
Abstract
Introduction:
Traumatic brain injury (TBI) is a major public health concern, and contributes significantly to mortality and morbidity in paediatric patients.
Objective:
The study is aimed to identify the factors predictive of TBI in paediatric patients with a minor blunt head injury.
Methods:
This was a retrospective cohort study conducted on 274 paediatric patients with a minor head injury and registered to Hospital Universiti Sains Malaysia (USM) from the year 2009 to 2013. Patients with a minor blunt head injury aged less than 18 years who underwent computed tomography (CT) of the brain were included, while the patients with penetrating head injuries were excluded from the study. Simple and multiple logistic regression analysis were performed.
Results:
TBI occurred in 49% of the patients. Headache (adjusted odd ratio (AOR): 2.24; 95% confidence interval (CI): 1.24, 4.05, p = 0.008), dizziness (AOR: 3.08, 95% CI: 1.27, 7.51, p = 0.013) and the presence of scalp haematoma (AOR: 2.93, 95% CI: 1.60, 5.34, p < 0.001) were the most important clinical variables for predicting TBI following a minor blunt head injury in paediatric populations.
Conclusion:
Headache, dizziness and scalp haematoma were identified as important clinical variables that can be used to predict TBI on a CT scan of paediatric minor head injury. The presence of these factors should alert emergency physicians to the need to monitor such children closely.
Introduction
Injury is the leading cause of death in children and teenagers in developed countries with 40% of related deaths being attributed to traumatic brain injury (TBI). 1 Worldwide, TBI has become a major public health challenge and a significant contributor to morbidity and mortality, particularly in populations up to 18 years of age. 2 The rate of TBI in children aged below 15 years was between 75 and 1373 per 100,000 children as stated in previously published studies conducted in Australia, New Zealand and the United States.3–6
TBI accounted for approximately 500,000 visits to the emergency department, 37,000 instances of hospitalisation and more than 2000 deaths every year in the United States. 7 Overall mortality of 5% has been reported in paediatric patients with TBI treated in the emergency department or requiring admission to hospital. The highest paediatric morbidity and mortality is reported in infants aged below 4 years. 8
Asia was reported to have the highest incidence of TBI in a recent review. 9 It was estimated in a hospital-based study that 5% of all paediatric cases admitted to the emergency department in Malaysia involved TBI. 10 However, this study was conducted two decades ago and to the best of the authors’ knowledge, limited studies have been published on paediatric TBI in Malaysia to date.
Thus, the aim of the current study was to determine the most significant clinical variables that can be used to predict TBI in paediatric patients with a minor blunt head injury. It is hoped that the current study findings will add to and inform the literature in this regard, while also being used as a guideline in the management of paediatric patients who present at the emergency department with sustained minor blunt head trauma.
Methodology
This retrospective cohort study was conducted at Hospital Universiti Sains Malaysia (USM), a tertiary level teaching hospital based in Kelantan, Malaysia. This is the only hospital in Kelantan with its own speciality neurology, neurosurgery, neuro anaesthesiology and critical care, neurorehabilitation and neurophysiology department. 11
The records of paediatric patients with a mild blunt head injury who presented to the emergency department of Hospital USM from the year 2009 to 2013 were retrospectively reviewed. Patients aged below 18 years with a mild blunt head injury (Glasgow Coma Scale (GCS) 13–15) who underwent computed tomography (CT) of the brain were included, whereas the patients with a penetrating head injury were excluded from the study. A total of 274 patients were eligible for the study.
A sampling method was not applied since this was a retrospective review. Participants were included in the study provided they fulfilled the inclusion and exclusion criteria. New cases were no longer recruited once the sample size was reached.
The sample size was calculated using Power and Sample Size (PS) calculation software with the significance level at 0.05, the power of 0.8 and the ratio of case to control at 1:1. Based on the variable in the literature review, the calculated sample size required was 97, 117, 230, 22 and 127. Therefore, the researcher took the largest sample size that was 230. In all, 20% of the calculated sample size was added to make up for the missing data and incomplete documentation in case records. Thus, the appropriate sample size for this study was 276.
