
Abstract
Patients with right upper quadrant pain are commonly encountered in the emergency department. The causes of right upper quadrant range from infection or inflammation to malignancy. Thus, prompt and accurate diagnoses are essential in the emergency department. However, vicarious excretion of contrast media via the gallbladder, presenting as right upper quadrant pain, has been rarely reported and is not well known. The present case is instructive because gallbladder opacification is often considered a pathologic condition in patients with right upper quadrant pain. Although vicarious excretion via the gallbladder is uncommon in patients with right upper quadrant pain, inaccurate or delayed diagnoses may prolong hospitalization and increase medical costs due to unnecessary and invasive diagnostic procedures.
Keywords
A 24-year-old woman presented to our emergency department (ED) with a 3-day history of right upper quadrant (RUQ) pain. The pain began as a day of intermittent squeezing in the RUQ, migrating to the right lower quadrant (RLQ); she also reported four episodes of diarrhea. Otherwise, her medical history was unremarkable. She had been tentatively diagnosed with colitis at a different hospital and empirically treated with antibiotics and hydration. When her clinical presentation did not progress, she was transferred to our ED. Upon arrival, her blood pressure (120/75 mmHg), heart rate (110 beats/min), respiratory rate (22 breaths/min), and temperature (38.5°C) were measured. Her abdomen was soft and had normoactive bowel sounds; there was RUQ and RLQ tenderness, without guarding or rebound tenderness. Murphy’s sign was positive. Except for her C-reactive protein (6.8 mg/dL) level, her laboratory findings and liver function tests were within normal ranges. Abdominopelvic computed tomography (APCT) on admission (Figure 1) and endoscopic ultrasound (EUS) (Figure 2) on hospital-day 2 were obtained.
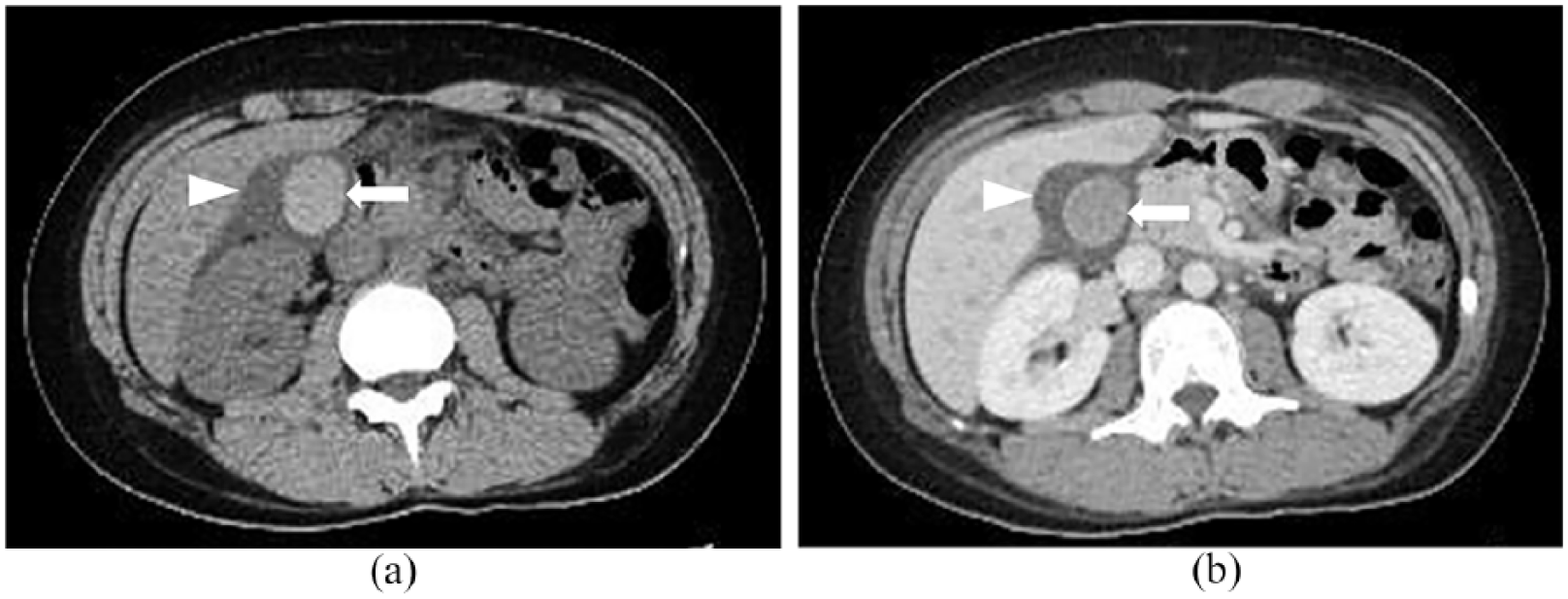
Pre-contrast (a) and post-contrast (portal phase) (b) CT images show an ovoid, smooth-margined, high-attenuated lesion is shown in the gallbladder (arrows, (a) and (b)). A concentric low-attenuated lesion around the gallbladder (arrowheads, (a) and (b)) is also seen, indicating gallbladder wall edema.
