
Abstract
A 2-year-old boy presented with abdominal pain and non-coffee-ground emesis for 1 day. He was afebrile and without decreased activity. Examination showed lower abdominal tenderness, but psoas and obturator signs were negative. Laboratory test showed mildly elevated C-reactive protein (1.321 mg/dL) without leukocytosis. An abdominal X-ray revealed a high-attenuation-calcified lesion near the right sacroiliac joint which was highly suspected as an appendicolith. Subsequent abdominal computed tomography proved an appendicitis with appendicolith inside. He underwent laparoscopic appendectomy and was discharged uneventfully 4 days later. Acute appendicitis is a commonly misdiagnosed pediatric emergency because of the atypical presentations. Appendicoliths are presented in more than half of pediatric appendicitis and are highly associated with perforation. Surgery is recommended instead of antibiotics therapy alone to manage appendicolith-related appendicitis. A careful interpretation of the plain abdominal films and keeping a high suspicion are vital to early diagnosis of this disease.
Case
A previously healthy 2-year-old boy presented to the emergency department with abdominal pain and 3 times of non-coffee-ground emesis for 1 day. He did not have a fever or change his activity. In physical examination, patient was irritable when palpating his lower part of abdomen. Both psoas and obturator signs were negative, and no muscle guarding was found. Laboratory tests showed normal white blood cell counts (WBC: 8840 µL−1), but mild elevation of C-reactive protein (CRP: 1.321 mg/dL). An abdominal X-ray was performed and shown in Figure 1.

The abdominal X-ray showing a round calcified lesion near the sacroiliac joint (arrow).
Questions
What are the findings in the abdominal X-ray?
Which surgical abdomen should be considered in this boy?
How should this patient be managed?
Answers
A high attenuation calcified lesion near the right sacroiliac joint (Figure 1, arrow) and focal dilated loops of small bowel in the left upper abdomen were found.
Appendicolith-related acute appendicitis.
Further image study like ultrasonography or abdominal computed tomography (CT) should be performed to evaluate the possibility of appendicolith-related appendicitis. For pediatric patients with appendicolith-related appendicitis, surgical treatment is required rather than non-surgical treatment with antibiotics.
Discussion
