
Abstract
Objective:
The goal of this prospective cross-sectional study was particularly to collect data on the epidemiology, the pattern of injury among motorcyclists and to relate with spatial data in a local district.
Methods:
It involved data collection from prehospital care and inhospital care record. In addition, it utilized geospatial ARCGIS® version 10.1 software in the identification of hotspot location of road traffic injury. Written informed consent was obtained from patient(s) or relatives for their anonymized information to be published in any article.
Results:
A total of 439 cases were recruited over 10 months. The mean age (standard deviation) of the motorvehicle crash victims was 26.04 (15.26) years. Male comprised 302 (73.3%) of the cases. A total of 176 (42.7%) of the victims were between the ages of 20–40 years. A total of 176 (42.7%) of the motorcyclists admitted were wearing the safety helmets either from the history taking or from the witness. A total of 117 (28.4%) and 28 (6.8%) of the victims were admitted to the general wards and critical care units, respectively for further management. The mean (standard deviation) length of hospital stays was 7.19 (6.94) days. Based on hotspot mapping using ARCGIS 10.1, most of the motorvehicle crash cases occurred mainly within the specific borough. This finding concurred with the locations of the state roads involved that traversed mainly within the same borough. Further geospatial and temporal analysis showed that most of the motorvehicle crash that occurred during the weekend were located within the suburban areas.
Conclusion:
Motorcyclists, being male and young age are the vulnerable group of road users commonly injured on our road. The initial geospatial analysis of injury-related motorvehicle crash cases has shown common hotspot trending along certain roads and borough within the district. This new knowledge can be used in the future for preventive and road safety programs in high-risk areas.
Introduction
Malaysia is a middle-income country and is typical of countries that have seen a decline in infectious disease but an increase in death and disability from injuries over the past few decades. Road traffic deaths and injuries today place an enormous strain on the country’s health-care system and national economy. More than 6000 Malaysians are killed annually on the roads, and many more are seriously injured. Undoubtedly, the large numbers of road traffic injuries (RTIs) relate directly to the ever-increasing number of road users. 1 In 2006, the number of registered vehicles were 15,790,732 and motorcycles were 7,035,930. A decade later in 2016, the number of registered vehicles increased substantially to 27,613,120 and motorcycles were 12,933,042. 2
The index of road traffic accidents to 100,000 of the population was 24.20, and index of road traffic accidents to every 10,000 of registered vehicle is 3.40 in 2015. 3 Motorcycle-related road accident is perhaps the commonest cause of RTI being reported in Malaysia. In general low-income and middle-income countries on an average have higher motorvehicle crash (MVC)–related death rate than the more developed and high-income countries (21.5 per 100,000 vs 10.3 per 100,000 population).4,5 Half of those injured and died involve the most vulnerable road users such as children, pedestrian, and two-wheeler users.6,7 The victims commonly involved the young age group (40% at between 20–40 years of age), the age at which the general population is very productive socioeconomically. Sadly, significant amount of the victims were among the school-aged population ranging from primary schools to the late adolescent (28%). Male group contributed significantly to the MVC victims compared to the female counterpart. The young age and being a male, both are common denominators in any motorcycle-related injury cases worldwide. 8
Therefore, the preventive measures and clinical care should be focusing on this group or road users in order to reduce the overall burden of RTI in Malaysia. Similarly, the enforcement of road safety and law on the road should also look at how to reduce impacts of RTI among these vulnerable road users. Much of the preventive programs and efforts on road safety in Malaysia are based solely on the non-clinical data. The knowledge of the epidemiological and clinical characteristics of motorcycle-related RTI is the backbone for trauma care planning, injury prevention, and systems improvement. The integration between the prehospital and inhospital data will assist the policymakers and the clinicians in promoting the preventive programs and hence enhance the road safety programs for motorcyclists locally and nationwide. Specifically, very little information has been gathered pertaining to the relationship between the spatial information and the actual clinical outcome of the patients who sustain motorcycle-related injury. Much of the studies in the past just identified clinical parameters of RTI but no correlation analysis has been done in relation to spatial factors.9,10 It would be ideal and interesting for the policymakers to know this correlation so that effective preventive and sustainable surveillance programs can be implemented.
Thus, the goal of this study is particularly to collect data on the epidemiology, the pattern of injury among motorcyclists and to relate with spatial data in the district of Kota Bharu. This study planned to utilize the geographical information system (GIS) software and performed the spatial-time analysis in relation to clinical data (Geoclinical) for motorcycle-related injury cases attending the emergency department (ED). The primary aim of this study is to document the demographic parameters, the predominant injury mechanisms and severity, geographical positioning data (i.e coordinates of the incidents locations), mortality, and length of hospital stay. The overall output is an integrated spatial-temporal, prehospital, and clinical data. This study provides additional reliable and integrated data that can be used for planning current and future trauma care related to RTI among the motorcyclists in Kota Bharu specifically and in Malaysia generally.
Methods
A prospective cohort study over 12 months was carried out that involved all motorcyclists (main and pillion riders) patients attending the EDs of two tertiary centers in the district of Kota Bharu Kelantan located in a northeastern part of Peninsular of Malaysia. Consent was taken from each patient or relatives by using standard consent form approved by the research and human ethics committee of the School Of Medical Sciences USM, Kota Bharu, Malaysia. The framework of the study is based on the public health system approach model that combines the clinical, geographical, and mechanical and road user data gathered from all victims of motorcycle crashes within the study locality. At the initial part of the presentation in the ED, a series of vital signs were taken, and injury severity scoring was carried out. The common parameters measured include the blood pressure, respiratory rate (RR), heart rate, Glasgow Coma Scale (GCS), revised trauma score (RTS), and the number of body parts or systems injured.
