
Abstract
Introduction
Uttar Pradesh ranks first in India as far as trauma deaths are concerned with 40% of victims under 18 years of age. In spite of such high mortality and morbidity no national portal for trauma registry data exists. This study was conducted to evaluate the profile of injured pediatric patients, to provide baseline knowledge for further research, management and development of pediatric injury prevention programmes.
Methods
A retrospective observational study was conducted in the only Level 1Trauma Centre of the most populous state of India. Children aged less than 18 years of age admitted to the trauma centre were analysed for mechanism, type and severity of injury, the mode of management and outcome.
Result
In a 2 year period 916 children were admitted and their data analysed. Most were boys (73%) and the most common age group was 12–18 years. Half of injuries were caused by road traffic accidents, and blunt injuries were commonest. Blunt abdominal trauma then head injury were the commonest areas injured; 20% of children had life-threatening injuries. Nearly half (47%) had moderate to severe trauma according to the Pediatric Trauma Score. 507 patients (55.4%) were managed conservatively and 409 children (44.6%) required surgery; 657 (71%) were successfully discharged and 39 children (4.25%) unfortunately died.
Conclusion
This study identifies the need for dedicated trauma registries, training of trauma team according to standard operating procedures, the development of paramedical teams for in-the-field management of patients and development of injury prevention programmes according to both age and gender.
Introduction
Trauma and its victims are the subjects of a preventable disease, with children in particular being innocent victims who need special care from paediatricians, pediatric emergency room clinicians, and pediatric trauma surgeons, who must be familiar with the current concepts in trauma care. Road safety continues to be a major developmental issue, a public health concern and a leading cause of death and injury across the world, killing more than 1.35 million globally each year. 1 The World Health Organisation (WHO) Global Status Report on Road Safety from 2018 showed that 90% of road traffic accidents (RTAs) are taking place in developing countries, 1 with India ranking first in the number of RTA deaths across the 199 countries worldwide and accounting for almost 11% of the accident-related deaths in the world. The 2019 Report on Road Accidents in India, 2 lists more than 1.5million accident-related deaths. To address this growing public health problem, there is a need for evidence based research based on relevant and reliable accident data. There is a possible under-reporting of fatalities from police data if death occurs after more than 30 days in hospital because of a lack of linkage between police and hospital records. Accident-related deaths are the eighth leading cause of death overall and the greatest cause of death among children aged 5–14 and adults aged 15–29. 1 Globally, 54% of accident-related deaths are pedestrians, cyclists and motor cyclists, resulting in considerable economic losses not only to individuals, their families, but also to the nation as a whole on account of the costs of treatment as well as lost productivity for those killed or disabled by their injuries and the loss of productivity of family members who need to take time off work to care for the injured.
Despite such high mortality and morbidity no national pediatric trauma registry exists in India, nor in the majority of countries worldwide; this absence of basic pediatric trauma epidemiology prevents the establishment of dedicated pediatric trauma centres. The epidemiology of pediatric trauma continues to be a challenge in India and specifically in Uttar Pradesh, which ranks third in India for number of road trauma cases and first for accident-related deaths, with children less than 18 years accounting for a significant proportion. 2
King George Medical University (KGMU) is Level one trauma centre in Northern India catering for a large number of pediatric trauma cases from both Uttar Pradesh and the neighbouring states of Bihar, Rajasthan and Uttarakhand. This study aimed to evaluate the profile of injured pediatric patients to provide baseline knowledge for further research, management and development of pediatric injury prevention programmes.
Methods
This is a retrospective observational study carried out in a high volume Level I trauma centre in Northern India from January 2018 to December 2020. Inpatient data of all children aged less than 18 years of age admitted to the trauma ward during the study period were collected on a standard proforma. Data regarding age, gender, mechanism of injury, type of injury, findings of primary and secondary survey, type of treatment given (conservative /operative), results of investigations, outcome of patients and duration of stay in the hospital were recorded. The children were classified according to age as: early childhood (1–6 years), mid-childhood (6–12 years) and adolescents (12–18 years). Modes of trauma were divided as falls, RTA, burns, assault (penetrating or blunt), machine injury and railway track injuries. Types of injury were subdivided: orthopaedic injuries, burns, blunt trauma (head and neck/abdomen/chest), penetrating trauma (chest/abdomen/head and neck) or polytrauma. The Pediatric Trauma Score (PTS) was used to calculate the severity of trauma - severe (PTS <5), moderate (PTS 6–8) and mild (PTS 9–12). 3 The data were analysed using SPSS version 25 and summarised as percentage, median and means. This study was granted Institute Research Board (IRB) official waiver of ethical approval as it was retrospective analysis of ordinarily collected clinical data.
