
Abstract
Introduction:
Stridor is one of the common presentations of children admitting to emergency department with respiratory distress. The most common etiology of stridor in pediatric age group is infective pathology or ingestion of foreign body. The presentation of dissecting aneurysm causing stridor in pediatric population is very rare and has never been reported in the literature.
Case Presentation:
A 14-year-old boy presented to the Emergency Department with sub-acute onset of stridor after fall from height on an uneven surface. A suspicion of foreign body or an infective pathology was made and the child was shifted to the operating room. After performing a successful intubation under general anesthesia, diagnostic rigid bronchoscopy and esophagoscopy were done which revealed a pulsating external compression of trachea. The child was further evaluated and managed for dissecting aneurysm of the aorta.
Discussion:
Among the various causes for stridor in pediatric-trauma population, dissecting aortic aneurysm is a rare cause. The association of elevated renal parameters to dissecting aortic aneurysm has been documented in various studies. Wheezing, shortness of breath, and stridor indicate a tracheal obstruction in a patient with aortic aneurysm. Computed tomography angiography is the investigation of choice. The defect needs to be repaired by a vascular graft under cardiopulmonary bypass.
Conclusion:
Stridor in pediatric population with etiology as dissecting aneurysm is unusual. A rare presentation like this deserves to be kept in mind while evaluating stridor in pediatric trauma patients by an emergency physician.
Introduction
Respiratory distress is one of the common presenting symptoms of the pediatric population admitted to the emergency department. The associated etiology may be laryngotracheobronchitis and foreign body ingestion. Stridor is an abnormal, high-pitched, whining breath sound caused by a blockage in the throat or larynx that is usually heard in children. Inspiratory stridor implies an obstruction above the level of obstruction and expiratory stridor indicates an obstruction in the lower part of trachea. We describe an unusual case of stridor in a 14-year-old child presenting to the Emergency Department with a history of trauma.
Case description
A 14-year-old child presented to the Emergency Department with complaints of subacute onset of shortness of breath and stridor. The child was unable to speak a complete sentence (probably due to difficulty in breathing) but was conscious and oriented. One day before the presentation, he fell from a height on an uneven surface. He suffered a fracture of the right lower limb and no blunt trauma to the chest. He was primarily treated at a local hospital where the fracture of right lower limb was stabilized with a cast. He had no positive history for bronchial asthma, inhalational injury, recent respiratory infection, or allergic reaction. On examination, the child was conscious, obeyed commands but had high-pitched biphasic sounds with shortness of breath, and used accessory muscles of respiration with no apparent tracheal deviation. On chest auscultation, bilateral air entry was equal with no added sounds. He had the blood pressure of 130/70 mm Hg measured in the right upper limb, pulse rate of 131 per minute, and respiratory rate of 24. His hemoglobin level was 5.8 g/dL, serum creatinine 13.3 mg/dL, and serum urea 254 mg/dL. Lateral view of the neck X-ray depicted narrowing of the trachea below the cricoid cartilage (Figure 1). Anteroposterior view of the chest X-ray showed widening of the mediastinum (Figure 2). As there was no history of chest trauma, a probable diagnosis of foreign body esophagus or trachea was made (most common cause of stridor in pediatric age group).
