
Abstract
Background:
Stonefish sting injury is one of the common marine stings in Hong Kong. It is commonly sustained during maritime activities, and it could be regarded as occupational hazard for chefs or domestic hazard for family. Its envenomation could lead to significant local symptoms (pain or swelling) and serious complications, including infection and compartment syndrome.
Objectives:
This study is to review its clinical presentation and various treatment modalities.
Methodology and study design:
Reported cases of stonefish stings to Hong Kong Poison Information Centre from October 2008 to October 2018 were included in the study. The cases were retrieved from the Hong Kong Poison Information Centre electronic database. Information on patient demographic data, clinical parameters (e.g. the site of injury, presenting symptoms), and various treatment modalities (e.g. analgesics, hot water immersion, and use of antivenom) was collected.
Results:
There were 32 eligible patients included in this case series. All of them sustained the injury over either their fingers or hands. All patients reported pain over the site of injury. Other reported symptoms included numbness (41%), swelling (81%), and redness (47%). Twenty-five patients (78%) had radiograph done, and one of them was noted to have foreign body retained at the site of envenomation. All patients received hot water immersion to the affected part at 40°C–45°C for at least 30 min. Altogether eight patients (25%) received stonefish antivenom for pain relief. One patient developed compartment syndrome and received emergency operation of fasciotomy of right hand and forearm.
Conclusion:
Stonefish envenomation can cause extreme pain, swelling, and erythema, which can be managed with hot water immersion, analgesics, and prophylactic antibiotics. Use of antivenom can be considered in selected case.
Introduction
Stonefish sting injury is one of the common marine stings in Hong Kong. It is commonly sustained during maritime activities, and it could be regarded as occupational hazard for chefs or domestic hazard for family. Its envenomation could lead to significant local symptoms (pain or swelling) and serious complications, including infection and compartment syndrome. This case series would help to review the clinical presentation and management modalities, including analgesics, hot water immersion, and use of antivenom, for patients with stonefish injury.