This patient underwent a CT scan of the abdominal because it was suspected to be acute appendicitis associated with an appendicolith formation. The CT scan revealed a dilated appendix with an appendicolith inside (Figure 2, arrows). Acute appendicitis with appendicolith formation was diagnosed. He received emergency laparoscopic appendectomy and was discharged uneventfully 4 days later.
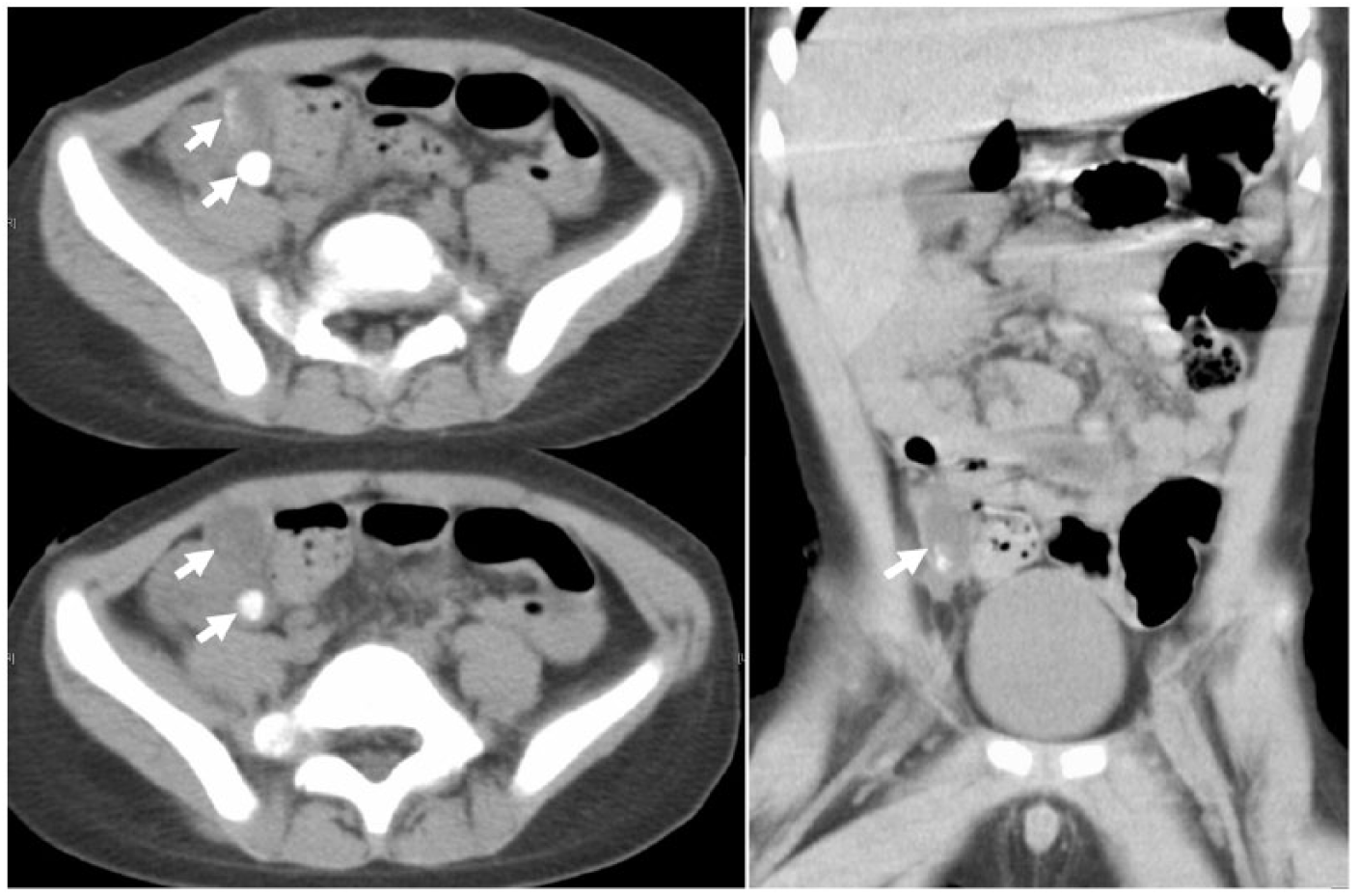
The CT scan of abdomen showing a dilated appendix with an appendicolith inside (arrows).
Acute appendicitis is a commonly pediatric emergency. Because the clinical presentations are frequently atypical and overlap with other gastrointestinal disease, delayed diagnosis and a high perforation rate are the characteristics of pediatric appendicitis, especially in young children.1–3 Previous studies have demonstrated that appendicoliths are present in more than half of pediatric appendicitis.1,3 More importantly, high perforation rate (up to 88%) is significantly associated with the presence of appendicolith in pediatric appendicitis.1,3 Although non-operative management with antibiotics therapy can be used as primary treatment in pediatric patients with uncomplicated appendicitis, high failure rate was observed in the presence of appendicolith.2,4 Hence, surgical management is suggested for appendicolith-related appendicitis in pediatric patients. 2 The diagnostic approach for pediatric appendicitis should combine history, physical examination, and laboratory findings, including WBC and CRP. 5 A pediatric appendicitis risk score or appendicitis inflammatory response scoring system is applicable clinically. Further imaging study, like ultrasound or CT, is indicated in intermediate probability group. 5 However, an equivocal finding on examination and a low risk score are not uncommon, like in this patient. Therefore, a high degree of suspicion and careful interpretation of the plain abdominal films may help to make an early diagnosis of this disease.
Footnotes
Acknowledgements
The manuscript, as submitted or its essence in another version, is not under consideration for publication elsewhere and will not be published elsewhere while under consideration by the Hong Kong Journal of Emergency Medicine. The authors have no commercial associations or sources of support that might pose a conflict of interest. All authors have made substantive contributions to the study, and all authors endorse the data and conclusions. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data sharing is not applicable to this article as no data sets were generated or analyzed during this study.
Informed consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.
Ethical approval
Ethical approval was not required as no patient’s identifiable data were disclosed.