Patients would be included based on the following criteria:
All patients who attended ED with RTIs related to motorcycle use within the district of Kota Bharu.
Patient who died in ED secondary to RTIs.
All severe trauma patients related to RTI (any one of the following):
11
All patients requiring admission to hospital more than 24 h for further management in a tertiary center. Abnormal vital signs on presentation (RR <10 or >30/min, presence of cyanosis, hypotension systolic <90 mmHg, GCS <15). All penetrating injuries. Significant blunt injuries to head/neck/chest/abdomen/groin and involving two or more body regions. Specific injuries, that is, limb amputations/limb-threatening injuries/suspected spinal injuries, burns >20%, facial burns, serious crush injury, major compound fractures, fracture of two or more long bones, and fractured pelvis. Patients with high risk of mechanisms of injury, that is, ejection from vehicle, motorcylist impact at >30 km/h, fall from height >5 m, high-speed MVC >60 km/h, vehicle rollover, and explosion. Presence of comorbidity, that is, age <10 or >55 years, pregnancy, and significant medical problems.
Patients were excluded based on the following exclusion criteria:
Patients with inadequate information that are needed for the study.
No or missing global positioning system (GPS) location identified.
RTI cases that occurred outside the district of Kota Bharu.
Patients with non-road-related injuries, that is, domestic violence, fall at work, assault, and so on.
The researcher asked the prehospital care providers (ambulance services) and patients or relatives to specifically identify and draw the map location of the accidents. The researcher attended each of the location of incidence and obtained x and y GIS coordinate in degree, minute, and second in World Geodic System (WGS) 84 format using a handheld GPS unit brand Garmin model GPS 72H (serial no.: 1T7071348; manufactured in Taiwan by the Garmin Corporation in 2010) which was accurate to 5 m of the location (Figure 1). The coordinates were documented into the case report form for each of the patient case. All of the victims involved at any particular incident location were recruited into the study.
GPS Garmin model 72H.
A set of digital maps was obtained from the Town Planning Unit of Kota Bharu Municipal Office (local district map). Vector spaces were spanned over these maps using GIS software (ARCGIS 10.1 licensed to USM), and attributes as explained in previous subsection from the identified trauma cases were added. The coordinates obtained were converted into a compatible format by using MapInfo Professional software version 10.0. The coordinates for each of the RTI case were then mapped into digital layers of road network, borough, and land use. The GIS analysis included general borough mapping, road network RTI locations mapping, and inverse distance weighting (IDW). IDW was used to identify the density of RTI and hence the common hotspot for RTI within each borough. General spatial analysis was also performed for motorcyclists involved in RTI based on type of injury, prehospital data, and inhospital clinical data. Sample calculation for the study was based on Weiner & Tapas article published in 2009, alpha value of 0.05, z value of 1.96, and power 0.8 that required the investigator to collect 440 cases inclusive of 20% drop out.
Results
A total of 439 cases were recruited over 10 months. The total patients attended the ED over the study period was approximately 53,000, and hence the prevalence of motorcycle-related RTI cases for our study center was 0.83%. The variables collected were divided into general demography, prehospital, clinical, and geographical data. A total of 66 cases (15%) were excluded due to lack of GIS coordinates, location beyond the study objective, and missing variety of clinical variables.
The median age of the MVC victims was 21 (interquartile range (IQR): 17, 35) years. The range of age was between 2 and 81 years. Male comprised 302 (73.3%) of the cases (Table 1). A total of 176 (42.7%) of the victims were between the ages of 20–40 years. Majority of the victims were also among the adult group (i.e above 18 years of age; 320 (77.7%)). A total of 191 (46.4%) of the victims possessed valid driving license for the vehicle involved. A total of 61 (14.8%) of the victims did not disclose whether they held any driving license, partly due to inability to give history or refusal to disclose. Majority of the victims were the main rider of the motorcycles involved in the crash (n = 320 (77.7%)). Majority of the vehicles ridden by the victims were hit by another vehicle. A total of 49 (11.9%) of cases resulted from spontaneous skid and falls without any two-vehicle impact. A total of 176 (42.7%) of the motorcyclists admitted wearing the safety helmets either from the history taking or from the witness. However, 120 (29.1%) of the victims do not disclose whether they wore the helmets during the incidents. Majority of the victims were brought to the ED by the hospital ambulance. Others were brought in by other means such as own transport, police vehicles, and private ambulances. The ED triage distribution for all the victims was as shown in Figure 2.
Demographic pattern of the motorcycle-related road injuries.
