
Abstract
Background:
An objective, comprehensive and scientific evaluation of emergency medical rescue capability (EMRC) is of great realistic significance in assisting the health administrative department to grasp the overall response capability of all emergency medical rescue teams, enabling each team to have a full understanding of its own strengths and weakness and improve itself accordingly. At present, the research on the evaluation of EMRC in Hazardous Chemicals Accidents (HCA) is not systematic and in-depth, and the existing research results also have some shortcomings, such as, the lack of strong theoretical support for the evaluation index system, the relatively single function of evaluation methods, and so on.
Objectives:
The objective of this article is to research the evaluation index system and a new evaluation method of EMRC in HCA to overcome the above shortcomings.
Methods:
It establishes an emergency medical rescue capability model by employing the competency model and then constructs the evaluation index system on the basis of the analysis of all the factors of emergency medical rescue capability in hazardous chemical accidents and sets up an evaluation model based on the theory of connection numbers and partial connection numbers. It determines the competence ranking of several emergency medical rescue teams and the competence state of an individual emergency medical rescue team by calculating the connection principal value, and it also predicts how the emergency medical rescue capability will develop based on the values of partial connection numbers.
Results:
The example shows that the calculation process of this model is relatively simple, and its assessment results are objective and authentic, and moreover, its multi-functions can make up for the deficiency of the simplified function of other evaluation models.
Conclusion:
This method is scientific and rational to some extent and can provide reference for evaluation problems of the same kind.
Keywords
Introduction
Emergency medical rescue for hazardous chemical accidents (EMRHCA) refers to all the professional acute rescue work in the event of hazardous chemical accidents (HCA),1,2 such as fires, explosions, leakages, poisoning, asphyxiation, burns, and radiation. 3 The EMRHCA includes efficient emergency treatment, disease control and prevention, and hygiene supervision by comprehensively applying different health technologies and medical methods,1,2 aiming to minimize the life and health hazards of the affected population; reduce the rates of injury, disability and mortality; and maintain their physical and mental health. HCA typically have characters of great suddenness, high perniciousness, wide spreading, and far-reaching subsequent consequences. In order to scientifically and efficiently carry out the HCA rescue, China has established chemical accident rescue centers across the country, built up national health emergency response