Data on the participants’ sociodemographic characteristics, mechanism of injury, symptoms and physical signs on arrival at the emergency department, CT findings, and disposition and outcomes were obtained from their medical records. The results of the CT scan were attained from the picture archiving and communication system and interpreted and recorded by the hospital’s radiologist.
TBI is defined as an intracranial haemorrhage or contusion, cerebral oedema, traumatic infarction, diffuse axonal injury, shear injury, sigmoid sinus thrombosis, a midline shift of the intracranial contents, signs of brain herniation, diastasis of the skull, pneumocephalus or skull fracture depressed by at least the width of the table of the skull according to the CT findings.
All the data were recorded on proforma forms. The clinical variables were obtained based on previously established and published clinical prediction rules. Ethical approval was obtained from the hospital’s human research ethics committee and permission to access the patients’ medical records was acquired from the hospital director.
The data were analysed using Statistical Package for Social Sciences® for Windows, version 22.0. 12 The mean with standard deviation (SD) was used for the numerical variables, while frequency and percentage were used for the categorical variables.
Simple and multiple logistic regression analysis were used to identify the most clinical variables for predicting TBI in paediatric patients with a minor blunt head injury. The results are presented as the crude and adjusted odd ratio (AOR), 95% confidence interval (CI) and p-value. Statistical significance was set at p < 0.05.
Result
Demographic characteristics
The sociodemographic characteristics of the study participants are depicted in Table 1. Half (49%) of the 274 patients with head injuries had TBI. The mean age of patients with TBI was 12.15 years (SD of 4.67 years). Majority of the patients with TBI were males and Malay. A large percentage of TBI patients were students at primary or secondary school. Twenty-two per cent of the patients with TBI were not yet at school.
The sociodemographic characteristics of the study participants (n = 274).
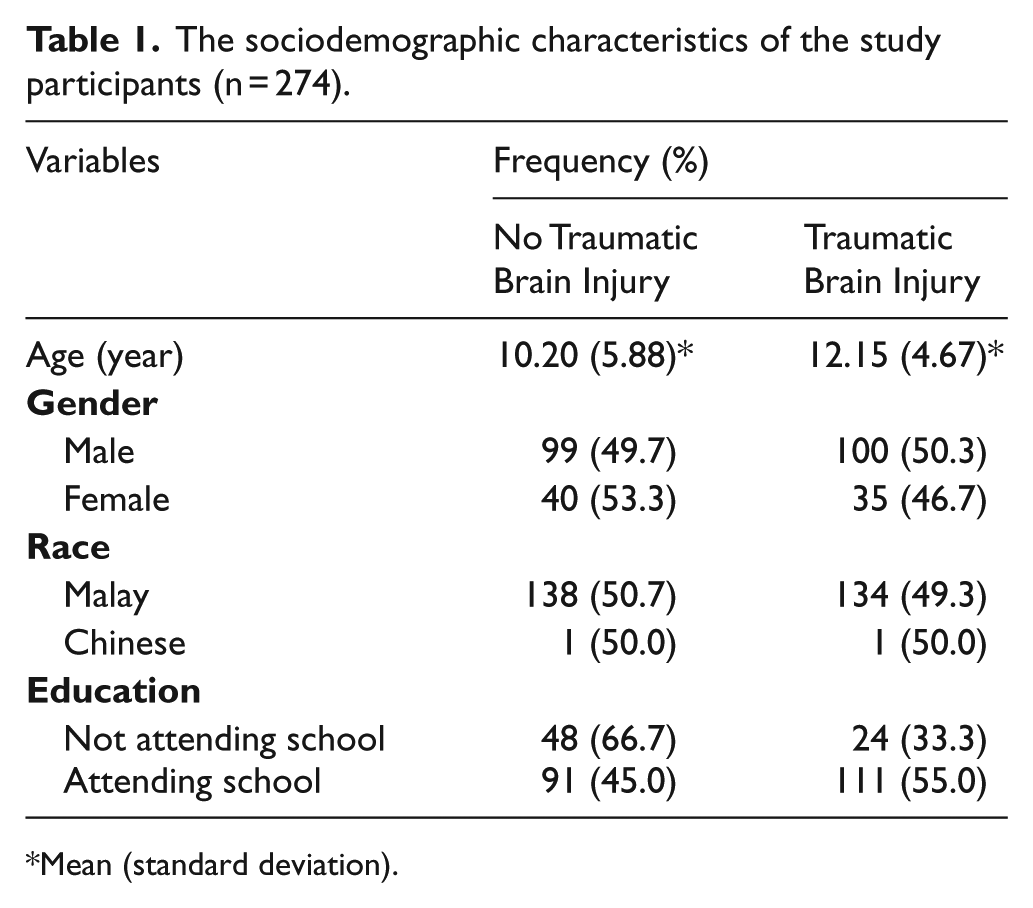
Mean (standard deviation).