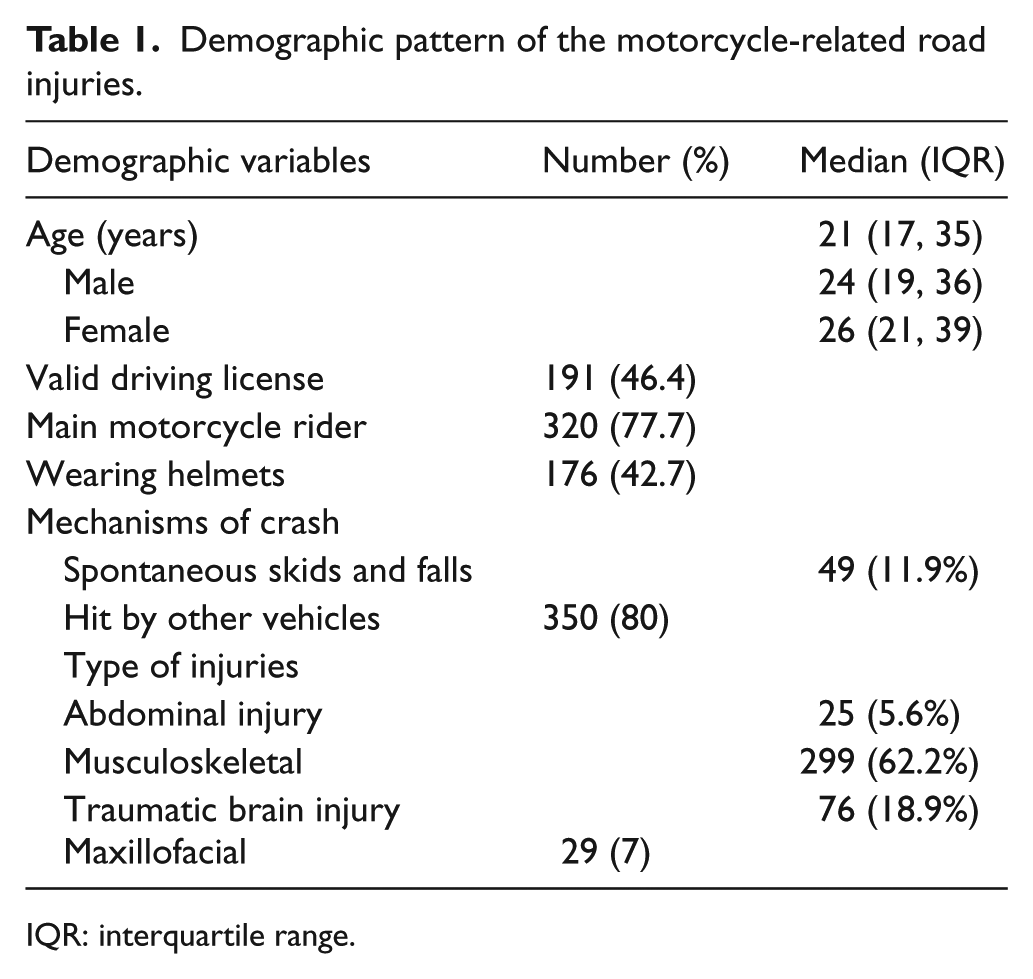
IQR: interquartile range.
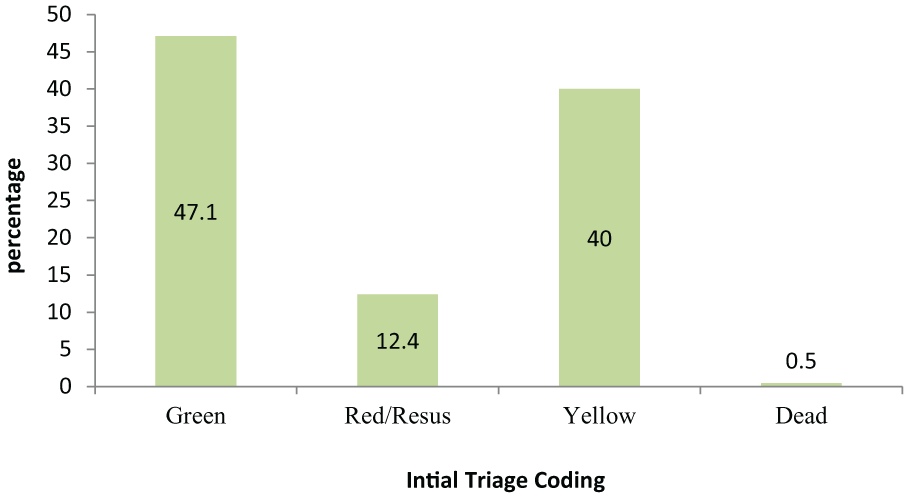
Triage coding for victims of all motorcycle-related injuries.
Table 2 shows the numerical data values for few of the initial vital signs obtained at the triage counter or in the treatment cubicles. This included the systolic blood pressure (SBP), GCS, and RR. The table also depicted the number of body systems and body parts injured, RTS, and Injury Severity Score (ISS). A total of 145 (35.2%) victims were admitted to the wards. A total of 117 (28.4%) and 28 (6.8%) of the victims were admitted to the general wards and critical care units, respectively, for further management. The median length of hospital stays was 5 (IQR: 3, 10) days, ranging from 1 to 51 days. A total of 48 (33.8%) of the victims who were admitted, stayed longer than 7 days in the hospital. Majority of the patients were discharged directly from the ED 268 (65.0%). A total of 44 (10.7%) of the victims sustained polytrauma which was defined as two or more bodily systems injured with signs of life-threatening conditions.
Vital parameters of all motorcycle-related injured victims.