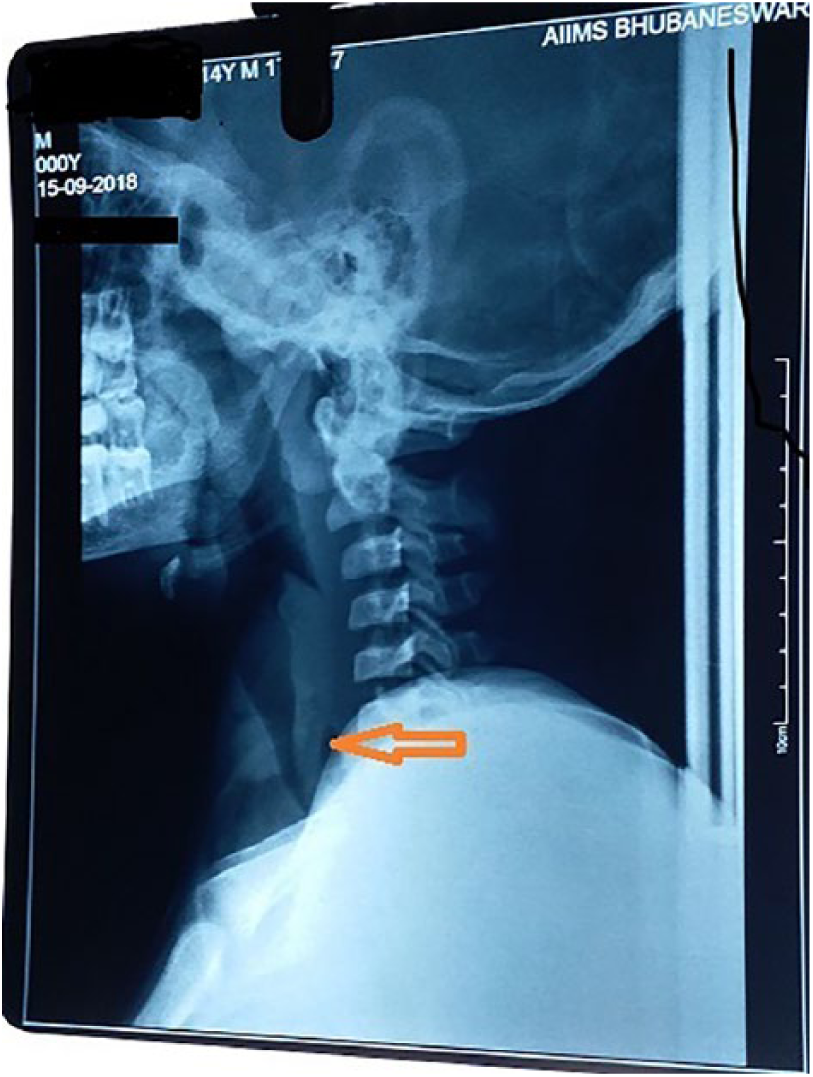
X-ray of the neck (lateral view) depicting narrowed trachea below the cricoid cartilage.
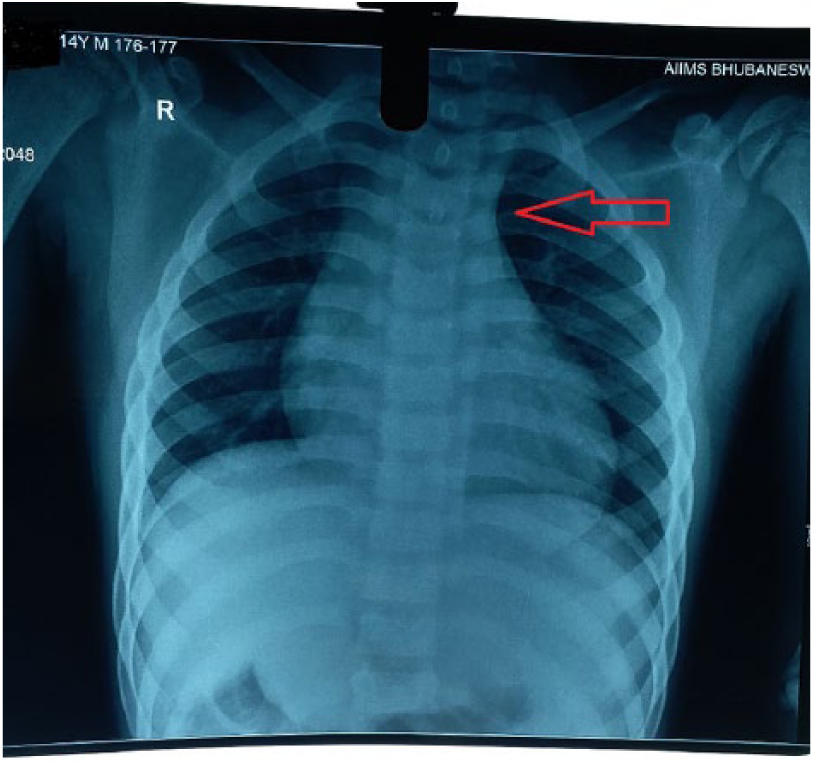
Chest X-ray (anteroposterior view) depicting widened superior mediastinum.
The patient was put in semi-Fowler’s position and oxygen was provided through the Venturi mask at a flow rate of 10 L/min. Dexamethasone injection (3 mg) was given in the emergency department and the child was nebulized with racemic mixture of epinephrine (2.5 mg diluted with 5 mL of normal saline). He was brought to the operating room for diagnostic/therapeutic bronchoscopy or esophagoscopy. We induced the patient with sevoflurane and muscle relaxant was avoided in order to preserve spontaneous breathing. The trachea was intubated with 5.0 mm uncuffed endotracheal tube which was fixed at 16 cm without any difficulty. Rigid bronchoscopy and esophagoscopy did not depict any structural abnormality or foreign body in the trachea or esophagus. There were visible pulsations in the posterior wall of trachea and narrowing of the tracheal lumen as depicted in the video clip (Supplemental Material; https://youtu.be/TQHLmvbXPH0). On inspection, there were visible neck pulsations.