Symptoms and signs
The most common presenting symptoms were the loss of consciousness (67.5%), followed by vomiting (53.6%) and headache (37.2%). Most of the patients had full GCS when presented to the hospital (56.9%). The presence of scalp haematoma is the commonest encountered sign on arrival, accounting for 104 cases (37.9%).
Mechanism of injury
The most frequent type of motor vehicle accident (83%) involved motorcycles. Eleven per cent of all motor vehicle accidents involved pedestrians with sustained minor head trauma. Only 5% of all head trauma injuries were attributed to car accidents.
The majority of patients (65%) fell from a vertical height. Sixteen of them fell from heights of less than 3 feet and 14 fell from heights of more than 5 feet. Some of them (7%) fell down the stairs, while others (28%) fell to the ground from a standing position or while walking.
Only 6% of the cases were attributed to a bicycle accident. Seven cases involved a collision or fall, and eight cases were struck by vehicles. Other reported mechanisms of injury were sport- and assault-related injuries, or trauma while walking or running into stationary objects. Falling objects struck the heads of 5% of cases.
Predictive factors
It was established that headache (AOR: 2.24; 95% CI: 1.24, 4.05, p = 0.008), dizziness (AOR: 3.08, 95% CI: 1.27, 7.51, p = 0.013) and the presence of scalp haematoma (AOR: 2.93, 95% CI: 1.60, 5.34, p < 0.001) were the most important clinical variables for predicting TBI due to minor blunt head injury in paediatric populations, and that these findings were statistically significant (Table 2).
Statistically significant predictors of traumatic brain injury in paediatric patients with minor blunt head injury (n = 274).
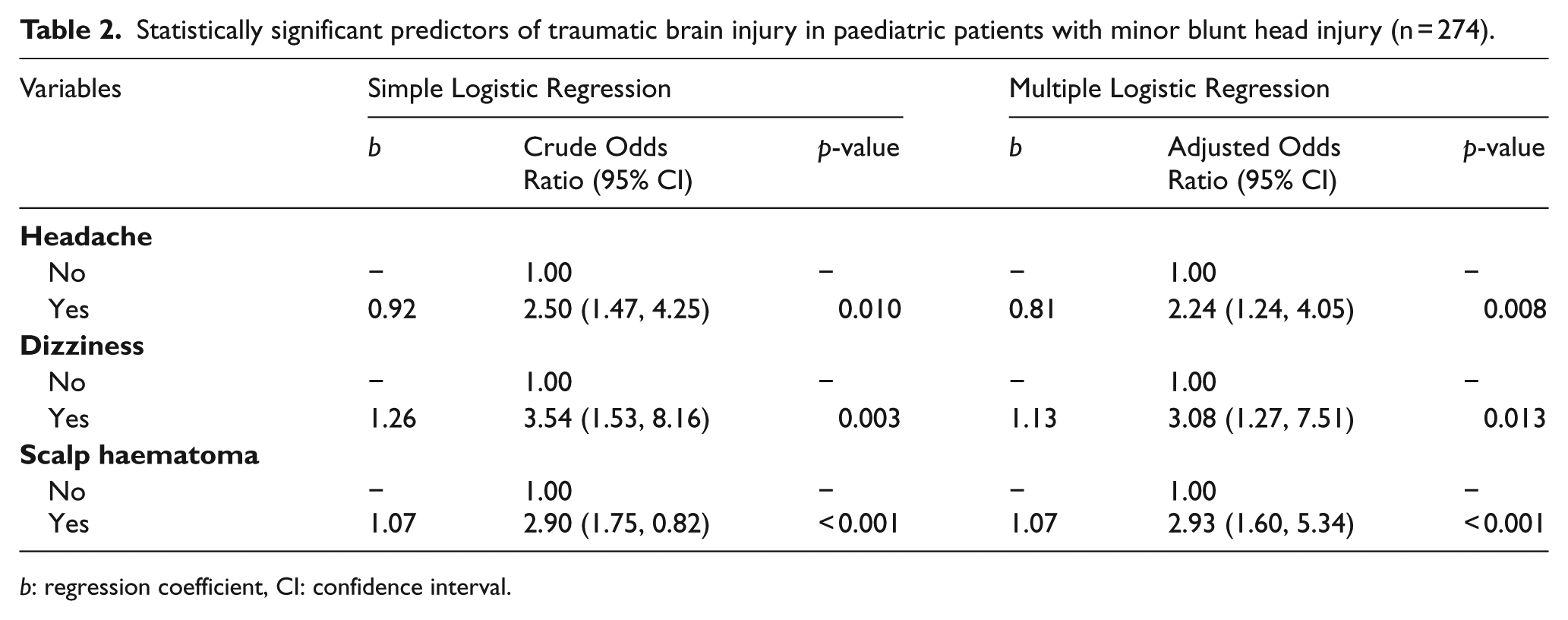
b: regression coefficient, CI: confidence interval.
Discussion
Three factors were found to be statistically significantly associated with the ability to predict TBI in paediatric patients with a minor blunt head injury on multivariate analysis: headache, dizziness and the presence of scalp haematoma.
Headache
The present study found that headache isa predictive factor of TBI in paediatric patients with a minor blunt head injury. Headache is a commonly presenting symptom occurring in up to 46% of such children. 13 According to the Pediatric Emergency Care Applied Research Network (PECARN), children with a blunt head injury, aged 2 to 18 years and with a history of severe headache are at high risk of TBI. 14 Worsening headaches were reported as a high-risk factor for TBI in the Canadian Assessment of Tomography for Childhood Head Injury study. 15