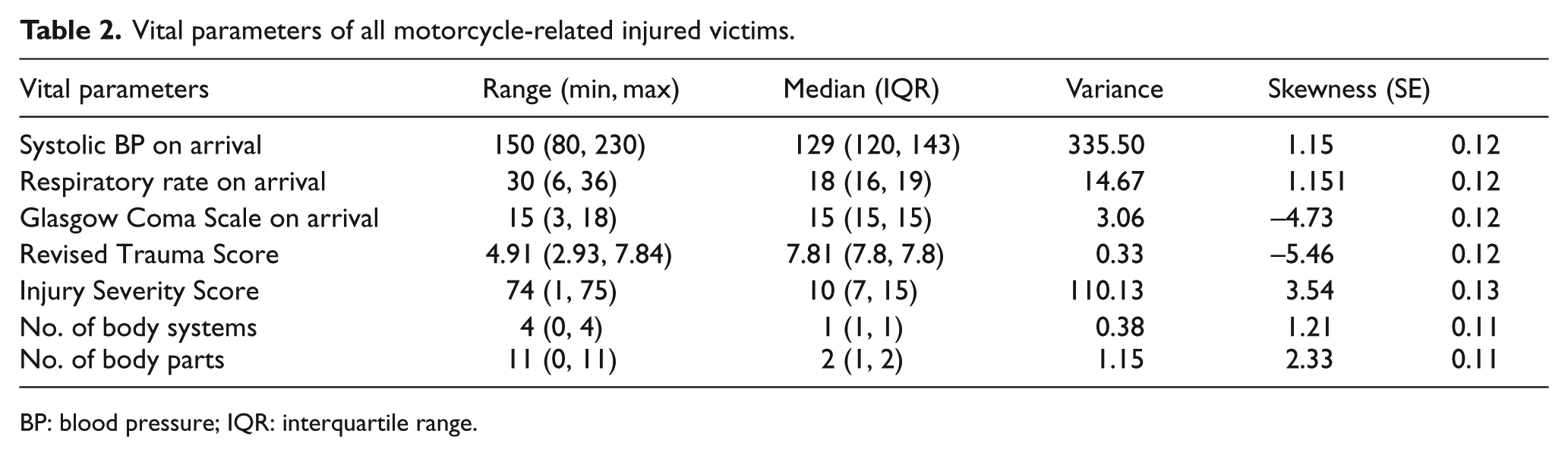
BP: blood pressure; IQR: interquartile range.
The mapping of the coordinate locations for all the MVC cases within the study period was plotted as below based on the borough and road network layers (Figures 3 and 4). Based on IDW (hotspot mapping), most of the MVC cases occurred mainly within specific borough namely Kenali, Chicha, Demit, and Pauh. This finding concurred with the locations of the state roads involved that traversed mainly within the same borough. The roads were major trunk road connecting one borough to another. Further geospatial and temporal analysis showed that most of the MVC that