teams, and specified the HCA-rescue-related provisions and requirements. Due to the high incidence of HCA in recent years, especially the occurrence of several major and serious accidents, there has been a constant increase in the demand for quality of EMRHCA from all levels of Chinese society. Therefore, an objective, comprehensive, and scientific evaluation of emergency medical rescue capability (EMRC) is of great realistic significance in assisting the health administrative department to grasp the overall response capability of all EMR teams, enabling each team to have a full understanding of its own strengths and weakness and improve itself accordingly, and building up the confidence of the general public in EMRHCA.
In review of recent literatures, there is an overall lack of enough investigations, especially systematic and in-depth studies on capability evaluation of EMRHCA. The insufficiency of the previous research is mainly manifested in the following three aspects. First, most of them are one-dimensional studies, and relatively few studies are on the integration of medical rescue and HCA. Some of them are based on the overall analysis of emergency rescue capability (ERC) from the perspective of “big rescue” for HCA, the medical rescue features of which are not prominent. Some studies are about EMRC for all types of emergencies, which are not fully applicable to HCA. For instance, in Wang et al., 4 the elements of technical capability in the EMR were analyzed and elaborated from seven aspects. In Zhang et al., 5 a three-level index system was set up for EMRC based on the theory of analytic hierarchy process (AHP), and the EMRC of all teams were evaluated according to the index weight at all levels determined by the experts’ rating. Dai et al. 6 studied the evaluation and sorting of the EMRC of the disease control and prevention institutions in the 22 districts. Second, in all the previous evaluation index systems, “capability” was not closely related or emphasized, and their theoretical basis seemed insufficient, or not strong enough, or too subjective, or even attached with strong administrative color. For example, in Cheng 7 and Wu, 8 relatively rational competence evaluation index systems were proposed for the national EMR teams of the Chinese People’s Liberation Army (CPLA) and the mobile medical units of Corps Hospital of Armed Police Force in antiterrorist operation, respectively. However, such systems are very subjective and poorly theoretically supported, as it was mainly acquired through expert consultation, and thus lacked the systematic analysis of index sources. In Zhang et al., 9 an evaluation index system was established for the health emergency capability of Xinjiang Production and Construction Corps. However, similar to the systems in Cheng 7 and Wu, 8 it was not scientific enough, as it was obtained mainly based on public administration, and there are inadequate discussions about the “competence” itself. Third, the functions of the evaluation methods employed in previous studies were usually simplified. The methods applied in the evaluation of the existing EMRC can be classified into two types: (1) preferred election through comparative evaluation (Type I) and (2) self-evaluation and orientation (Type II). The first method (Type I) aims to select the best and set a model on the basis of comparative analysis of several EMR teams. For example, in Dai et al., 6 the health emergency response capabilities of the disease control and prevention institutions in the 22 districts were evaluated, ranked, and studied by comparing the AHP and entropy methods. While in the second method (Type II), each individual EMR team was studied and evaluated to determine its competence ranking. In Cao et al., 10 for instance, about 104 health units were evaluated individually in a comprehensive manner to determine their rankings of health emergency capacity. So far, little researches have been done on developing a capability evaluation index system which can combine the advantages of both Type I and II methods.
This article aims to extend the well-known competency model (CM) 11 to the field of EMRHCA, establish an evaluation index system, and seek its theoretic support by analyzing all the constituent factors in EMRC. In this article, by taking into consideration all the certainties and uncertainties in the process of evaluation, a mathematical model based on connection numbers (CN) and partial connection numbers (PCN)12,13 is established for the assessment of EMRC in HCA, and the competencies of the EMR teams are evaluated quantitatively and reflected objectively, thus realizing the integration of “prioritized selection” and “self-orientation” and identifying the trend of EMRC in the future.
Methods
EMRC Evaluation Index System on the basis of CM
As stated in the theory of the CM, 11 a competence, in essence, is collection of resources and the property that a resource collection displays in fulfilling a task. It is also clarified that a clear description of a competence should involve its associated tasks and resource collection. The two aspects interrelate with each other and constitute a competence entity, which displays certain capabilities. And a competence itself can become the component of another competence.
As defined, the core tasks of EMR are first aid, disease control and prevention, and hygiene supervision. According to the characteristics of HCA as well as the demands and general procedures in EMR, the three core tasks can be subdivided into the following six aspects: emergency response, investigation and supervision, decontamination and protection, grading treatment, medical supply and equipment support, and survival guarantee. The six tasks correspond with the six links in the rescue process, which intertwine, interfere, and interact with each other. Meanwhile, they also represent the six essential