
Abstract
A common diagnosis to patients with sudden onset of peripheral facial paralysis is Bell’s palsy. However, when there are other clinical features, such as increased intracranial pressure or bidirectional nystagmus, one must consider central causes. This report illustrates the importance of detailed observation and identification of nystagmus in arriving at an accurate clinical diagnosis.
A lady in her thirties with good past health presented to the emergency department with sudden onset of recurrent vomiting, headache and dizziness. She had no recent infection. Her Glasgow Coma Score was 15. Neurological examination demonstrated full limb power with downgoing plantar reflex, but corneal reflex was absent on the right side. In addition, she was noted to have a right-sided peripheral facial paralysis (House-Brackmann grade IV) without any rash/vesicle in the right ear. Non-contrast computed tomography (CT) of the brain was arranged (Figure 1).
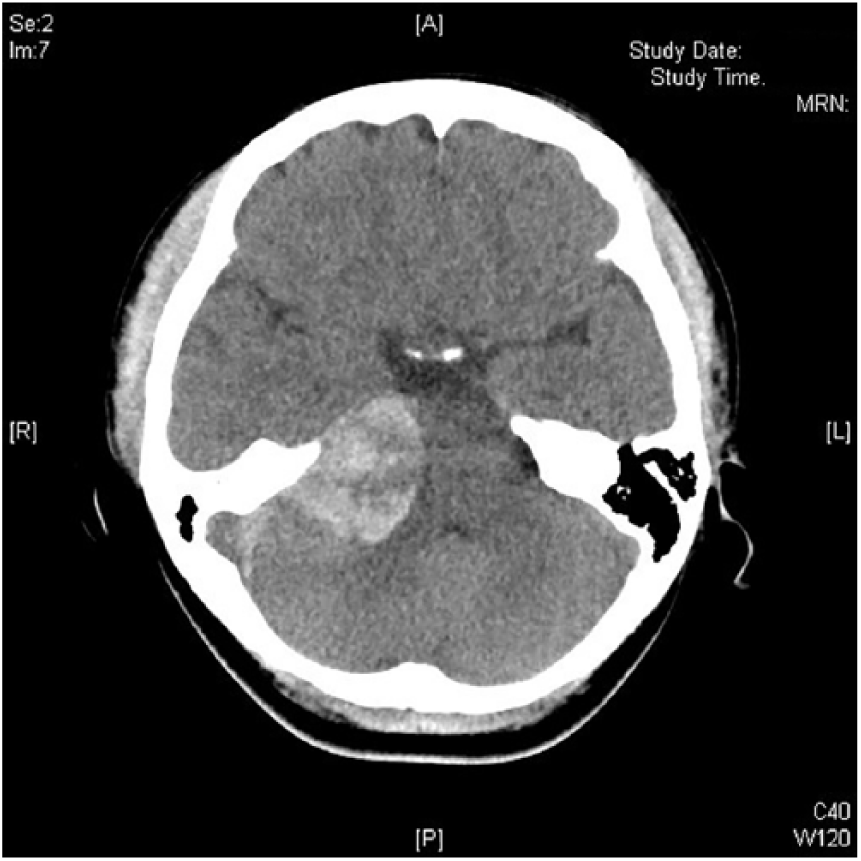
Patient’s non-contrast computed tomography of the brain.
Questions
What were the CT findings?
What was the diagnosis?
Name the specific form of nystagmus related to this condition.
Answers
CT brain illustrated a relatively rounded hyperdense mass with a 3.7 cm maximum diameter in an isodense background at the right cerebellopontine angle (CPA), which compressed on the right pons and right cerebellum. The brainstem was displaced leftward.
The diagnosis was an extra-axial tumour with acute haemorrhage at the right CPA. Its histology was consistent with papillary meningioma with rhabdoid features, a rare variant of malignant meningiomas.
Bruns’ nystagmus.
Discussion
On further examination, a bidirectional nystagmus was observed in this patient. Specifically, a coarse, large amplitude, low frequency right-beating nystagmus with rightward gaze and a fine, low-amplitude, high-frequency left-beating nystagmus with leftward gaze were appreciated.
The detection of Bruns’ nystagmus signifies a space-occupying lesion in the cerebellopontine angle. As a form of jerk nystagmus, it is characterised by alternating fast and slow components. Failure to focus on an object at its extreme deviates the eyes away and contributes to the slow component of the nystagmus. Subsequent corrective saccade refocuses the object and contributes to the fast component of the nystagmus. The pathophysiology of Bruns’ nystagmus involves the concurrent impairment of two neural networks.1,2 While maintaining an eccentric gaze towards the side of the lesion, ipsilateral compression of the neural integrator (pons and flocculus of cerebellum) results in a large amplitude and low frequency gaze-evoked nystagmus towards the side of the lesion. However, while maintaining an eccentric gaze in the opposite direction, decreased tonic firing from ipsilateral peripheral vestibular dysfunction results in a slow-phase movement ipsilaterally and a compensatory low amplitude and high frequency movement contralaterally.
A study by Lloyd et al. demonstrated Bruns’ nystagmus was present especially in those patients with large vestibular schwannoma. 3 In those with tumours larger than 3.5 cm maximum diameter, 92% had nystagmus and 67% of whom had Bruns’ nystagmus. Patients with Bruns’ nystagmus may experience a relatively greater improvement in balance status post-operatively compared with those with no or other forms of nystagmus. Other causes of Bruns’ nystagmus reported include CPA astrocytoma (intra-axial), 4 pontine 5 and cerebellar infarction. 6
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.