However, the current study finding was not supported by that in the study by Dayan et al. 13 They found that TBI was not associated with either headache severity or location. 13 Differences in the study populations and methodology used might explain the dissimilar results. Only GCS of 14 and 15 patients were recruited in their study, whereas those with GCS of 13 to 15 were included in the current research. The rate of TBI in children with GCS 13 had been reported to be as high as 20%.16,17 Perhaps this explains why patients with GCS 13 are excluded from assessment in the majority of TBI studies as a CT scan of the brain is routinely conducted as part of the investigations, regardless of the presence of other symptoms and signs relating to altered mental status. The focus in the study by Dayan et al. 13 was on isolated headache in the absence of other signs and symptoms; a major difference when compared to the current study objective.
Dizziness
Dizziness was found to be associated with TBI in paediatric patients with a minor blunt head injury in the current study. However, according to PECARN, dizziness was not identified as being significantly clinically associated with TBI in all-age paediatric age groups. There are a few possible explanations of why it is seldom included as a clinical variable in research on TBI. This symptom is very subjective and is difficult to define clinically. It is delineated in the PECARN study as any vertigo-type sensation, a sense of physical imbalance or postural instability. Dizziness is difficult to assess in children who are unable to adequately express themselves verbally. Preschool children might not be able to understand the meaning of dizziness, vertigo or unsteadiness. A headache, on the other hand, is much easier to identify and assess, and that is probably the reason why it dominates the interest of researchers.
However, difficulty with understanding the definition of dizziness did not apply in the current study as most of the children were aged more than 10 years and were able to express themselves eloquently. They understood the questions asked of them when the details of their history were taken and communicated well with the treating physician at the time that they presented at the emergency department.
Scalp haematoma
Scalp haematoma was also identified in the current study as being significantly associated with and predictive of TBI in paediatric patients with a minor blunt head injury. Non-frontal scalp haematoma was determined to be a clinically significant factor in terms of ability to predict TBI in patients aged below 2 years with a minor blunt head injury in the PECARN study. 14 A higher prevalence of TBI in infants aged below 6 months with isolated scalp haematoma, compared to that in older children, was found following subsequent secondary analysis by Dayan et al. 13 using CT.