Results
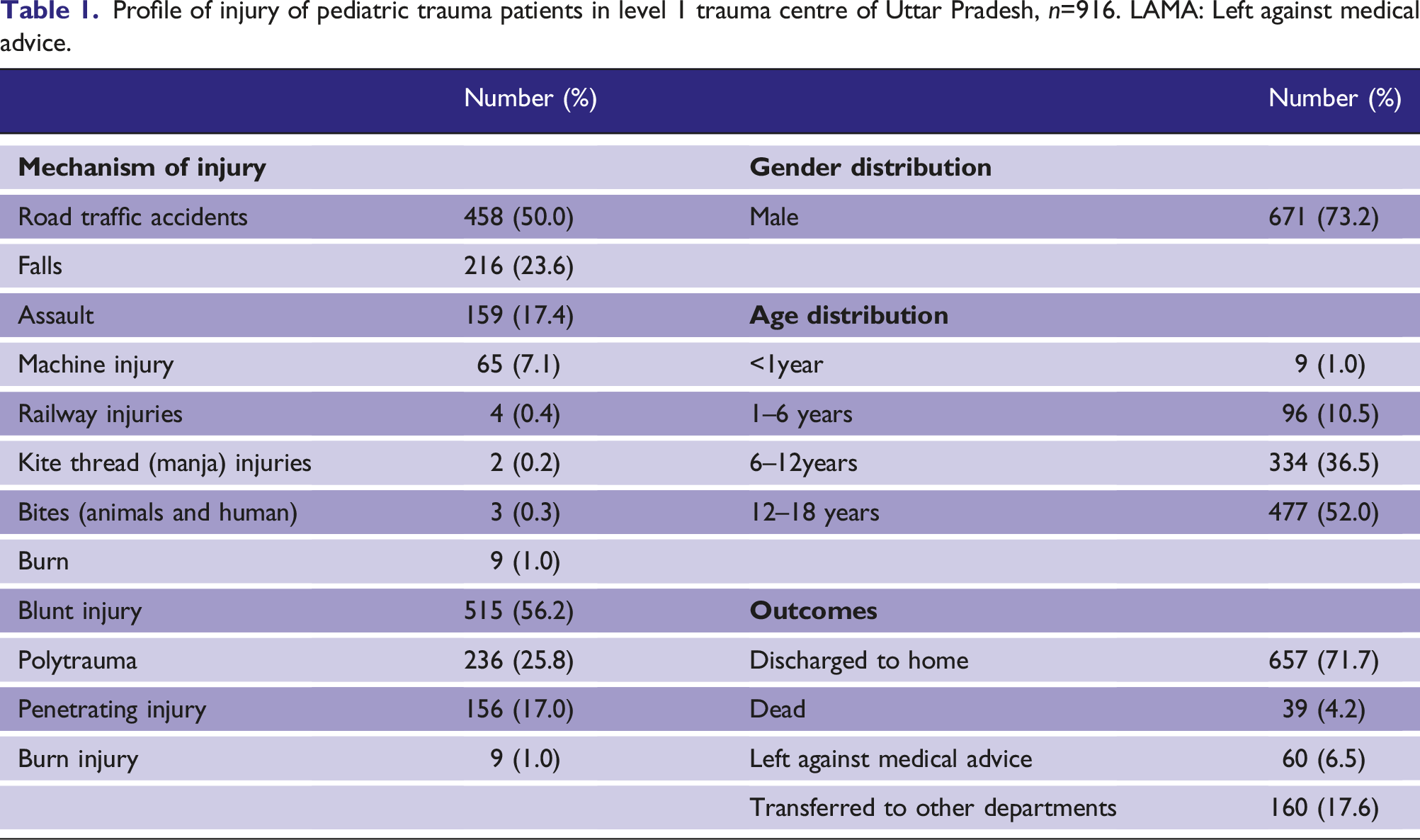
Profile of injury of pediatric trauma patients in level 1 trauma centre of Uttar Pradesh, n=916. LAMA: Left against medical advice.
Mechanisms of injury, types of injury, severity and outcome among children aged 0–18 years.
