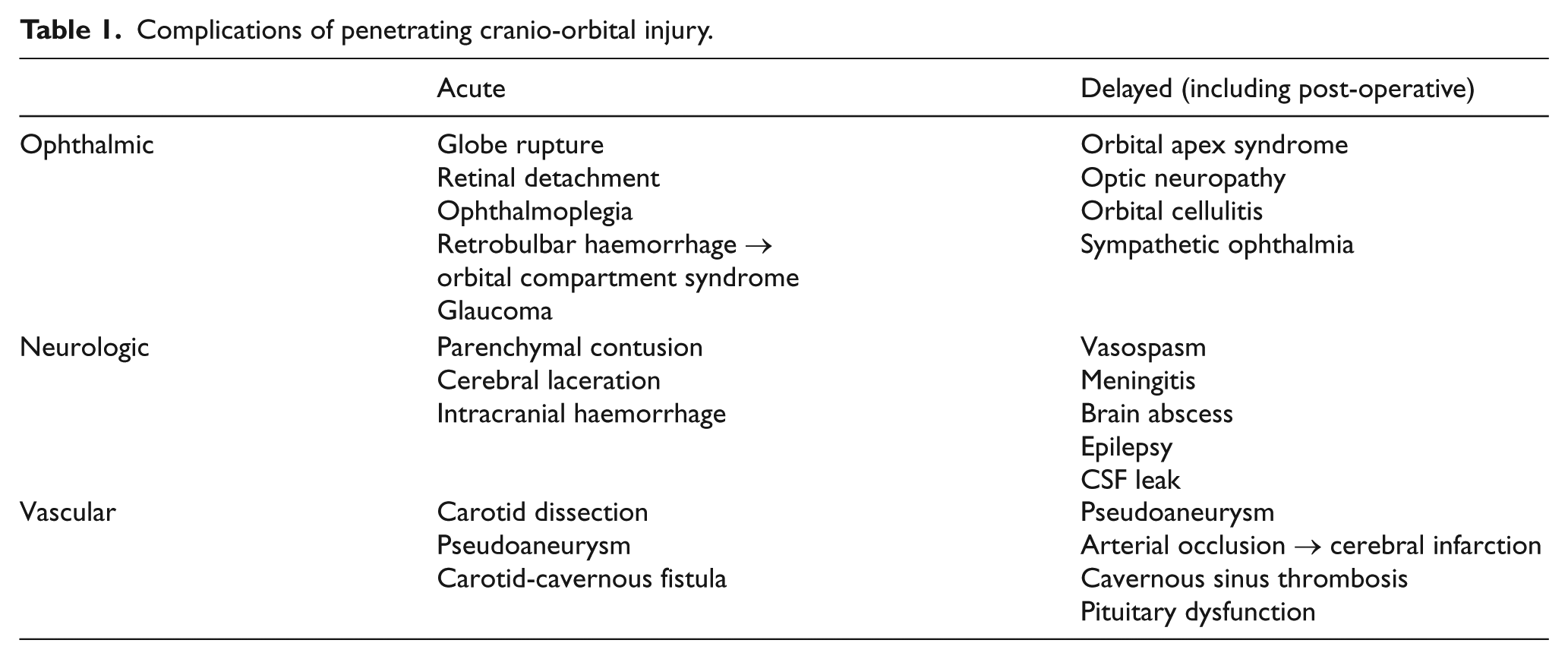
It is important to re-evaluate the patient for clinical recovery and development of complications (Table 1). One study recommended performing CT angiography 2–3 weeks after injury. 13
Complications of penetrating cranio-orbital injury.
Prognosis
Penetrating cerebral trauma carries good prognosis if immediate appropriate care is provided and the patient survives past the first week. In a large case review of penetrating cerebral trauma from the Vietnam conflict, only 8% of patients who survived past the first week since injury died. Of those deaths after the first week, one-third occurred in the first 3 months since injury. 13
As a result of prompt recognition of cranio-orbital injury and appropriate multidisciplinary management, our patient achieved full recovery. At 2 weeks from discharge, he had no neurological deficit or visual disturbance.
Conclusion
Penetrating cranio-orbital injuries are rare but should not be missed. Patients may present with seemingly trivial wound and intact neurology. The emergency physician should maintain a high index of suspicion for intracranial injury. Expedient imaging and multidisciplinary consultation can facilitate timely management.
To our knowledge, this is the first report of a penetrating brain injury caused by such an object in Hong Kong. Fortunately, our patient sustained minimal injury which did not result in long-term sequalae. This case illustrates the importance of collaboration of different specialties in management of penetrating cranial-orbital injury. With timely assessment by ophthalmologists and neurosurgeons, complications that required immediate management were ruled out and the patient received adequate observation and management.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.