
Abstract
Leukocytoclastic vasculitis (hypersensitivity vasculitis) is defined as small blood vessel inflammation with skin or other systemic manifestations due to infections, drugs, or neoplastic disease. This clinical case report highlights an association between ceftriaxone and leukocytoclastic vasculitis in a 49-year-old female patient with a history of penicillin allergy, on mirtazapine for anxiety disorder. Articles concerning antibiotic-induced leukocytoclastic vasculitis are also reviewed. The patient reported a symptom of upper respiratory tract infection and fever 5 days previously for which she received ceftriaxone for 2 days before presenting to the emergency department with a pruritic skin rash in the upper and lower extremities and swollen lips for 1 day. The rash was erythematous, maculopapular, itchy, and non-tender, with no mucus membrane involvement. Laboratory investigations revealed leukocytosis (white blood cells, 22.3 × 109/L) that was mainly eosinophilic (18.4%). The patient was administered prednisolone and antihistamine after stopping ceftriaxone empirically. A skin biopsy confirmed the diagnosis of leukocytoclastic vasculitis. Significant clinical improvement was observed after treatment initiation. Upon follow-up, the skin rash was resolved entirely with no scars; however, there was skin-peeling over the lower extremities. Recognition of antibiotic-induced leukocytoclastic vasculitis is crucial as many classes of antibiotics can contribute to this condition. Continuation of the offending drug may lead to life-threatening complications.
Keywords
Introduction
Leukocytoclastic vasculitis (also known as hypersensitivity vasculitis) is defined as small blood-vessel inflammation, typically presenting with generalized symptoms, such as fever, arthralgia, myalgia, and skin manifestations described as painful purpuric lesions in the lower and upper extremities. 1, 2 Leukocytoclastic vasculitis is sometimes associated with other systemic manifestations, for example, involving the renal or gastrointestinal systems. 3, 4
Precipitating factors include infections, drugs, chemicals, and systemic and neoplastic disease, 5 with reports of leukocytoclastic vasculitis in patients post coronavirus disease 2019 vaccination, and in those with inflammatory bowel disease. 6, 7 When leukocytoclastic vasculitis is suspected, it may be diagnosed after detailed history, physical examination, and laboratory investigations, and confirmed by punch skin biopsy showing neutrophilic infiltration into small venule walls. 8 –10
Most cases of drug-induced leukocytoclastic vasculitis are treated by discontinuation of the offending agent and application of supportive measures. Severe and chronic cases may require systemic steroids. 5 Here, the case of a 49-year-old female patient who developed leukocytoclastic vasculitis after receiving ceftriaxone for acute pharyngitis is described, and currently available literature regarding leukocytoclastic vasculitis is discussed.
Case report
A 49-year-old female patient with a history of penicillin allergy and Guillain–Barré syndrome secondary to influenza vaccine, presented to the emergency department of King Abdulla Medical City in September 2019, with a pruritic skin rash in the upper and lower extremities and swollen lips for 1 day. Five days prior to hospital presentation, she reported an upper respiratory infection and fever that was treated with ceftriaxone. After taking 1 g intravenous ceftriaxone, daily for 2 days, she developed a skin rash involving the upper and lower extremities, including the palms and soles. The rash was erythematous, maculopapular, and simultaneously pruritic and burning (Figure 1). Swelling was confined to the lower lip, with no facial puffiness, tongue swelling, hoarseness of voice, difficulty breathing, or change in her mental status. Besides the known history of penicillin allergy, the patient reported an allergy to particular foods that suggested an immunoglobulin (Ig)E-mediated process. There was no reported patient or family history of autoimmune diseases. Systemic review was unremarkable, except for generalized arthralgia and myalgia.

Representative image of skin lesions in a 49-year-old patient with leukocytoclastic vasculitis. The lesions covered the anterior and lateral aspect of the lower limbs, and showed asymmetrical violaceous discoloration with sharp borders and different sizes, ranging from 1–6 mm.
On examination, the patient was conscious, oriented and anxious, but not in distress. Vital signs were as follows: blood pressure, 137/84 mmHg; pulse, 127 beats per min; respiratory rate, 18 breaths per min; body temperature, 37.7 °C; and oxygen saturation, 98% room air. The cardiovascular, respiratory, and gastrointestinal examination was unremarkable. The skin exam revealed erythematous, maculopapular, and non-tender rash that spared the mucus membranes and affected the upper and lower extremities, including the palms and soles.