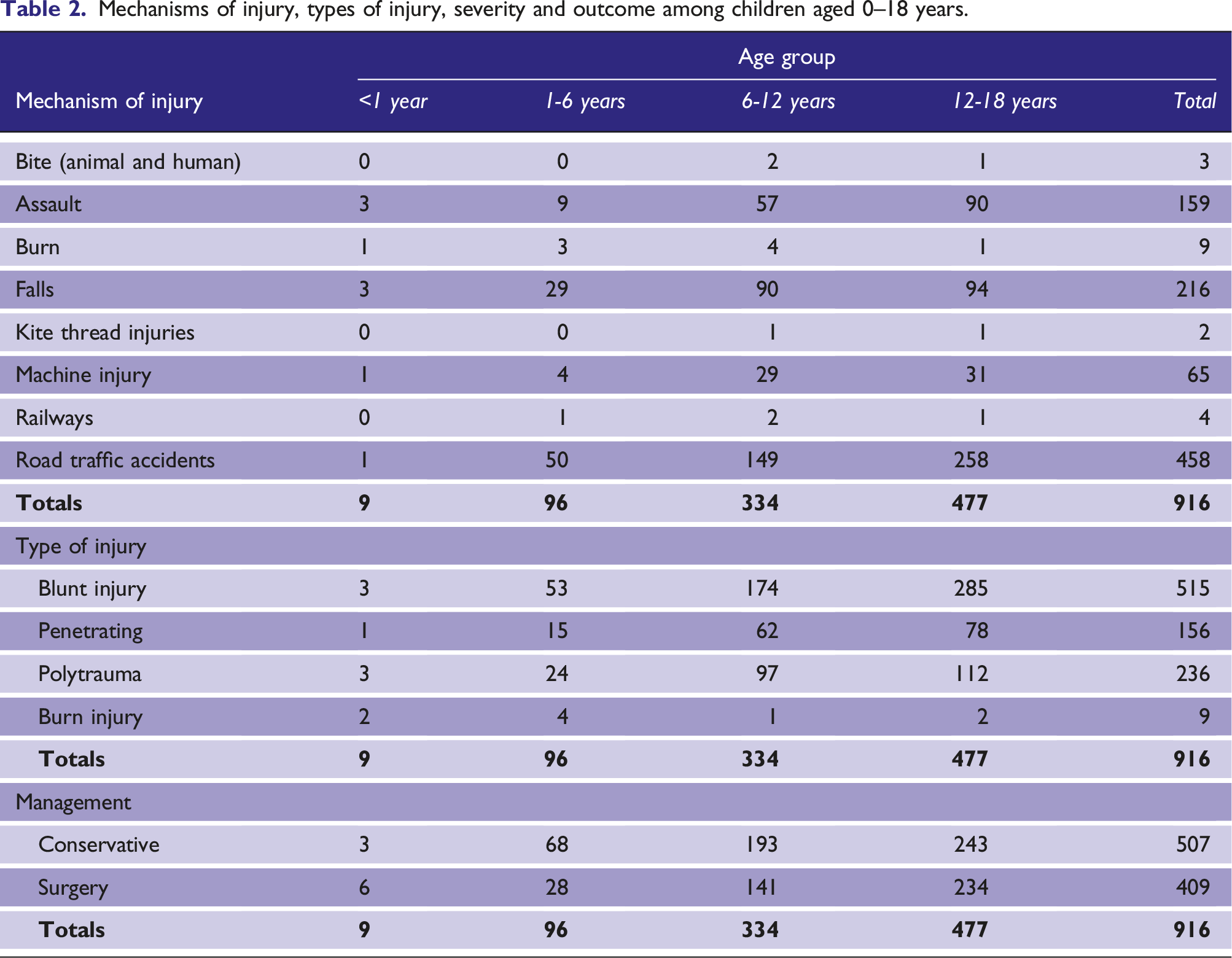
Mechanism and pattern of trauma
The most common mechanism of injury was RTA followed by falls and then assault 154 (16.81%) According to the Pediatric Trauma Score most of the injured children had mild trauma (n = 473; 51.6%); 321 (35%) children had moderate trauma and 122 (13.3%) had severe trauma. Blunt injury was commonest (515 children (56.22%)) followed by polytrauma (236 children (24.24%)). The most common body part injured was the abdomen (275 children), followed by head (119 children), with isolated orthopaedic injuries noted in 198 (21.6%) children. Two children had cut throat injury from manja (kite thread) and three had thoracoabdominal lacerations from wild animal attacks (1 Tiger, 2 Leopard) in the neighbouring forest areas of Pilhibhit.
Management
During primary survey, life threatening injuries were identified in 182 children (19.8%) with Focused Assessment Sonography in Trauma (FAST) positive in 275 (30%) patients. One child had hepatic lacerations detected on Contrast Enhanced CT Thorax (CECT Thorax) but missed by FAST. Of the 276 children with blunt trauma abdomen, 167 (60%) had liver injuries, 106 (39%) splenic injuries and three had both liver and splenic injuries. Overall, (70%) of the blunt abdominal trauma was managed conservatively, with 80 children requiring surgical intervention as well as 81 with penetrating abdominal injury. In total, 507 patients (55.4%) were managed conservatively and 409 children (44.6%) required some kind of surgical intervention.