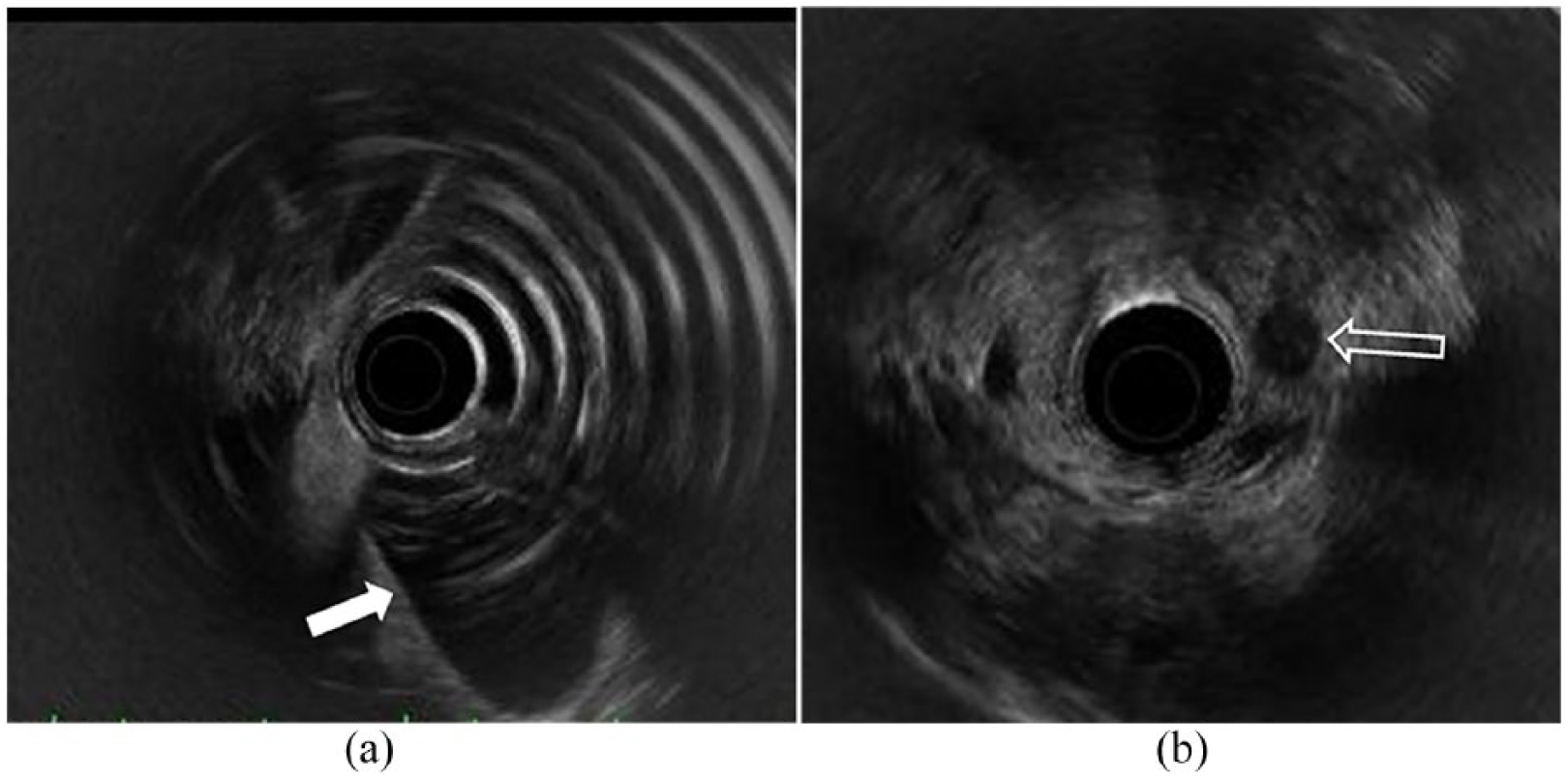
EUS ((a) and (b)) images show no evidence of sludge or stones in gallbladder (arrow, (a)). Also, no evidence of intra-duct stone, dilatation, or wall thickening on common bile duct (open arrow, (b)).
Questions
Answers
Pre-contrast (a) and post-contrast (portal phase) (b) CT images show an ovoid, smooth-margined, high-attenuated lesion is shown in the gallbladder (arrows, (a) and (b)). A concentric low-attenuated lesion around the gallbladder (arrowheads, (a) and (b)) is also seen, indicating gallbladder wall edema.
EUS ((a) and (b)) images show no evidence of sludge or stones in gallbladder (arrow, (a)). Also, no evidence of intra-duct stone, dilatation, or wall thickening on common bile duct (open arrow, (b)).
The diagnosis was vicarious excretion of contrast media via the gallbladder.
Discussion
RUQ pain is a commonly encountered complaint in the ED. 1 The pain may be due to inflammation (e.g. acute cholecystitis, acute pancreatitis, cholelithiasis, hepatitis, liver abscess), hepatobiliary vascular problems, or malignancy. Thus, a prompt and accurate diagnosis is essential. 1 However, vicarious excretion of contrast medium via the gallbladder, presenting as RUQ pain, is rarely encountered.
Generally, contrast medium is excreted via the kidney. Vicarious excretion involves contrast medium being excreted via other organs, including the stomach, small intestine, or gallbladder.2,3 Few cases of vicarious excretion via the gallbladder have been reported, 4 but several recent reports have suggested that vicarious excretion via the gallbladder occurs in patients with cholelithiasis. Vicarious excretion via the gallbladder is relatively common after intravenous contrast medium injection and may present as gallbladder opacification in delayed plain radiographs or APCT. 2 Bile, an enzymatic secretion made by hepatocytes, is modified by the bile duct epithelium and flows through the interlobular septa to the common bile duct; it is concentrated in the gallbladder, resulting in gallbladder opacification. 5
In our patient, we believe that the contrast medium was excreted through the biliary system, remained in her gallbladder after the first APCT scan, and became increasingly concentrated due to her fasting state and lack of gallbladder emptying. Moreover, aggressive hydration may have resulted in the periportal edema and gallbladder wall edema. Eventually, the concentrated contrast may have resulted in gallbladder distension that mimicked acute calculous cholecystitis and caused her biliary colic. This aggravated her RUQ pain and positive Murphy’s sign, without causing abnormal laboratory findings. Careful medical history-taking and prompt diagnostic imaging are essential to prevent harming patients. Indeed, in this case, our patient underwent unnecessary examinations and an invasive procedure (EUS).
The radiological finding of the vicarious excretion of contrast media via the gallbladder differed from that associated with typical acute calculous cholecystitis. First, there was relatively low attenuation (40–50 HU) compared with gallbladder stones (>60 HU); possibly because the contrast medium was mixed with bile secretions. Second, the “lesion” demonstrated smoother margins than are typical for gallbladder stones, and its shape was more ovoid than is typical gallbladder sludge. We believe the lesion would have disappeared in any follow-up imaging. Radiation hazards are always concerning to emergency physicians, and we recommend point-of-care ultrasound in cases with similar clinical presentations.
The present case is instructive because gallbladder opacification is often considered a pathologic condition in patients with RUQ pain. Although vicarious excretion via the gallbladder is uncommon in patients with RUQ pain, inaccurate or delayed diagnoses may prolong hospitalization and increase medical costs due to unnecessary and invasive diagnostic procedures. Thus, ED physicians need to keep in mind the mechanism of vicarious excretion via the gallbladder and approach potential patients appropriately.
Footnotes
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required as no patient’s identifiable data were disclosed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.