Methodology and study design
Reported cases of stonefish stings to Hong Kong Poison Information Centre (HKPIC) from October 2008 to October 2018 were included in the study. The cases were retrieved from the HKPIC electronic database, namely, “DATOX,” with the coding of “bite/sting/envenomation” and “Stonefish.” Information on patient demographic data, clinical parameters (e.g. the site of injury, presenting symptoms), and various treatment modalities (e.g. analgesics, hot water immersion, and use of antivenom) was collected. Patients aged 18 or above who sustained stonefish sting injury in the above specified period would be included in the study.
Results
There were 32 eligible patients included in this case series. The median age of patients was 52 (range = 22–67) years. Twenty-six patients (81%) were male. Table 1 reveals the demographics of our patients who sustained stonefish injury. All of them sustained the injury over either their hands or fingers, but not other body part. All patients reported pain over the site of injury. Other reported symptoms included numbness (41%), swelling (81%), and redness (47%). The majority of our patients sustained one puncture wound over their hands or fingers. Two patients sustained more than one puncture wound: one had four puncture wound over his hand, whereas the other patient had two puncture wound over her finger. Work-related stonefish injury accounted for 56% of our cases.
Patient demographics.
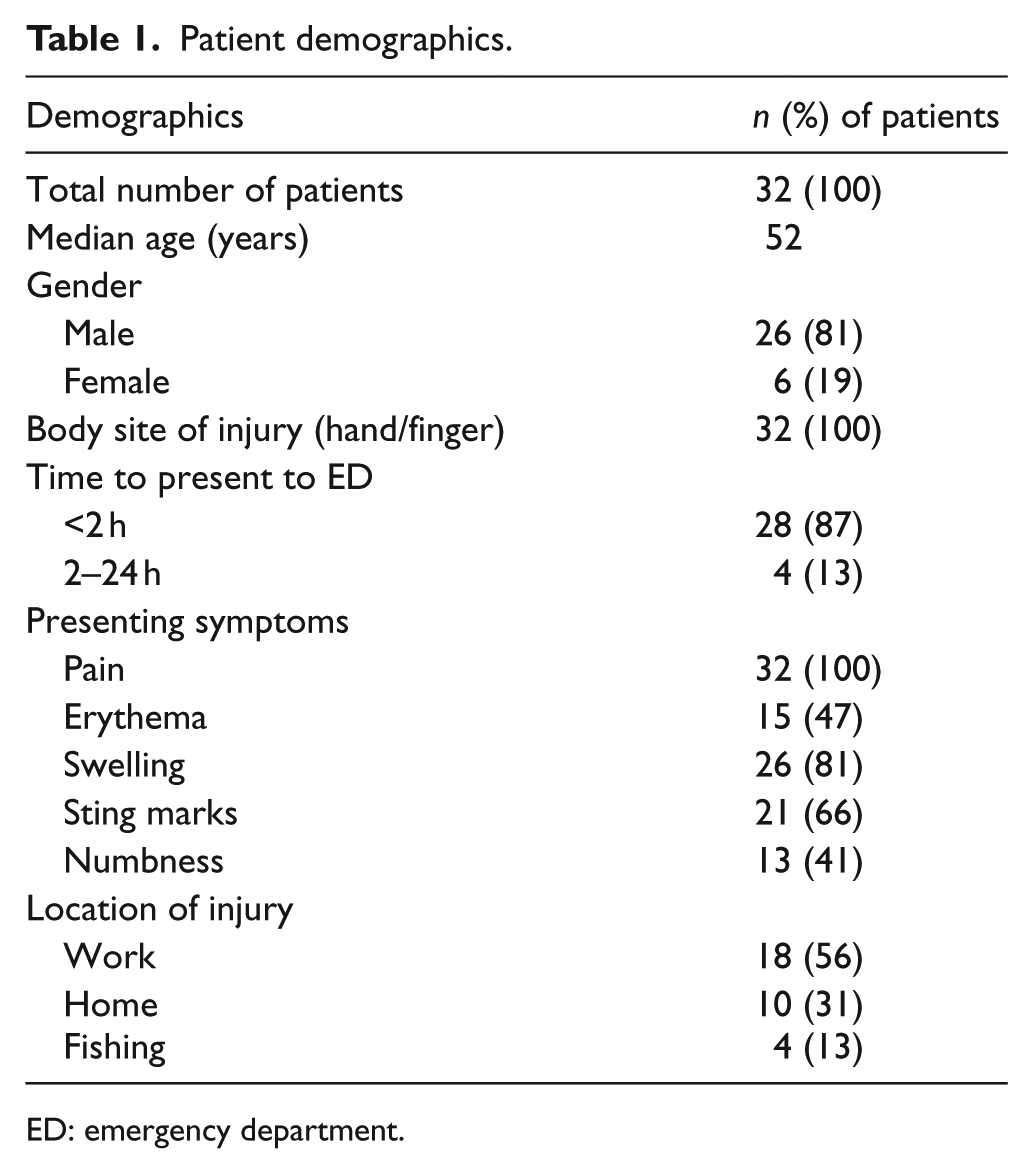
ED: emergency department.
Table 2 describes the management of stonefish injury in the emergency department (ED). Twenty-five patients (78%) had radiograph done. One of them was noted to have foreign body retained at the site of envenomation. Wound exploration was performed, and the foreign body was then successfully removed. All patients received hot water immersion of the affected part (hand or fingers) at 40°C–45°C for at least 30 min for pain relief. Twenty patients (63%) received analgesics in the ED as shown in Table 3. Intramuscular tramadol or ketorolac was commonly used in the ED for pain relief. One patient was given intravenous fentanyl for pain control.
Management in ED.
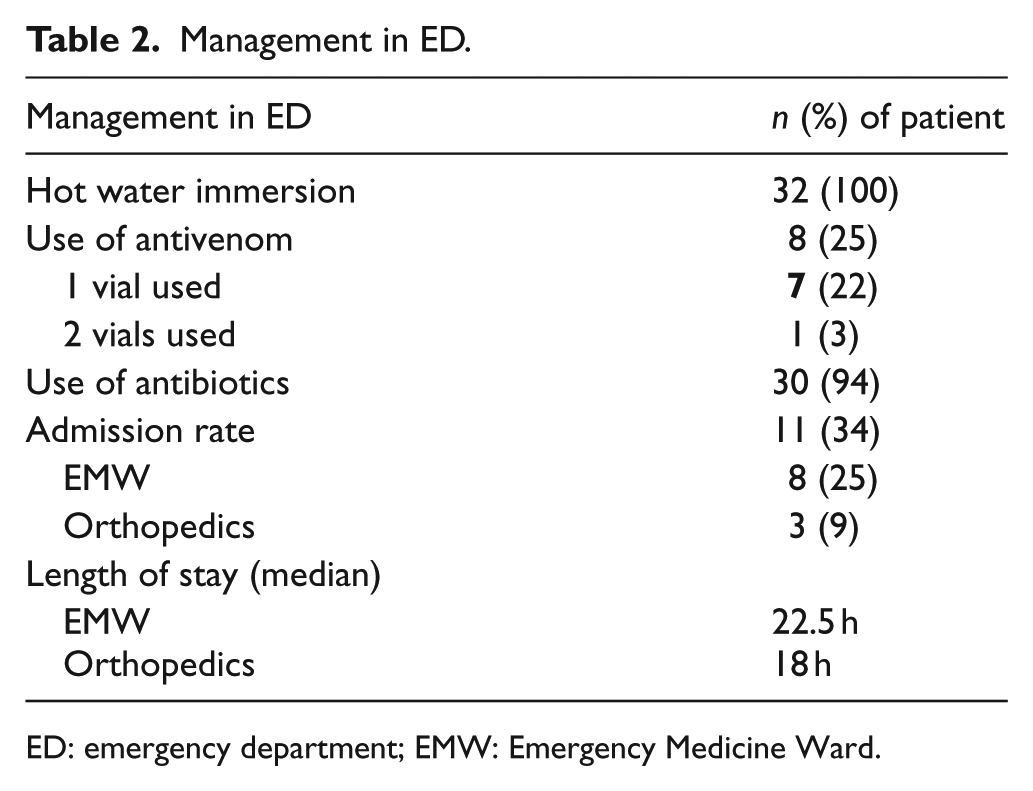
ED: emergency department; EMW: Emergency Medicine Ward.