Scalp haematoma (more than 5 cm) was regarded as an indication for CT of the brain in children aged below 1 year with a minor blunt head injury using the Children’s Head Injury Algorithm for the Prediction of Important Clinical Events. 16 By contrast, a large ‘boggy’ (soft) scalp haematoma was identified as a medium-risk factor for TBI in the Canadian Assessment of Tomography of Childhood Head Injury study. 15
It was suggested in research by Palchak et al. 17 that scalp haematoma should be considered a key factor in the identification of children aged less than 2 years at low risk of TBI. Scalp haematoma in this age group was included as a variable to determine the need to undergo CT scanning.
Scalp haematoma is an important indicator of the need for a CT brain in infants and toddlers because young children do not often have any immediate signs or symptoms following a minor head injury, other than scalp haematoma. 18 They are also unable to describe their symptoms as they do not have an advanced vocabulary. History taking is difficult and positive findings on physical examination appear to be an important indicator of TBI, thus requiring a CT scan of the brain.
However, scalp haematoma was not found to be diagnostically useful as a clinical factor in predicting the likelihood of an intracranial injury in a meta-analysis. 19 Elsewhere, following a retrospective review, scalp haematoma was not found to have a significant association with the pathological CT findings attributed to a mild head injury, although it is the most frequent CT brain finding. 20
Nevertheless, there was a marked difference in the methodology used between that study and the current one. They excluded patients with GCS of 13 and 14, and those aged less than 2 years. 20 In addition, the difference in the sample populations could be a major contributory factor to the discrepancy between the results. Thus, the inclusion of scalp haematoma as a consideration for CT imaging is recommended, especially when dealing with preverbal infants with limited complaints following minor trauma to the head.
As conclusion, headache, dizziness and scalp haematoma were identified as important clinical variables that can be used to predict TBI on a CT scan of paediatric minor head injury. The presence of these predictors should alert emergency physicians to monitor children with head injuries more closely. Further cross-sectional studies with a larger sample size, of longer duration and larger number, should be performed to determine high-risk factors in paediatric patients with a minor head injury, and especially dizziness, as only a few studies have included this symptom in their assessments to date.
Limitations
There were several limitations to the current study. First, missing data were an inevitable disadvantage owing to the retrospective nature of the study. Several variables were not included in the analysis because of incomplete data, including an altered consciousness, lethargy, visual and speech changes, abnormal behaviour (according to the parents), unequal pupils, a bulging fontanelle, signs of a basal skull fracture or palpable skull fracture, severe headache, the size of the haematoma and the exact location of a scalp haematoma.
Besides, Patients with GCS above 13 were included. However, there is controversy regarding the exact definition of a minor head injury. Some clinicians believe that GCS 13 equates to moderate TBI and that such patients should undergo CT of the brain routinely to identify intracranial bleeding.14,21 By contrast, others classify GCS 13 as a minor head injury and advocate that such patients should be evaluated according to the clinical guidelines before a decision is made as to whether or not they should undergo a CT of the brain.
The sample for the current study was recruited from a single centre. Therefore, the results may not be generalisable. Future studies are warranted that involve data collection from other hospitals, including those assigned to the Ministry of Health to remedy this.
Footnotes
Acknowledgements
Special gratitude goes out to all staffs and doctors in Emergency Department who assisted in the study, with special mention to the Hospital Director of Hospital Universiti Sains Malaysia and the Human Research Ethics Committee for granting the use of patients’ data, as well as the approval for study conduct. This manuscript is submitted solely to the Hong Kong Journal of Emergency Medicine (HKJEM) and was not published or submitted elsewhere. It had been read and approved by all authors. The authors made a substantial contribution to the concept, study design, acquisition, analysed and interpretation of data, drafted and revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data of materials
The authors declare that no data have been fabricated or manipulated (including images) to support the conclusions. The authors declare that no data, text, or theories by others are presented as if they were the authors own.
Ethical approval
Ethical approval was granted by the Human Research Ethics Committee of Universiti Sains Malaysia (USM/JEPeM/14110413).
Human rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
For this retrospective study, informed consent is not required.