occurred during the weekend were located within the suburban areas namely Guntong, Binjai, and Chicha, whereas those that occurred during weekdays were located mainly in the borough of Kenali and Demit. Similarly, the peak hour incidences occurred mainly on the main trunk road traversing through borough Kenali. The non-peak-hour incidences were more equally distributed within other borough and affected more within the suburban areas (Figure 5).
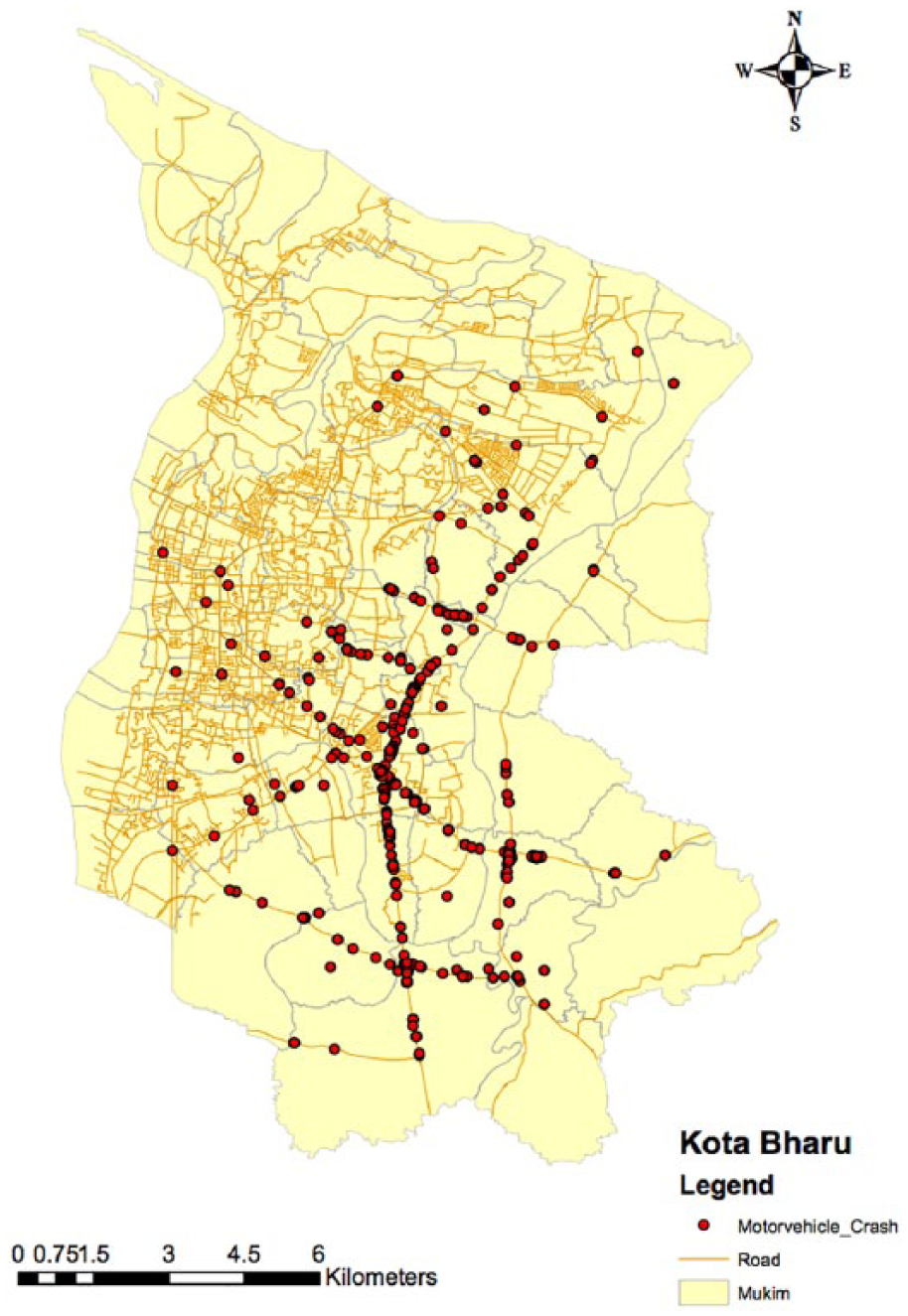
Locations of all MVC based on road network.
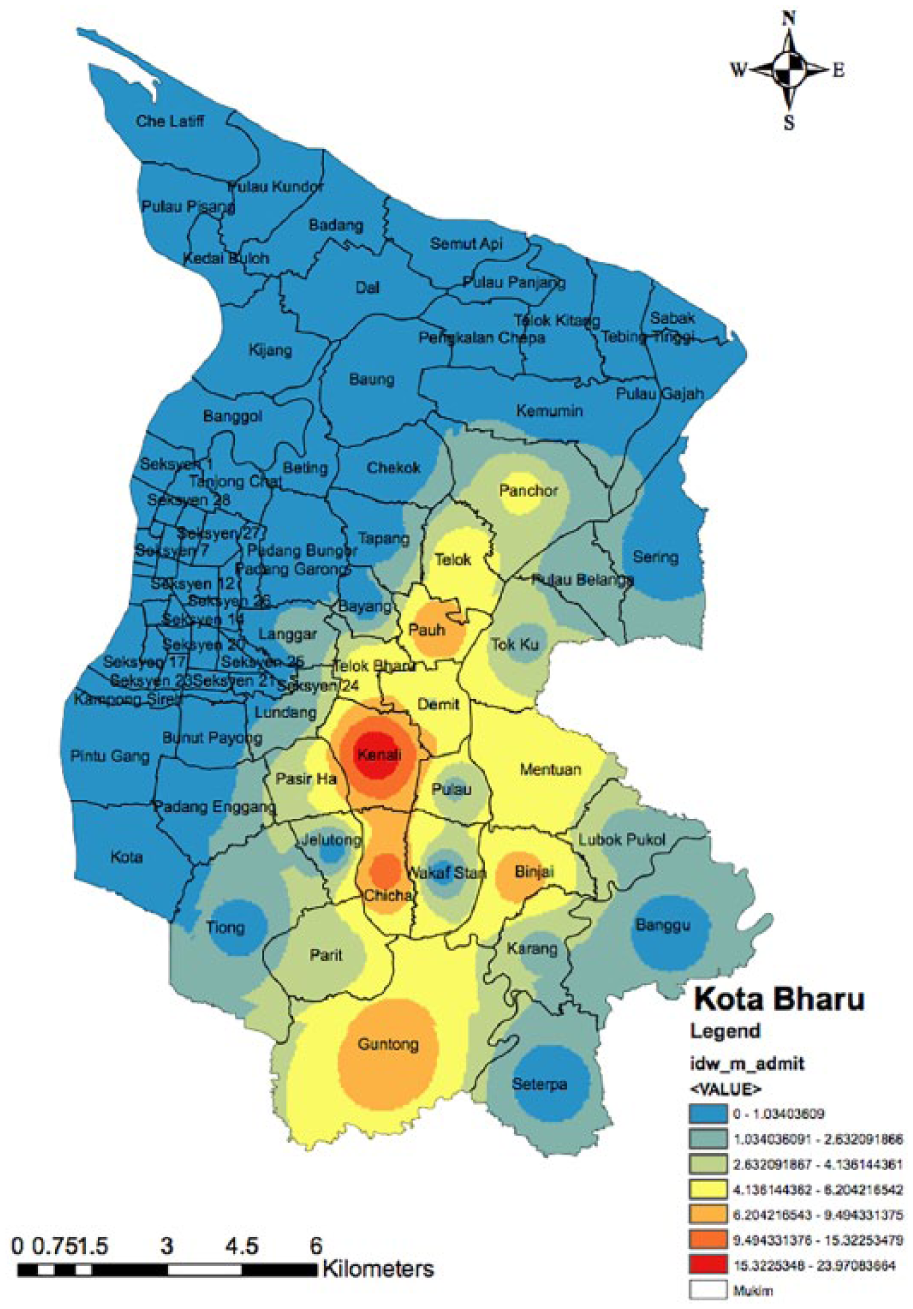
Map of motorcycle crash (driver) based on inverse distance weighting analysis.