competences in EMR, namely, the competences of emergency response, investigation and supervision, decontamination and protection, grading treatment, medical supply and equipment support, and survival guarantee.4,5,14 Furthermore, the resources in support of EMRC in HCA consist of the elements of manpower, material resources, financial resources, information, spirit, and corresponding system. Similar to the six tasks, these elements intertwine, interfere, and interact with each other and restrain the generation and development of EMRC.
Combining with the most recent frequent major and serious HCA of different types and the associated EMR practices in China, such as the pipeline explosion in Qingdao, Shandong, on 22 November 2013, the extraordinarily serious fire explosion at Tianjin Port on 12 August 2015, the explosion of Sinopec at Linyi, Shandong on 5 June 2017, and taking into full consideration of the characteristics of HCA and the competence requirements of EMR as well as all the influencing factors and their interactions, a CM was specially constructed for the EMRHCA, as illustrated in Figure 1.
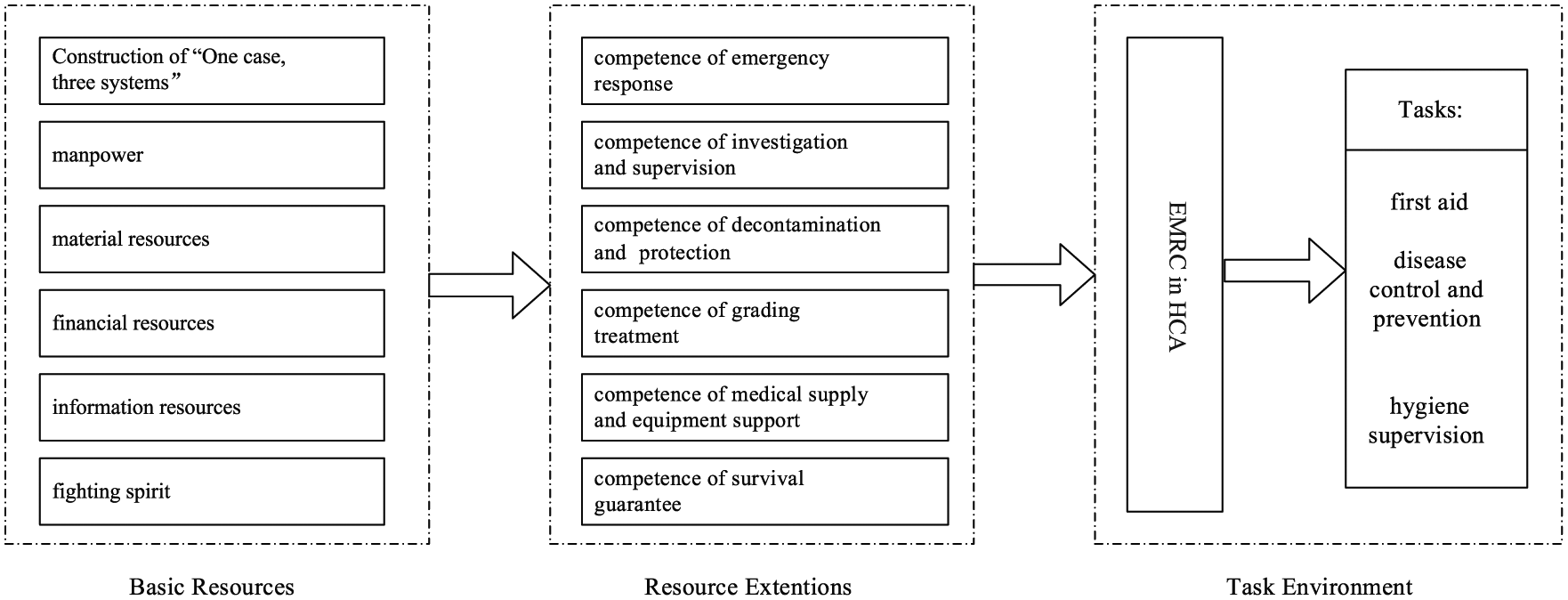
Competency model for EMRHCA. (“One case, three systems” is an emergency management system with Chinese characteristics, where “one case” means emergency plan, and “three systems” refers to emergency management system, emergency management mechanism, and emergency management legal system.)
A capability evaluation index system can then be set up for EMRHCA with further detailed analysis of all the components in the model, as shown in Table 1.
Capability Evaluation Index System of EMRHCA.
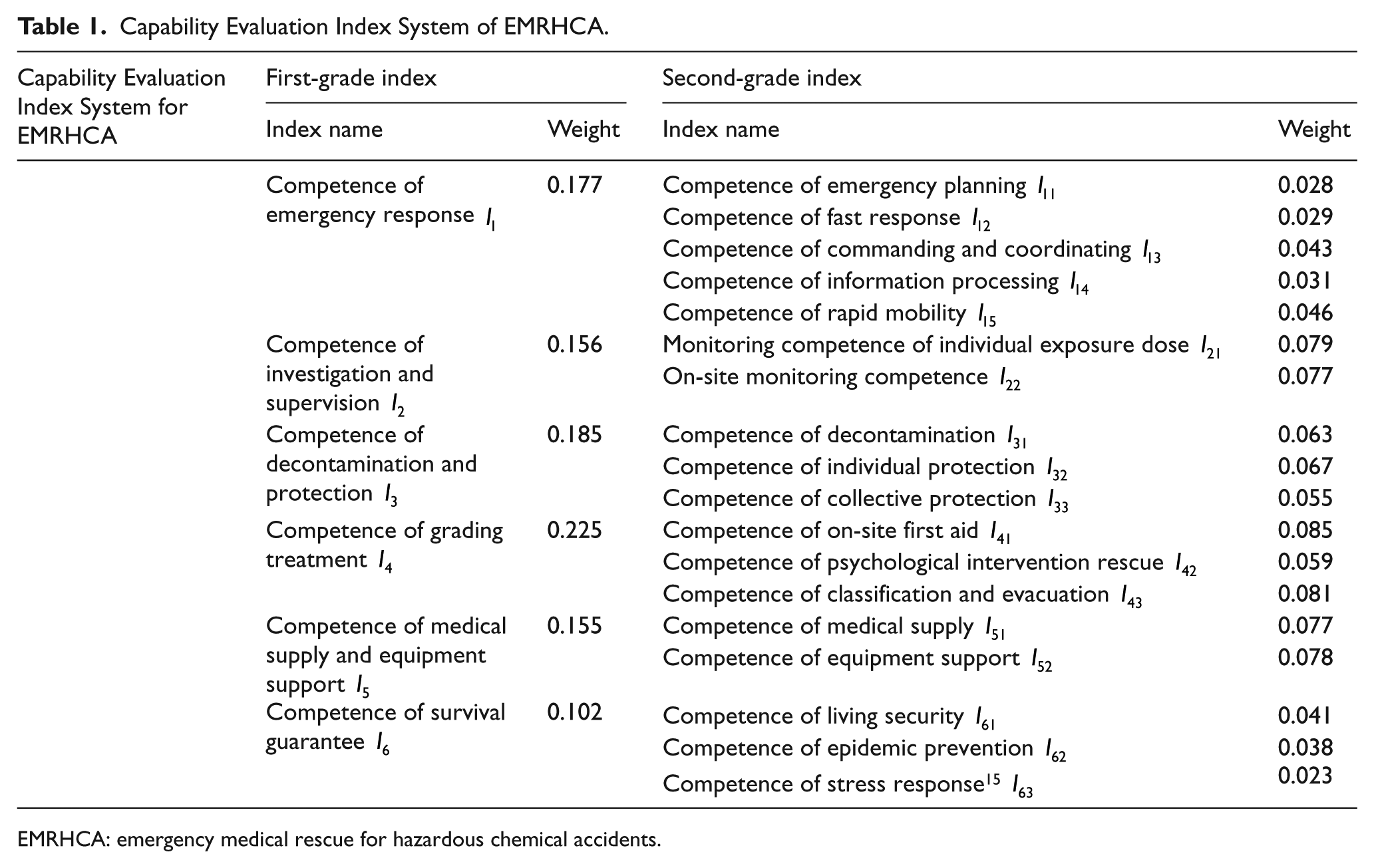
EMRHCA: emergency medical rescue for hazardous chemical accidents.
EMRHCA capability evaluation model based on theory of CN
Theory foundation: CN and PCN
The theory of connection numbers (CN) was developed from the set pair analysis (SPA).
16
It is based on the concepts of universal connection and “one divided into three” (as a unity of contradictions, things not only include two aspects of contradiction and contradiction, but also the third party that plays a key role in the unification and transformation of the two parties) and describes problems by using logical unit set pairs. It gives a universal description and expression of identified and unidentified relations using connection numbers by means of dialectical identity–discrepancy–contrary (IDC) analysis12,13 and conducts a universal study on the uncertainty problems from the macroscopic and microscopic perspectives. The basic concepts of the CN theory are set pairs and connection numbers. The set pair, also the logic unit of the CN theory, refers to Set A and Set B connected with each other or the set pair consisting of internal elements, denoted as
Four-element connection numbers (FECN) can be regarded as an extension of three-element IDC connection numbers, 13 with the general formula of