Types of analgesics use in ED.
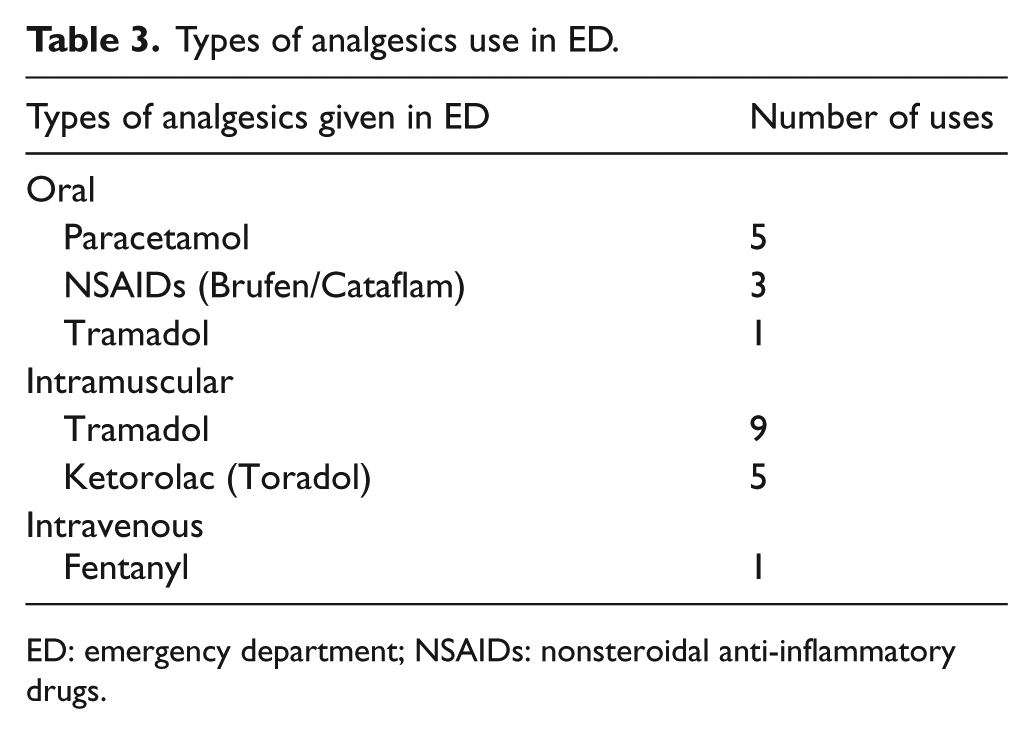
ED: emergency department; NSAIDs: nonsteroidal anti-inflammatory drugs.
Altogether eight patients (25%) received stonefish antivenom for pain relief as shown in Table 2; seven received one vial of antivenom, whereas one patient received two vials of antivenom as he had four puncture wound over his hands. None of them developed allergic reaction or other adverse reaction after the administration of stonefish antivenom.
Twenty-one patients (66%) were treated and discharged with prophylactic antibiotic of quinolone to cover Vibrio infection, and none of them developed complication. For those who could be discharged from ED, the median time of length of stay was 3.5 h (range = 1–23 h). Eleven patients (34%) were admitted to hospital; eight patients were admitted to the Emergency Medicine Ward (EMW), whereas three patients were admitted to the Orthopedics ward. The median length of stay in the EMW and the Orthopedics ward was 22.5 and 18 h, respectively.
Discussion
Stonefish envenomation is one of the common marine stings in Hong Kong. 1 The unaesthetic appearance and toxic venom of stonefish have earned them the label “the master of deceit.” It belongs to the genus Synanceia, characterized by 13 strong and short dorsal spines with distally located venom glands which enable them to deliver a relatively large dose of venom, 2 and is regarded as one of the most dangerous venomous fish stings.3–5 Its sting causes extreme pain, local erythema, gross edema, vesicle formation, cellulitis, and hyperesthesia. Systemic envenomation symptoms include vomiting, sweating, muscle weakness, pulmonary edema, anaphylaxis, hypotension, and even cardiac arrest. 6 However, they have become the regional delicacy and pose an occupational hazard to fisherman, fishmonger, and chefs. 7
Though seldom fatal, a stonefish sting may be so painful that most of our patients (87%) presented themselves to ED within 2 h following the sting. The active component of stonefish venom is a potent membrane-damaging toxin that is capable of releasing substance P and cyclooxygenase (causing intense pain) and increasing vascular permeability (causing swelling).8,9This cytotoxin is heat-labile; thus, immersing the affected body part in hot water (45°C) provides effective relief of pain and swelling. Nonetheless, this is not without risk.