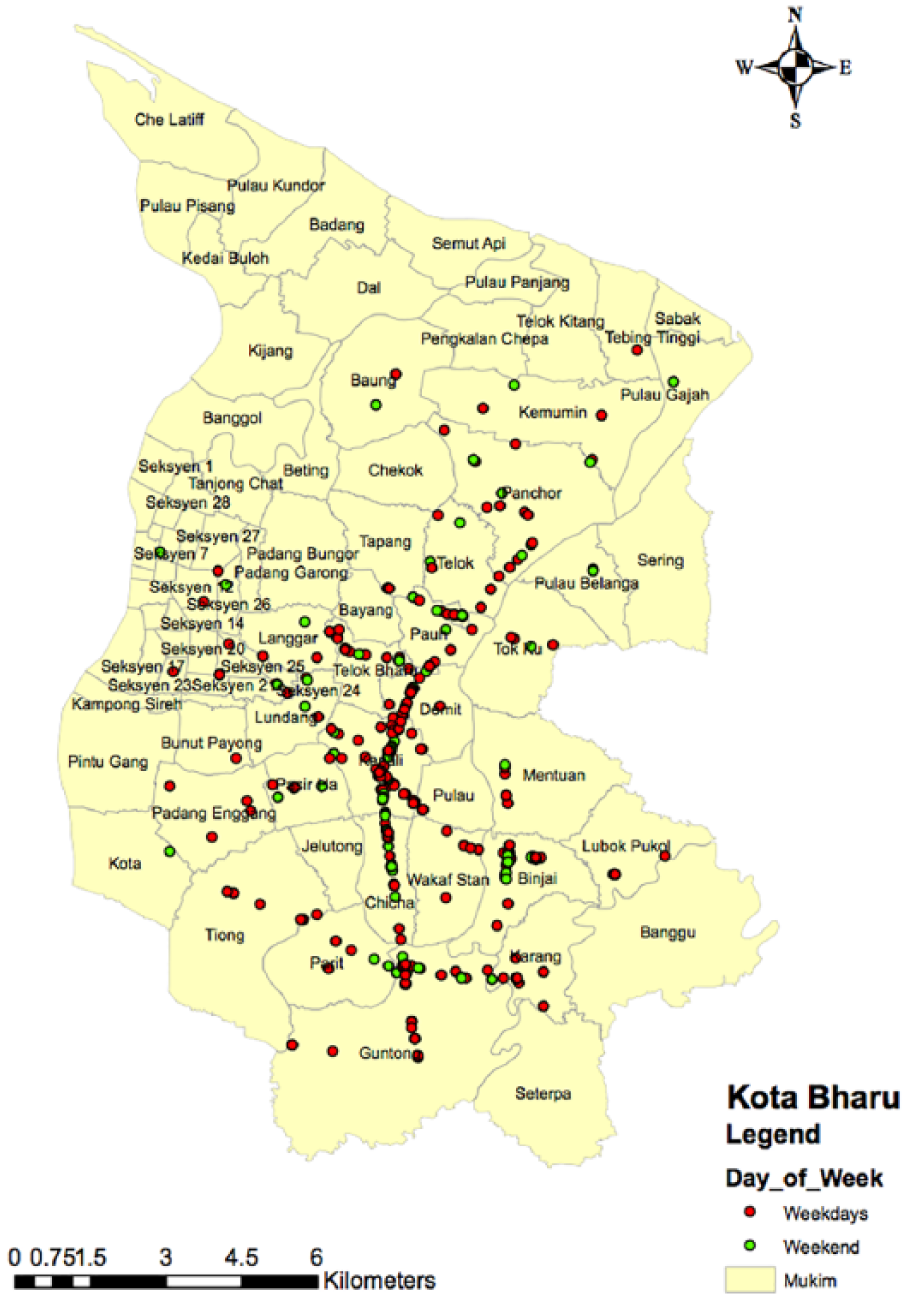
Map of motorvehicle crash locations based on days of the week (borough layer).