where µ represents FECN (degree), and a, b, c, and d are the identification degree, pro-identification degree, pro-contrary degree, and contrary degree, respectively. Typically
As a key associated connection number, PCN reflects a potential paradoxical movement and its interlayer migration trend of the objects described with connection number at micro level. 17 The PCN of FECN is 13

in which


Substituting equations (3) and (4) into equation (2), the PCN can be recast into the following formula

When
Step 1. Mathematical description of the problem
For the convenience of narration and calculation,
The EMRHCA capability evaluation can be converted into a mathematical problem:
18
by setting up a mathematical model, relevant calculations are made about evaluation matrix
Step 2. Determining the connection component matrix of individual evaluation index
The connection component matrix of individual evaluation index of the EMR team
in which
Step 3. Determining the connection number of total index
The connection number of total index of the EMR team

in which

is the connection component of the total index of the EMR team
Step 4. Ranking of evaluation, determination of the comments, and development trend
1. To rank the evaluation by calculating connection principal value
For the convenience of calculation and evaluation, based on the “principle of equipartition,”
20
the values of i and j should be located on the nodes of trisection within the interval of

Then, the capability of each EMR team will be evaluated and ranked according to its
2. To determine the comment grade by calculating connection principal value
Divide
3. To analyze the development trend by calculating PCN
By calculating the PCN
Discussion
Assuming that the evaluations are carried out on the EMRC of EMR teams A and B in one particular HCA, for the convenience of calculation, the three evaluation experts
Calculations are made in the following steps:
Step 1. The connection component matrices
Step 2. The FECN of total indices is determined using equations (8) and (9) based on the index weights as illustrated in Table 1

Step 3. The connection principal value can be calculated with equation (10)

Obviously,
Step 4. From equation (5), with
Results
As illustrated in example analysis, the capability evaluation model of EMRHCA established in this article is scientificity and rationality to some degree, as it can be used not only for the evaluation and comparison of the capabilities of several EMR teams but also for the grade evaluation of the capability of an individual EMR team, thus making up the deficiencies of functional simplicity of the other existing evaluation methods. Besides, this evaluation model is able to analyze the capability development trend of EMR through the calculation of PCN, thus providing valuable references for the long-term construction of EMR teams and leadership decision making in the relevant field.
Conclusion
This article attempts to build a capability evaluation index system of EMRHCA by using the theory of CM, which can better solve the problems of insufficient theoretical support when constructing capability evaluation index system in the past and also provide a reference in ideas and methods for other similar problems.
With the features of relatively strong operability, simplified model, and convenient calculation, the present model are relatively in line with the capability evaluation practice of EMR in China at present. It is conducive to the full playing of the expert consultation of the committee of experts and is also able to realize the quantitative calculation of qualitative comments made by the experts. In case of the multiplied increase of calculation workload in the model as the result of the large number of experts, a computer evaluation system can be developed in practice to assist the decision making.
This method is still in the stage of theoretical discussion, and its effectiveness and feasibility remain to be further verified and improved in the future practice. All the index data in this article are acquired through the method of expert rating. Despite its ease in the operation and control, the method has the disadvantage of strong subjectivity and is susceptible to the influence and restrictions of the knowledge, capacity, experience, and personal preference of the experts concerned, thus probably impacting the accuracy of evaluation results. Therefore, the in-depth research in the data collection and its quantitative processing of evaluation indexes is to be further strengthened in the future, so as to realize the objectivity and quantitativeness of evaluation.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of the relevant researchers in the Department of Demonstration and Evaluation of Medical Support System, Institute of Medical Service Support Technology, Academy of System Engineering Research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Research and Development Program of China (2017YFC0806400).
Availability of data and materials
The main purpose of this paper is to explore a new multi-objective evaluation method. Data are important but not the core of this study. The data involved in this paper are all sample data, not real data, which are used to explain the specific application of the evaluation method. The weight of the index system in ![]() is generated randomly by computer. The data in the evaluation matrix (in discussion) are obtained by expert consultation, and all the original data are given in this paper. In practice, we can use the multi-objective evaluation method proposed in this paper to evaluate the actual case according to the collected real data.
is generated randomly by computer. The data in the evaluation matrix (in discussion) are obtained by expert consultation, and all the original data are given in this paper. In practice, we can use the multi-objective evaluation method proposed in this paper to evaluate the actual case according to the collected real data.
Informed consent
Written informed consent was not necessary because no patient data has been included in the manuscript.