This child presented with progressive stridor associated with dysphagia post-trauma, without fever, which was suggestive of a non-infectious extra-tracheal etiology. Lateral view of the neck X-ray depicted narrowing of the trachea below the cricoid cartilage, and anteroposterior view of the chest X-ray showed widened superior mediastinum, which go in favor of the above perception. An aortic aneurysm was thought of as a diagnosis of exclusion. The child was then shifted to the intensive care unit with the endotracheal tube in situ for further evaluation and management.
Discussion
Stridor is a presentation of disturbed normal breathing pattern due to an obstructed airway. 1 This may present during inspiration (extrathoracic obstruction, above the level of vocal cords), expiration (intrathoracic obstruction, below the level of vocal cords), or both (at and below the level of the cords). Etiology of stridor can be congenital or non-congenital, with an acute or sub-acute presentation. 2 The most common causes of stridor like laryngotracheobronchitis and retropharyngeal or parapharyngeal abscesses were excluded in this case. An aortic aneurysm causes airway compression as it crosses the trachea and left main bronchus. 3 This is a rare cause of stridor which can be considered especially in the pediatric age group. An aortic aneurysm can also lead to tracheomalacia. 4 Hence, the airway needs to be secured without the use of muscle relaxants. The patient with an aortic aneurysm can also present with hoarseness of voice due to the involvement of the recurrent laryngeal nerve. Wheezing, shortness of breath, and stridor indicate a tracheal obstruction in them. 3 The investigation of choice for the detection of an aortic aneurysm is computed tomography (CT) angiography. It has a specificity of 99% and a sensitivity of 98%–100%. 3 The vascular anatomy needs to be delineated for specific repair under cardiopulmonary bypass. This child presented with elevated renal parameters which have a good association with abdominal aortic aneurysms. Obstructed renal blood flow due to the compression of the true lumen by the false lumen in dissecting aneurysms, multiple aneurysms, aneurysmal rupture, uncontrolled blood pressure, and myocardial infarction are other risk factors for chronic kidney disease in these patients.5,6 This case can also be analyzed in terms of post-trauma dissecting infra-renal aneurysm due to the high-impact compression forces leading to longitudinal rupture which is indeed rare.7,8 The intimal tear may be due to direct or indirect trauma. Any patient presenting with high-impact injury, abdominal pain, and decreased pulses in lower limbs must be evaluated by CT angiography, in order to diagnose and initiate early treatment of aortic aneurysm. 7 Maintaining the systolic blood pressure, in fact lowering it to decrease the shear forces and vascular graft placement includes the treatment. 9 Eimany and Roberts 10 reported a case of traumatic aortic dissection in a 65-year-old patient who presented with lower limb ischemia after a car accident. In contrast to our case, this patient presented with completely ischemic lower extremities. Ngu and Konstam 11 presented the case of a 37-year-old woman with a high-impact aortic injury following the use of a surfboard. In 1969, Hewitt and Grablowsky 12 reported the case of a 65-year-old man who was admitted to hospital with an aortic dissection and treated with Dacron graft.
Implications to practice
This case has an ambiguous history of trauma in a 14-year-old child, but the possibility of dissecting aortic aneurysm was not ruled out in the hospital where the patient was admitted previously. The presentation of stridor is the only sign of doubt in this case, with the pulses being palpable. The video clearly depicts the pulsating posterior wall of the trachea. A rare presentation like this deserves to be kept in mind while evaluating stridor in pediatric patients by an emergency physician.
Footnotes
Acknowledgements
The manuscript is the original work of the authors. The manuscript has not been and will not be published elsewhere or submitted elsewhere for publication.
Author contributions
R.B.R. contributed to the management of the case and drafting the manuscript; agreement to be accountable for all aspects of the work. S.B. contributed to the management of the case and drafting the manuscript; agreement to be accountable for all aspects of the work. C.M. contributed to the management of the case and drafting the manuscript; agreement to be accountable for all aspects of the work. M.M. contributed to the management of the case; agreement to be accountable for all aspects of the work. L.K. contributed to the management of the case; agreement to be accountable for all aspects of the work. S.D. contributed to the management of the case; agreement to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data, tables, and figures used in the manuscript were prepared originally by the authors; if otherwise, the sources are cited and reprint permission is attached.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.