Discussion
Injury is one of the common causes of attendance to ED in any parts of the world, in particular in the developing country such as Malaysia. Most of the injured victims worldwide are due to MVC. 12 World Health Organization (WHO) has published the most recent report on global road safety in 2013 and stated that 1.24 million people were killed on the world’s roads annually. 13 According to the Ministry of Health Malaysia data in 2015, injury due to MVC was ranked at the fourth place as the cause of admission to the hospitals and fifth cause of death in the country. 14 The prevalence of the MVC in Malaysia in 2013 was at 25 deaths per 100,000 populations making the country at the highest rank in South East Asia and at the 20th place in the world. 15
As in other middle- and low-income countries, the most common type of vehicle involved was two-wheelers (motorcycles) and cars (80% and 12%, respectively). Numerous other similar findings were published on the risk factors of two-wheeler involvement in the MVC resulting either in severe injuries or deaths worldwide.16,17 Malaysian Institute of Research on Road Safety (MIROS) reported that over the 10-year period (2000–2010), an estimated 1.2%–1.5% of the registered motorcycles in Malaysia involved in accidents. 18 In 2010 alone, of the 120,156 motorcycle accidents, 3614 riders and 422 pillion riders were fatal. This gave the fatality index (i.e. no. of fatalities per road accidents) of 0.03 and 0.003 for riders and pillions, respectively. 19
Although the fatality index for both motorcycle riders and pillions were small, it was significant enough to cause huge losses to the economic output of the country. This was because the majority of motorcyclists consisted of adolescents and young adults, the future contributor to strength of our socio-economic development. In 2015, 50% of the riders who died on the road were 29 years old and below, while the mean age of the pillions who died were 28, and 50% of them were 21 years old and below. 20 In another analysis on motorcycles crashes in Malaysia, Abdul Manan and Várhelyi 21 reported that 22.5% of the fatalities in their study involved riders aged 16–20 years. This age figure of motorcycle users was similarly reflected in this study. Most of the workers in Kota Bharu district are of low and middle-income group who depend significantly on two-wheeler for their daily routine mode of traveling within the town area. This is due to low-cost maintenance and fuel-saving strategy of the road users. In addition, the main reason of using the motorcycle is due to affordability of motorcycles and high cost of cars in the country. As noted from the study data, one-third of the motorcyclists were hit from a side by another vehicle, and there were incidences where the victims skidded and fell off the roads without any involvement of other vehicles or objects. Other mechanisms included frontal impact, hit a fixed object at road-side, hit from back and run off road into ditches. There are so many reasons why motorcyclists are prone to sustain MVC injuries. Motorcyclists are particularly vulnerable to injury, as they do not have the steel car frame to absorb the transmitted forces imparted during a collision.
Another striking issue in our study was the low rate of safety helmet users. Only 40% of the riders and pillions admitted of wearing safety helmets during the MVC. Another quarter of the victims did not disclose whether they were wearing the helmets during the MVC. This finding was almost consistent not only in other parts of Malaysia but also in other developing countries where two-wheelers are common mode of transportation.22,23 Though the helmet wearing alone is not a contributing factor to MVC but the consequence of not wearing the helmet is a more important issue. The trend of not wearing helmet in our society in particular in Kota Bharu is mainly due to road users who ride motorcycles in the suburban areas of the town where the enforcement of the law is lacking. Commonly, the non-helmet wearers ride the motorcycle during the weekend and the early evening just for social ride with friends and family members attending local markets and coffee shops in the vicinity of their home. However, the upsurge of these road users during this time of the week in addition to inadequate experience and another risky method of riding (speeding, multi pillion riders, and illegal racing) has placed them into higher risk to sustain MVC. 24
The trend of MVC was uniform throughout the week with slight peaked during the weekend. This was notably due to more victims spent time freely out of their home rather than at work and schools. More time would be spent on the roads either with the family members or with friends for the purpose of recreational and outings. The common weekend trend in Kota Bharu district depicted the upsurge of people doing outings to the shopping malls, markets, and other outdoor activities. The vehicle density and population density on the road were markedly increased constantly throughout the day and early evening during the weekend and put them at higher risk to get involved in road-related injuries. Unlike during the weekdays, people tend to stay more at their workplace and schools. Another common trend in suburban area of Kota Bharu district over the weekend was the upsurge of people doing outing at local markets especially in the early morning and evening till midnight. There were certain areas within the Kota Bharu districts that were popular for their local markets outing that resulted in marked increase in road users focussing at these areas. Similarly, the increase in vehicle and road user density would result in increased risk of MVC-related injuries in these areas. This finding of weekend effect on the risk to sustain MVC-related injuries was very similar and supported by other studies and surveys in other parts of the world.25,26
The underage motorcyclists and speeding are frequently seen in the suburban and village areas. The enforcement is lacking, and the relative low-density vehicles on the road attract the vehicle users to speed. Many of these vulnerable road users do not wear protective helmets. Futhermore, the distance from the tertiary hospitals results in the delay in ambulance arrival and hence delayed in ED treatment. A study done by Abdul Manan in 2012 on road fatalities among motorcyclist in Malaysia has shown that 60% of the fatalities occurred on the roads in the areas such as suburban and rural locations. They also found that the majority are young riders (89%), 16–20 years old (22.5%), and 90% of the motorcycles are privately owned. 21 Interestingly, the east coast region in Malaysia, with a lower motorcycle population and less built-up density, has the highest fatality rate per 10,000 motorcycles. Meanwhile, the Federal Territories, which have the highest population density, record the lowest rate in motorcycle fatality per 10,000 registered motorcycles. 27 Motorcycle fatality on the primary road accounted for 47% of all death on the road. Striking similarity to this study was found that 66% of all severe injuries cases occurred on straight road. The obvious reason for the severe injuries and high mortality occurring on straight road in Malaysia generally is purely due to speeding.28,29 The less vehicular density at suburban and rural area in addition to speeding and poor attitude of motorcycle riders, have collectively contributed to high risk of sustaining MVC with significant severity.
This study mainly used data from the ambulance services from both Hospital USM and HRPZ within the district of Kota Bharu and utilized real-time clinical data documented by the paramedics and hospital records. The spatial pattern and distribution of all motorcycle-related cases followed the same pattern as the whole MVC cases, since more than 80% of the cases were among the two-wheelers. The distribution showed that most of the motorcycle-related MVC focused on the main municipal roads on the central and southern parts of the town namely the borough of Kenali, Demit, Chica, Teluk Baru, Lundang, Pauh, Binjai, and Guntong. These areas are the main catchment area for the ambulance services that were based in the Hospital USM. The most plausible explanation was due to occurrence of MVC within the areas that contained extensive major road network with high density of road users.30,31 The roads within these areas were the main feeder road network connecting the suburban and the urban areas. Borough Kenali, Demit, Chicha, Teluk Baru, and Lundang can be considered as urban areas with high population, road users, and vehicle density. Whereas borough Pauh, Binjai, and Guntong are the suburban areas with high road user density traveling not only within the area but also to and fro the urban area by using the main municipal trunk road. Borough Kenali is located in the southern part of Kota Bharu that was formerly considered the suburban area of the town. The road network and infrastructure development within the town area expanded as the population of Kota Bharu increased. There was a shift of the center of business and offices toward this area to accommodate the population expansion, and hence the density of road users will also increase. This area contains a major road trunk connecting the center of the town to the other boroughs and the neighboring state. As the density of road users increased, so does the risk of MVC.32,33
This study focussed mainly on the data of RTIs in Malaysia that may have very different geographical factors, type of road users and health-care services. However, the conceptual framework of the study and the methods can be replicated to other cities and localities worldwide in particular for road safety and preventive programs implementation. Many researches conducted worldwide in the field of road safety were based on model developed in developed countries, but still the framework and intentions are replicable to others in different parts of the world.34,35 The GIS utilized in this study can be used by emergency medical services (EMS) agency in any locality to plan for ambulance standby and focuses their catchment areas, hence preparation for severe trauma cases based on hotspot identifications. This will inturn provide the most efficient and predictable responses by the EMS providers.36,37
The investigators had confronted few limitations throughout the study. The main concern was regarding the source of the data variables used in the study. Quality of data is paramount in any population-based research. The robustness of the data at the level of interest determines the ability of geomatics to inform the process of prevention. For this reason, the study had to focus on the data collection mainly based on the prehospital datasheet and hospital case note. Dedicated data collectors and research assistants were appointed for the two EDs merely to oversight the data collection prospectively of all MVC cases attended the two EDs. However, the data collectors also had to obtain some data retrospectively due to the nature of the availability of the information on cases such as post-operative finding, final diagnosis, and outcome at discharge. Even though the GIS application health research has been proven to be very helpful in investigating and preventing the progress of certain diseases, it was not without limitations. Most of the GIS analysis used secondary data sources. The variable data sources might have different definitions and quality. Good example was the data from the police and hospitals. Police may define serious injury differently from the clinicians. In this situation, the investigators has had a predefined taxonomy for all terminology used throughout the study. Finally, using the ARCGIS software by the non-expert such as medical doctors might have contributed to technical limitations. The investigator must learn the jargons and new terms. The investigators have attended the ARCGIS workshop that was conducted by ESRI Malaysia at the Geomatics laboratory prior to the commencement of the research.
The investigator had proven the strong implications for the GIS technologies in RTI research, and it has few remarkable potential uses in the near future in providing information that may influence local and national policy to improve road safety in our country. The investigator had also proven that the use of geospatial technique was feasible in identifying crucial factors related to RTIs at least for Malaysia perspective. The combination of clinical and geographical data clearly elicited a much clearer picture of the injury demography and outcome pattern. The knowledge on geographical factors specifically related to locations within the district that commonly associated with severe injuries and vulnerable road users can be utilized further in future by the local authority to implement the preventive measure such as focus and target group education, that is, among the minors and motorcyclists within the suburban areas in particular originating from the hotspot boroughs such as mentioned above. This new knowledge is also crucial for the enforcement agencies such as Road & Transport Department and Police Force to implement targeted and focused surveillance on road users such as camera installation and speed trap enforcement. This will create a more resource utilization benefit by the authority and avoid unnecessary surveillance and monitoring at areas with low MVC incidences.
Conclusion
This study combined geospatial and clinical data analyses to evaluate the trending among injury-related motorcyclists. Motorcyclists, being male and young age are the vulnerable group of road users commonly injured on our road. The initial geospatial analysis of injury-related MVC cases has shown common hotspot trending along certain roads and borough within the district of Kota Bharu. This new knowledge can be used in the future for preventive and road safety programs in high-risk areas.
Footnotes
Acknowledgements
The author would like to thank the co-investigators who had contributed significantly to the conception of the study, data collection, and writing up of the manuscript. Special thanks to the staff of ambulance services of Hospital USM who had assisted in obtaining the GIS data. The raw data of the research are available by requesting from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Universiti Sains Malaysia, who had granted Research University (RU) Grant (grant no.: 304.PPSP.6316147).
Author contributions
N.H.N.A.R. contributed to the conception and data collection and manuscript writing. N.N.N. contributed in statistical analysis and manuscript checking.
Ethical approval
The ethical approval, consent form preparation and human right protection were presented to and approved by the Universiti Sains Malaysia ethical and review committee and National Malaysian Research and Review (NMRR) committee referenced USMKK/PPP/JEPeM (225.3 (11)).