Outcome
The outcomes for the 916 children are shown in Table 1, with 657 discharged home. Unfortunately 39 children died – 16 from haemorrhagic shock, 13 from sepsis and its complications and 10 from respiratory failure.
Discussions
Over the next decade pediatric trauma will become a major cause of concern worldwide and in India; the lack of proper infrastructure, appropriate standard operating procedures and pediatric trauma team training will further worsen outcomes. Currently India, and particularly the state of Uttar Pradesh has the worst data as far as number of cases and outcome of admitted patients is concerned. 2 KGMU is currently the only apex trauma centre in the state and it is also the nodal centre of trauma training in India with a high rate of pediatric trauma patients as all pediatric patients requiring trauma care in and around the state of Uttar Pradesh are referred here.
In the absence of any baseline data this study was planned to outline the basic epidemiology and patterns of injury in this patient group. More than half of our patients were above 12 years of age similar to a trauma center in New Delhi, 4 but in contrast to a Southern Indian study where the commonest age group was 1–6 years 5 This study showed a male preponderance with nearly two thirds of our patients being male, similar to other published literature4–7 suggesting males are most likely to be affected by RTA compared to females; a study on gender effects in young road users on road safety attitudes, behaviours and risk perception identified the need of gender-based prevention programmes. 8
Nearly 45% of admitted patients were referred to our centre from neighbouring districts and almost one fifth had life-threatening injuries on admission suggesting that delays in resulted in fatalities; thus there is an urgent need to develop paramedical teams, trained to, ATLS protocols so as to identify life-threatening injuries on field and secure them before transport. The most common mechanism of injury in our patients was RTAs – one study found domestic accidents to be commonest, 9 but the majority of published literature confirm RTA as the predominant mechanism of injury.3–6,10 Likewise, ‘fall from height’ was another significant mechanism of injury, in keeping with most other studies from India;4,6,7,11 three of the nine traumas under 1 year of age were falls.
When road safety programmes are developed for children, particular attention to falls and its prevention needs to be emphasised; further policies such as well-fitting helmets for child cyclists should also be emphasised. Unlike more developed nations where wearing of helmet is mandatory for children of all age groups, whether riding a bicycle or simply as an occupant of a two wheeler, India has no such guidelines or regulations. Due to lack of knowledge, parents are carrying children in two or three wheelers without adequate protection, resulting in a high incidence of falls; injury to a child’s developing brain can have both short term and long term damage and the head was the second most commonly injured body area in this study.11,12
Blunt abdominal injury was the most common type of injury and liver was the most affected organ. Data from developed nations like the USA have shown a high incidence of RTA death in children who are not restrained in their cars. In 2019 alone, 600 children aged less than 12 years died in RTAs and more than 91,000 were injured; 38% of those who died were not appropriately restrained in their cars. 13
In India, the use of seat belts for children in road vehicles is infrequent, with the movement of children on both rural and urban roads often unsupervised, making this population more vulnerable to accidents, thus appropriate restraints in cars and the use of helmets on two-wheelers must be used on every road trip; to avoid the short and long term consequences of serious injury in childhood, which are generally greater than in adults any future road safety protocols must place due emphasis on child safety measures.
There was a significant number – almost half of those admitted - with moderate to severe trauma cases, potentially because KGMU is the only level 1 Trauma Centre in the state and a large number had life-threatening injuries. KGMU medical and paramedical staff are ATLS trained, and the unit is a trauma training centre and the outcomes, despite the influx of severe trauma were good, with only a 4% mortality rate – which is comparable to another Northern Indian Level 1 Trauma Centre, but better than those reported elsewhere in India5,7,13,14 suggesting that the nationwide adoption of our trauma training and protocols, adapted to local community needs, could be of benefit. 15
Conclusions
The results of this study suggest a number of areas for improvement in the management of injured children across India including the need for dedicated trauma registries, trauma team training according to standard operating procedures, development of paramedical teams for in-field management of patients and development of injury prevention programmes according to both age and gender. This study also emphasises the need for the nationwide study of epidemiology pattern of injuries in children, as unless such data are available no proper planning and implementation of trauma prevention and injury programmes can be possible.
Footnotes
Acknowledgements
All residents working in trauma unit.
Contributorship
NT, VJ, AS, NK, MM, ST, SM, DS and YD drafted the initial manuscript, and reviewed the literature revised the manuscript and did the statistical analysis and drafted the manuscript. All authors have approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Prof Samir Misra, National ATLS Course Director, Prof and incharge Trauma centre, KGMU. Email: