
Abstract
Background:
Leukocytosis is a common laboratory finding in emergency departments worldwide. Various infectious diseases are common causes of leukocytosis in hospitalized adult patients. Most emergency physicians have a high awareness of sepsis or severe infection, which requires empirical antibiotics. However, there are many other etiologies for leukocytosis. The outcome of prescribing broad-spectrum antibiotics in the emergency department for leukocytosis patients is not well-understood.
Objectives:
Our objectives were to determine whether prescribing antibiotics in the emergency department affect outcome for hospitalized adult patients with leukocytosis.
Methods:
A retrospective cohort study of hospitalized adult emergency department patients with leukocytosis was conducted in a tertiary hospital in Taiwan between June 2016 and June 2017. Patients with leukocytosis (white blood cell count >11,000 cells per μL) who were admitted via the emergency department at the Kaohsiung Veterans General Hospital, from June 2016 to June 2017 were enrolled. Patients aged ⩽18 years, pregnant women, those who received prophylactic antibiotics prior to operation, and those with a final diagnosis of hematologic malignancy were excluded from this study. The primary outcome measure was hospital stay, and the secondary outcome measure was mortality. All collected data were statistically analyzed.
Results:
A total of 8054 hospitalized adult patients with leukocytosis were included (the exclusion criteria included patients aged ⩽18 years, pregnant women, those who received prophylactic antibiotics prior to surgery, and those with a final diagnosis of hematologic malignancy); all patients were admitted via the emergency department. In all, 4486 patients received initial antibiotic treatment in the emergency department, whereas 3568 patients did not receive antibiotics in the emergency department and ward/intensive care unit within 3 days. There was no statistically significant difference in hospital days (p = 0.239) or mortality (p = 0.345) between those who received and did not receive antibiotics in the emergency department.
Conclusion:
Hospitalized adult patients with leukocytosis did not necessarily require antibiotics in the emergency department except when they had a differential diagnosis that requires antibiotic treatment.
Introduction
Leukocytosis, defined as an increase in white blood cell (WBC) count greater than 11,000 cells per μL, is a common finding with a broad differential diagnosis, encompassing both benign and malignant entities. The normal range for WBC counts changes with age and pregnancy. 1 Healthy newborn infants may have a WBC count ranging from 13,000 to 38,000 cells per μL at 12 h after birth. At 2 weeks of age, this decreases to approximately 5000–20,000 cells per μL, and it gradually declines throughout childhood to reach adult levels of 4500–11,000 cells per μL by approximately 21 years of age. During pregnancy, there is a gradual increase in the normal WBC count (third trimester level of 13,200 cells per μL) and a marginal shift toward an increased neutrophil percentage. 2
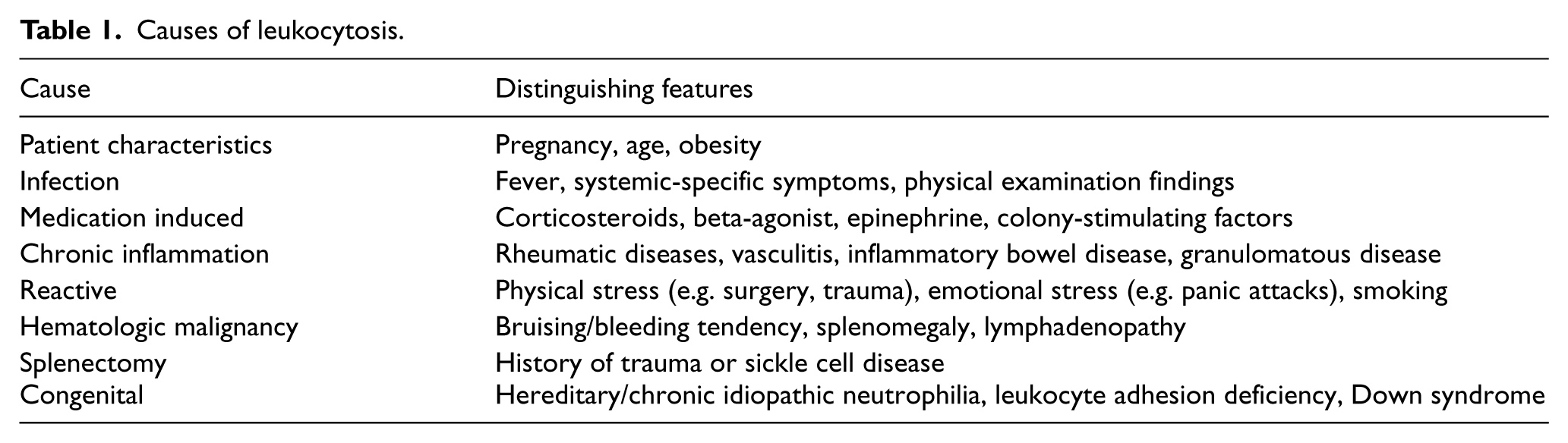
Leukocytosis can arise from infection, medications, stressful conditions, chronic inflammation, hematologic malignancy, and other causes (Table 1).3–7 Leukocytosis provides a diagnostic challenge for emergency physicians. Antibiotics should be considered for patients with infectious diseases, which must be carefully diagnosed according to system-specific symptoms, physical examination findings, and potential biomarkers such as C-reactive protein (CRP) or procalcitonin. 8 To investigate the association between leukocytosis and infectious diseases in the emergency department (ED) and to determine whether there were better outcomes after receiving antibiotics in the ED, we conducted a retrospective study to review the final diagnosis of hospitalized adult patients with leukocytosis and measure outcomes between those who received empirical antibiotics in the ED and those who did not. Based on our findings, when presented with a case of leukocytosis without a definite impression of an infectious disease that requires empirical antibiotic treatment, the emergency physician can decide whether to prescribe an antibiotic.
Causes of leukocytosis.
Materials and methods
The Institutional Review Board of Kaohsiung Veterans General Hospital, Taiwan, approved this retrospective study. Patients with leukocytosis (WBC count >11,000 cells per μL) who were admitted via the ED at the Kaohsiung Veterans General Hospital, from June 2016 to June 2017 were enrolled. Each patient’s medical record was reviewed for documentation of clinical characteristics, final diagnosis, hospitalization duration, comorbidities, mortality, and whether they received antibiotics (both intravenous and oral) in the ED. Patients aged ⩽18 years, pregnant women, those who received prophylactic antibiotics prior to operation, and those with a final diagnosis of hematologic malignancy were excluded from this study.
Receiving antibiotics in the ED was defined as receiving at least one dose of antibiotics in the ED and continuing the treatment in the ward/intensive care unit (ICU) within 3 days after admission. The non-receiving antibiotic group was defined as not receiving antibiotics in the ED and ward/ICU within 3 days after admission. The primary outcome measure was hospital stay, and the secondary outcome measure was mortality. We categorize patients depending on final diagnosis which was made by in charge subspecialist during admission. Two authors must agree with each patient’s categorization based on documented final diagnosis, even chart review, otherwise may categorized to others.
All data were analyzed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). Continuous variables were analyzed using the t test, and categorical variables were analyzed using the chi-square test, except when 20% of the cells had expected counts of <5, in which case Fisher’s exact test was used. The p values less than 0.05 were considered statistically significant.
Results
The characteristics and outcomes of the patients are listed in Table 2. In total, 4486 patients received initial antibiotic treatment in the ED, whereas 3568 patients did not receive antibiotics in the ED and ward/ICU within 3 days. Those who received antibiotics in the ED but discontinued them in the ward/ICU within 3 days and those who did not receive antibiotics in the ED but received them in the ward/ICU within 3 days were excluded. There were no statistically significant differences in age (p = 0.487), sex (p = 0.694), absolute WBC count (p = 0.121), and comorbidities between the groups. Similarly, the outcomes of hospital stay and mortality did not differ significantly.
Clinical characteristics of receiving and non-receiving antibiotic in ED groups.
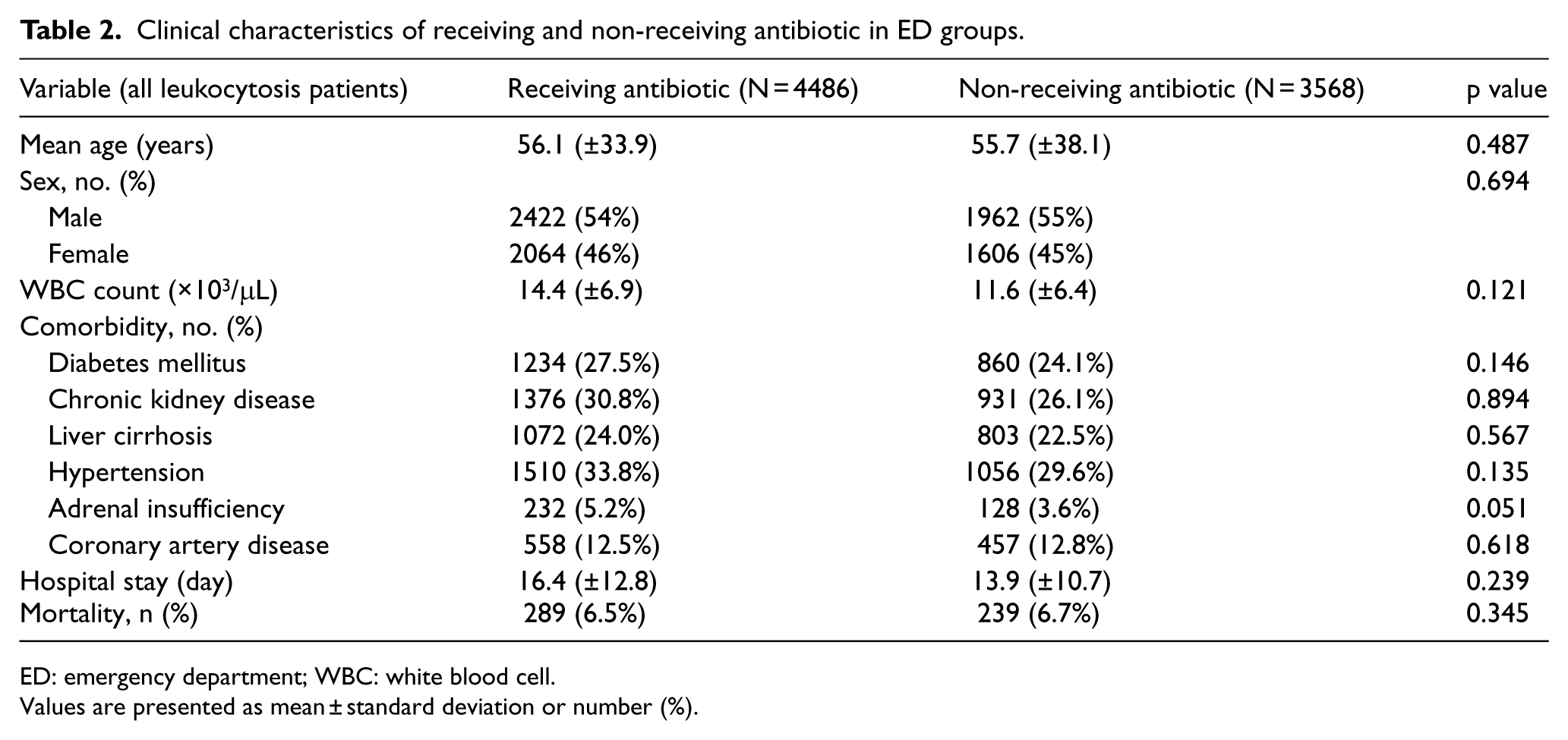
ED: emergency department; WBC: white blood cell.
Values are presented as mean ± standard deviation or number (%).
In the antibiotic-receiving group, 3230 (72%) had a final diagnosis of an infectious disease. In the non-receiving group, 2248 (63%) had a final diagnosis of an infectious disease. In the group of patients confirmed to be non-infectious cause of leukocytosis, we did subgroup analysis based on whether antibiotic was administered only in the ED. This subgroup analysis excluded any patients who might have received antibiotic in ward/ICU to eliminate confounding effect from antibiotic administration at ward/ICU. The outcomes of hospital stay (p = 0.238) and mortality (p = 0.079) did not differ significantly (Table 3). Another subgroup analysis was performed in those confirmed to have an infectious disease based on whether they received antibiotics in the ED. The mean age (64.7 ± 18.7 vs 58.7 ± 15.3 years, p = 0.02) and incidence of diabetes mellitus (41.8% vs 29.8%, p = 0.005) of those who received antibiotics were significantly higher than those who did not receive antibiotics. The outcomes of hospital stay (p = 0.071) and mortality (p = 0.058) also did not differ significantly between the subgroups (Table 4).
Subgroup analysis of patients of leukocytosis without infection in ED (all non-received antibiotic in ward/ICU).
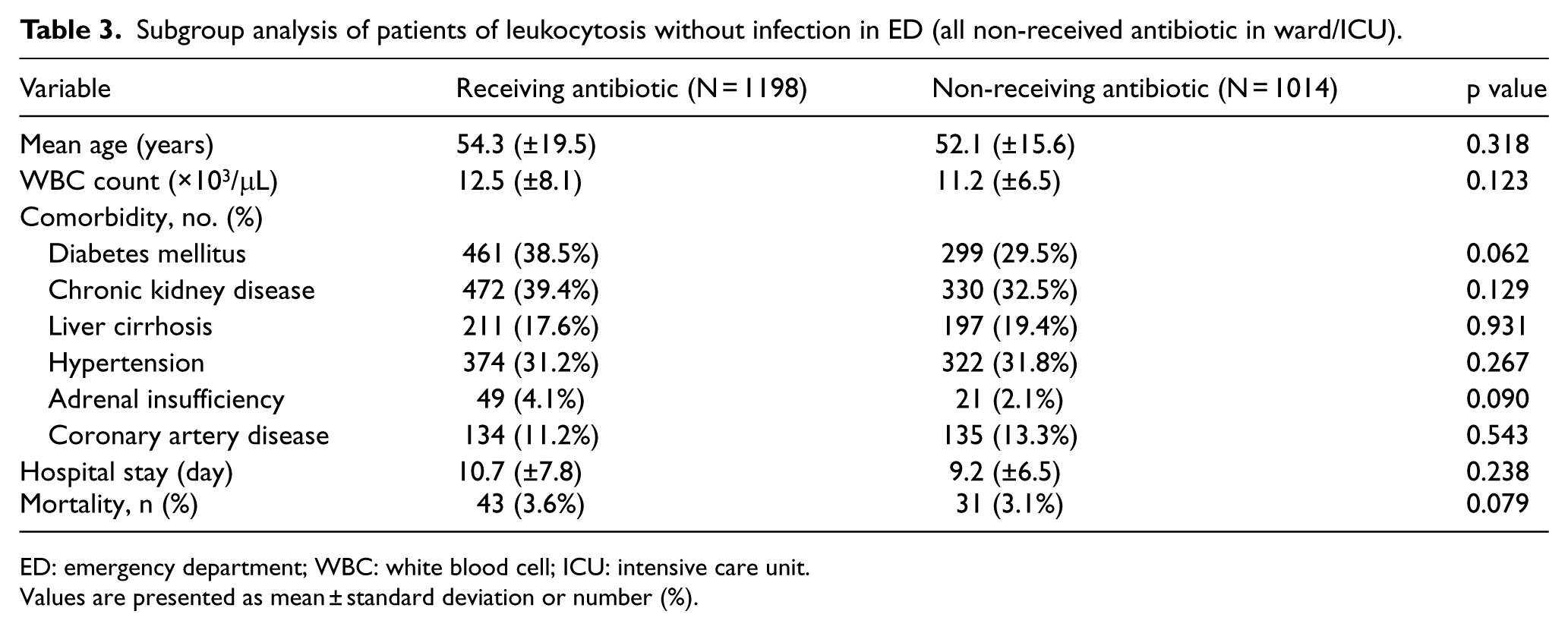
ED: emergency department; WBC: white blood cell; ICU: intensive care unit.
Values are presented as mean ± standard deviation or number (%).
Subgroup analysis of patients of leukocytosis with infection in ED.
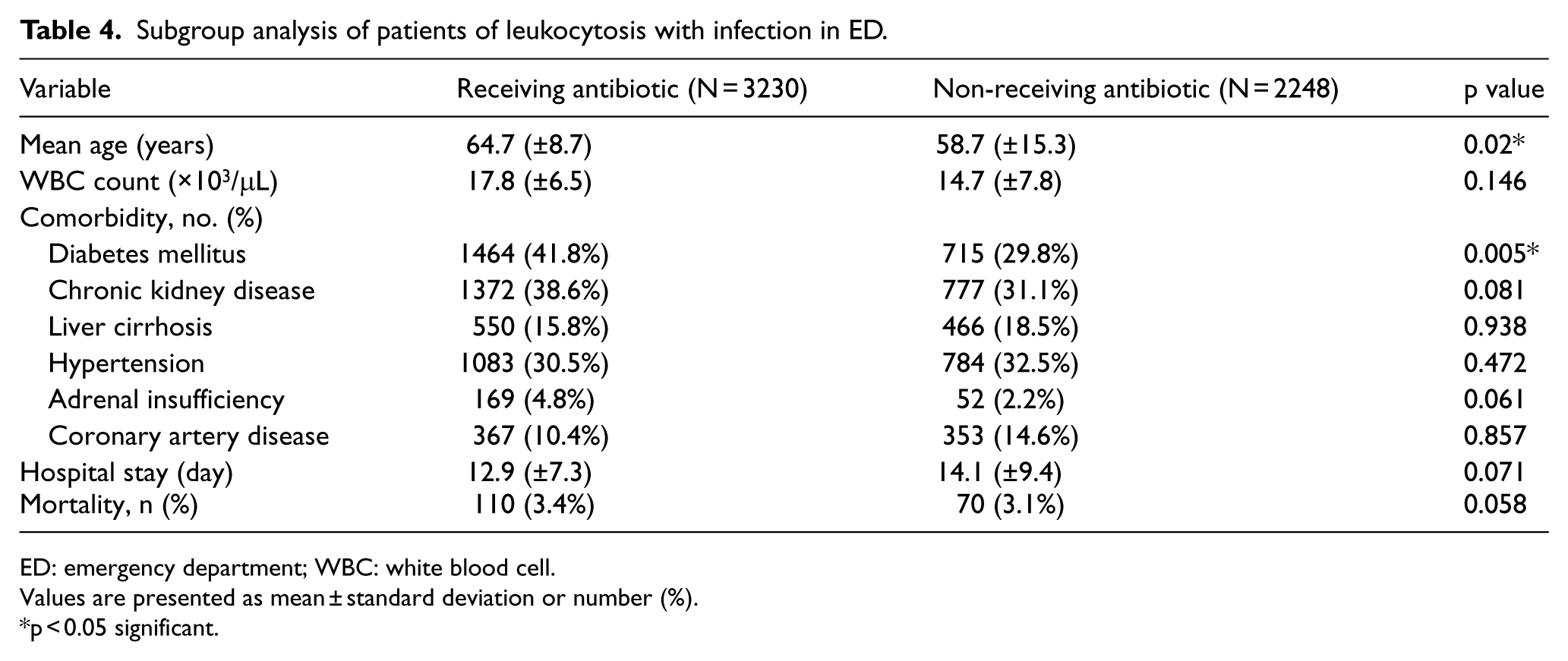
ED: emergency department; WBC: white blood cell.
Values are presented as mean ± standard deviation or number (%).
p < 0.05 significant.