There is a trend of positive correlation of the activity and proliferation of Vibrio vulnificus up to a surrounding temperature of 31°C, which is lower than the temperature of hot water immersion.10,11 While referring to the same aforesaid studies on temperature effect on Vibrio growth,10,11 Tang et al. 12 suggested that the hot water bath used in the absence of prophylactic antibiotics may have facilitated the activity of Vibrio, causing necrotizing fasciitis, and also the concomitant use of prophylactic antibiotics, for example, ciprofloxacin, to cover Vibrio infection upon hot water immersion. Therefore, there is limited evidence of the prophylactic use of antibiotics in hot water immersion.
Most studies support the use of injected antivenom as a potent tool in the management of stonefish envenomation.2,12,13It is a horse anti-stonefish toxin, F(ab′)2 antivenom, with established efficacy for analgesia and diminution of tissue damage due to stonefish sting. 14 It is indicated for stonefish envenomation with significant pain, severe local symptoms (e.g. compartment syndrome), or presence of systemic symptoms (e.g. diaphoresis, muscle weakness, delirium, and convulsion). 15 Due to its equine origin, the antivenom could theoretically cause serum sickness or precipitate anaphylactic reactions, but there is little documented evidence that these adverse effects occur in practice. Within 32 reported cases of stonefish injuries in our study, eight patients received stonefish antivenom. Seven of them received the antivenom in ED for pain relief, and it relieved their pain. One of them received the antivenom after the emergency operation in the Orthopedics ward. None of them developed adverse effect after receiving the stonefish antivenom.
In our study, three patients were admitted to the Orthopedics ward. One case was a 52-year-old man who worked as a fishmonger. He presented to the ED 20 min after stonefish sting injury. He complained of pain, swelling, and bruises over the thenar eminence of right hand (site of sting). X-ray did not reveal any foreign body. The pain and swelling persisted despite hot water immersion and intramuscular ketorolac and tramadol given. With the clinical diagnosis of compartment syndrome, emergency operation of fasciotomy of right hand and forearm was performed 7 h after sting injury. One vial of stonefish antivenom was given to him after the operation (within the same day). He recovered with a course of antibiotics of ciprofloxacin. The other two patients, admitted to the Orthopedics ward, were treated conservatively with wound care, antibiotics, and analgesics in ward. Both of them were discharged uneventfully.
Stonefish is regarded as regional delicacy and it poses an occupational hazard to fisherman, fishmonger, and chefs and a domestic hazard to general public as well. Occupational safety could be enhanced with education (fish identification and the proper way of handling) and use of protective equipment, for example, gloves. The general public may not be aware of the hazard associated with stonefish sting. Further evaluation is needed to see whether we should continue to allow stonefish transaction in the market, where the public can easily gain access.
Limitations of this study
This study is limited by its retrospective nature spanning a duration of 10 years. The number of patients in this study replied on reporting by the physician-in-charge. Under-reporting of cases was often seen in busy ED. Case identification (stonefish) relied heavily on report from patient, and there was a lack of confirmation of which marine envenomation. There were a small number of patients in our series with a paucity of documentation of symptoms and signs in the charts.
Conclusion
Stonefish is a common marine sting in Hong Kong. Its envenomation, though it rarely kills, can cause extreme pain, swelling, and erythema, which can be managed with hot water immersion, analgesics, and prophylactic antibiotics. Use of antivenom can be considered in selected cases.
Footnotes
Acknowledgements
We thank Ms Winnie Cheung, Personal Secretary of Hong Kong Poison Information Centre, for data collection and retrieval.
Authorship
All authors have made substantial contributions to the viewpoints of this study, literature review, and critical revision for important intellectual content. KM Poon drafted the manuscript. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: As editor of this journal, KM Poon was not involved in the peer review of this article. All other authors have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Reported cases of stonefish stings to Hong Kong Poison Information Centre (HKPIC) from October 2008 to October 2018 were included in the study. The cases were retrieved from the HKPIC electronic database.
Ethical approval
The ethic of study was approved by the Research and Ethic Committee in Hospital Authority.
Human rights
Human rights permission is ensured.
Informed consent
This is not required as there is no involvement of clinical trials on human subjects. All patient identifiers have been removed.