Initial laboratory investigations revealed leucocytosis (white blood cell count, 22.3 × 109/L) with a predominance of eosinophils (18.4%). Results of renal and liver function tests, and urine analysis, were within normal limits. The chest x-ray was unremarkable, but the electrocardiogram showed sinus tachycardia. The patient was started empirically on an anti-inflammatory dose of prednisolone (0.5 mg/kg, oral, daily) and antihistamine (10 mg oral cetirizine, daily). Results of additional blood workup, including tests for antinuclear antibody, rheumatoid factor, herpes simplex virus, complement levels and tryptase level were within normal limits. Skin biopsy revealed perivascular inflammatory infiltrate composed of neutrophils with frequent eosinophils, and prominent vascular damage evidenced by the presence of endothelial injury and extravasated red blood cells (RBCs), suggestive of leukocytoclastic vasculitis (Figure 2). The skin rash progressed after 3 days to involve the trunk in addition to the extremities, with the development of tense bullae and notable development of palpable purpura, mainly on both ankles and heels, which were swollen. Nevertheless, there remained no facial or mucosal involvement. Prednisolone administration was increased to an immunosuppressive dose (1–2 mg/kg, oral, daily) for 5 days with reduction of 5 mg every 3 days, which led to significant clinical improvement and rash resolution.

Representative photomicrographs of haematoxylin and eosin-stained skin pinch biopsy sections, showing mild spongiosis with focal vesicle formation and perivascular inflammatory infiltrate in the dermis, composed of neutrophils and frequent eosinophils. Prominent vascular damage is evidenced by the presence of endothelial injury and extravasated red blood cells.
The patient was discharged, and during an outpatient follow-up visit after 1 month, the skin rash was observed to have resolved entirely with no visible scars. However, skin-peeling was observed over the lower extremities.
Ethics approval was not deemed necessary for this case report. Patient data were deidentified and verbal informed consent to publish the case was obtained from the patient. The reporting of this study conforms to CARE guidelines. 11
Discussion
Leukocytoclastic vasculitis is a histopathologic term commonly used for small-vessel vasculitis, also known as hypersensitivity vasculitis. The incidence rate is around 30 cases per million people per year, and it affects both sexes equally. 12, 13 Leukocytoclastic vasculitis may occur as a primary disorder or as a secondary condition in association with drugs, infections (particularly upper respiratory tract infections), collagen-vascular diseases, hematologic disorders, or malignancy. 14 However, in around one-third of patients, the precipitating factors are impossible to ascertain. 15
Drug-induced leukocytoclastic vasculitis accounts for about 10% of all vasculitis cases. Antibiotics, particularly beta-lactam groups, sulfonamides, and quinolones; cyclosporine; azathioprine; methotrexate; and allopurinol; antithyroid drugs, particularly propylthiouracil; valproic acid; phenytoin; anti-tumour necrosis factor-α agents; and hydralazine are well-known causes of leukocytoclastic vasculitis. 15 –19
Leukocytoclastic vasculitis usually presents as skin lesions in a palpable purpuric form that likely begins 7–21 days after exposure to a particular agent. It mostly involves the lower extremities and less frequently affects the forearm, hand, back, sacral, and gluteal regions. Other less common skin manifestations include vesicles, bullae, nodules, or ulcers. In addition to skin lesions, leukocytoclastic vasculitis may be associated with systemic manifestations, such as abdominal and joint pains, and renal involvement. 20
Detailed history, physical examination and laboratory workup are essential steps in evaluating leukocytoclastic vasculitis, focusing on the presence of underlying cause and systemic involvement. 21 The American College of Rheumatology proposed criteria to define leukocytoclastic vasculitis including patient age >16 years; use of a possible drug in temporal relation to symptoms; palpable purpura; maculopapular skin lesions; and biopsy of a skin lesion showing neutrophils around arterioles or venules. At least three of five criteria must be present to diagnose leukocytoclastic vasculitis with a sensitivity of 71% and specificity of 83.9%. 22 The present case scored 5 out of 5, which favours the diagnosis of leukocytoclastic vasculitis.
Biopsy of skin lesions for histopathology and examination under immunofluorescence is the gold standard for confirming a diagnosis. The presence of perivascular inflammatory cell invasion with necrosis of the vessel wall and fibrinoid material deposition is pathognomonic for leukocytoclastic vasculitis. 17 These findings may change after approximately 2 days, so it is necessary to take a biopsy within 24–48 h from the onset of skin lesions. 10, 21
The precise mechanism of pathogenicity of leukocytoclastic vasculitis is unknown. However, circulating immune complex deposition in the walls of arterioles, capillaries and postcapillary venules is proposed to play a role. 23 –25 Immune complex deposition (IgG and IgM) leads to activation of the complement cascade (C3a and C5a), which produces chemotactic factors and vasoactive cytokines. Consequently, neutrophils become activated and migrate to the affected tissue injuring the vessel wall by releasing lysosomal enzymes such as collagenases, elastase and free oxygen radicals. Thus, permeability of the damaged vessel wall increases, causing leakage of RBCs and fluid that generates purpura. 3, 4, 10, 25
The management of cutaneous leukocytoclastic vasculitis depends on the aetiology and severity of disease. Mild cutaneous manifestations are self-limited and may need symptomatic relief with antihistamine and nonsteroidal anti-inflammatory drugs with discontinuation of the offending agent. However, systemic involvement needs steroids alone or in combination with immunosuppressive drugs. 10, 20, 26 In general, skin-limited disease has a good prognosis, and the time to recovery is variable, ranging from days to weeks. 27, 28 Nonetheless, around 10% of reported cases develop recurrent or chronic involvement. 29
An extensive review of the published literature was performed by searching three databases (PubMed, Scopus, and Google Scholar) for articles published between January 1955 and October 2021. Keywords used in the search were: antibiotic-induced leukocytoclastic vasculitis, antibiotic and leukocytoclastic vasculitis. Case reports and case series with study samples aged >16 years, involving antibacterial drug, that were published in English were included. After removal of duplicates, all articles were fully reviewed by two researchers (AAA and ESB).
A total of 60 published articles were included, comprising a total of 74 cases published between 1955 and 2021 (Table 1). 20,26,27,30 –86 Analyses of the reported cases of antibiotic-induced leukocytoclastic vasculitis revealed that it is associated with numerous classes of antibiotic, including penicillin (amoxicillin, amoxicillin-clavulanic acid, oxacillin), cephalosporins (cefazolin, cephalexin, cefuroxime, ceftriaxone, cefotaxime), fluoroquinolone (ciprofloxacin, levofloxacin, ofloxacin), macrolides (azithromycin, clarithromycin), vancomycin, teicoplanin, trimethoprim-sulfamethoxazole, dapsone, linezolid, pristinamycin, tigecycline, isoniazid, streptomycin, rifampin, ethambutol, and pyrazinamide.
Review of published cases reporting antibiotic-induced leukocytoclastic vasculitis.
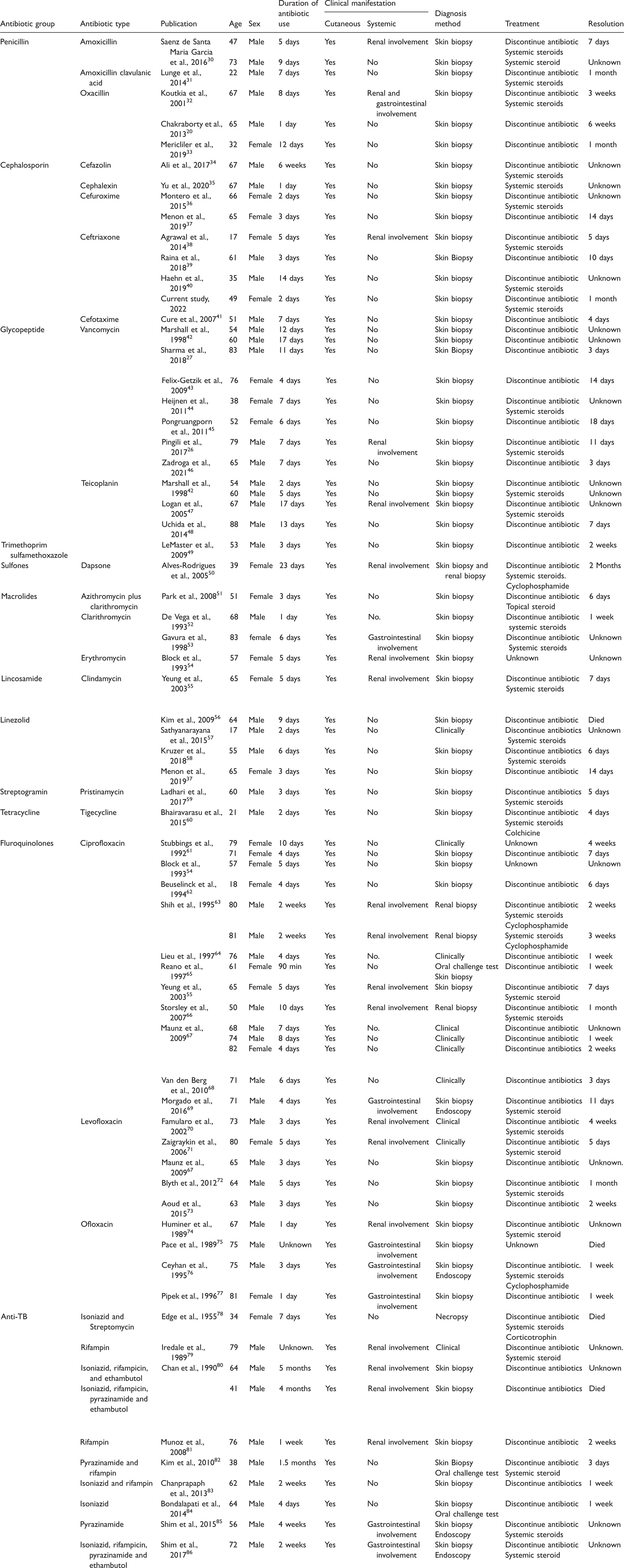
Based on the present review, the most common antibacterial drug-type to cause leukocytoclastic vasculitis was the fluoroquinolone group, particularly ciprofloxacin. The minimum duration for developing symptoms was 1 day and the maximum duration was 5 months. Patient age ranged between 17 and 88 years and twice as many male than female patients were affected, which contradicts a previous study suggesting no predominance between the sexes. 26
All cases presented with non-blanching purpuric rash in all extremities, and the trunk and face without affecting the mucous membrane. However, 26 cases showed systemic manifestations along with skin lesions; 18 of which involved the kidney in the form of acute kidney injury, seven involved gastrointestinal systems and presented with diarrhoea and hematemesis, and one case had both gastrointestinal and renal involvement.
The patient in the present case was a 49-year-old female who presented with localized symptoms in the form of a non-blanching purpuric rash that started in both extremities and progressed to involve the trunk. There was no systemic involvement, and the rash was preceded by ceftriaxone intravenous injection that was administered for upper respiratory tract infection 2 days prior to presentation for rash. The majority of cases included in the review (64 out of 74 cases) were diagnosed by skin biopsy and a few were diagnosed by clinical examination, kidney biopsy, endoscopy, or oral challenge test. The present case was diagnosed by skin biopsy that showed a typical finding for cutaneous vasculitis.
The reviewed cases were treated either by discontinuation of the offending antibiotic alone or with the addition of systemic steroids. Cyclophosphamide was administered in four cases, all of which had systemic involvement (renal and gastrointestinal). Most of the cases were observed to have complete skin manifestation resolution and normalized kidney function, except four deceased cases. The duration of resolution varied from 3 days to 2 months. In the present case, ceftriaxone discontinuation and systemic steroid administration resulted in complete recovery in 1 month.
In conclusion, medications are one of the important precipitating factors of leukocytoclastic vasculitis and some, such as antibiotics, are used in daily practice. Thus, recognition of this reaction is important as it may lead to fatal consequences, and discontinuation of the offending drug is a major part of the management.
To the best of our knowledge, this is the first reported case of ceftriaxone-induced leukocytoclastic vasculitis in the Middle East, and the first published review of articles concerning antibiotic-induced leukocytoclastic vasculitis.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221097768 - Supplemental material for Ceftriaxone-induced leukocytoclastic vasculitis: a case report and literature review of antibiotic-induced leukocytoclastic vasculitis
Supplemental material, sj-pdf-1-imr-10.1177_03000605221097768 for Ceftriaxone-induced leukocytoclastic vasculitis: a case report and literature review of antibiotic-induced leukocytoclastic vasculitis by Aseel A Almasoudi, Eman S Bablghaith, Samaher I Alaauldeen, Ayman M Falemban, Ahlam A Sherbeeni and Adeeb A Bulkhi in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.