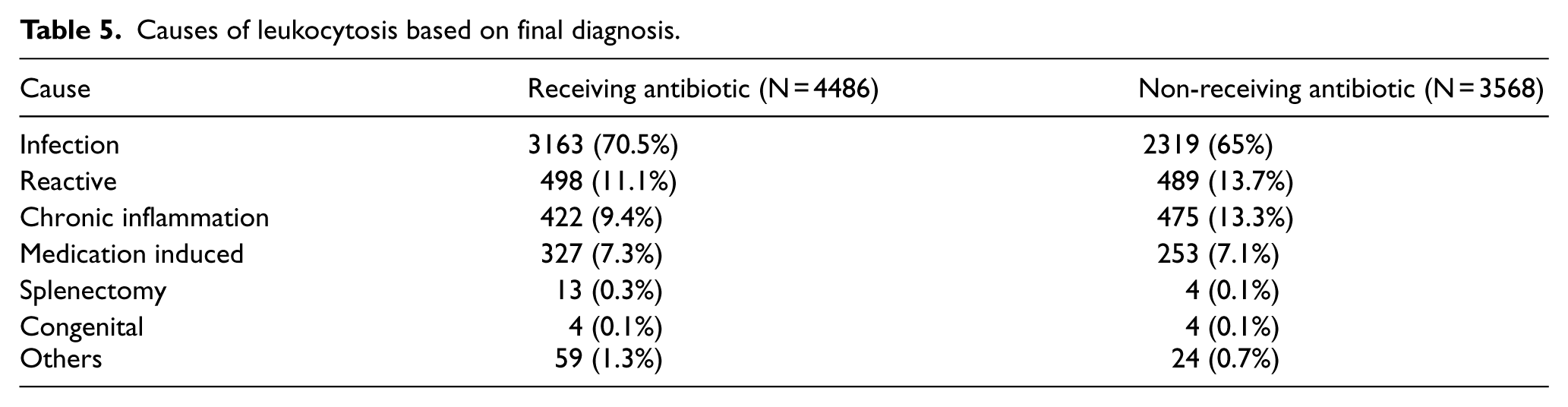
Infectious disease is the most common cause of leukocytosis in the ED, accounting for 68.1% of all causes, followed by reactive inflammation, chronic inflammation, and medication-induced leukocytosis, which account for 12.3%, 11.1%, and 7.2%, respectively (Table 5).
Causes of leukocytosis based on final diagnosis.
Discussion
Leukocytosis is a common laboratory finding among patients in the ED worldwide. Although it is no longer part of the definition of sepsis, 9 it is still highly positively correlated with infectious disease and sepsis. Emergency physicians should prescribe empirical antibiotics in patients with sepsis or severe infection to prevent disease progression. However, in patients with leukocytosis, but without other obvious symptoms/signs of infection, the results vary. Based on our findings, there was no significant difference in absolute WBC count, comorbidities, and outcomes (mortality and hospital stay) between those who received and did not receive antibiotics in the ED groups of all patients with leukocytosis. Furthermore, in the subgroup of patients with leukocytosis without a final diagnosis of an infectious disease who did not receive antibiotics in the ward/ICU, there was no statistically significant difference in hospital days or mortality between those who did and did not receive antibiotics in the ED. In another subgroup analysis, 68.1% of hospitalized adult patients with leukocytosis in the ED had a final diagnosis of an infectious disease. Approximately, 59% of those patients received antibiotics in the ED, whereas 41% did not. Furthermore, there was no significant difference in absolute WBC count, comorbidities, and outcomes between the two groups. However, the mean age and incidence of diabetes mellitus were both significantly higher in those who received antibiotics in the ED, which may have had an impact on emergency physicians’ judgment.
Although infectious disease is the most common cause of leukocytosis in the ED, emergency physicians should be cautious when administering empirical antibiotics with a diagnosis of sepsis or an infection condition that requires antibiotics for hospitalized adult patients with leukocytosis in the ED. Otherwise, there is no better outcome compared to routinely prescribed antibiotics for patients with leukocytosis in the ED. That may have some benefits in reducing medical costs and the incidence of resistant strains of microorganisms in the ED.
Limitations
We recognize some limitations of this study. Not all infectious diseases require antibiotic treatment during hospitalization. The correlation between nosocomial infections and receiving antibiotics in the ED remains unclear. In some patients, the cause of leukocytosis was identified in the ED, which may have biased the results. Further studies are required to determine the significance of these findings.
Conclusion
When encountering patients with leukocytosis in the ED, emergency physicians should prescribe antibiotics under a differential diagnosis of sepsis or an infectious disease that requires antibiotics. Otherwise, prescription antibiotics broadly to patients with leukocytosis do not result in a better outcome.
Footnotes
Acknowledgements
The authors thank all the participants who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data set used and analyzed during this study is available from the corresponding author on reasonable request.