
Abstract
Background:
The Radboud university medical center designed an obligatory basic life support and first-aid course for first-year medical students.
Objectives:
We evaluated the value of an additional train-the-trainer course following European Resuscitation Council guidelines, which focuses on practical basic life support training and providing feedback, in comparison with standard in-service instructor training.
Methods:
This study was a prospective randomized controlled trial. A total of 10 intervention instructors, 14 control instructors, and 337 first-year medical students participated in the study. Students, blinded for the type of instructor, completed questionnaires evaluating the quality of the basic life support training (theoretical and practical) and provided feedback. The secondary endpoint was the basic life support examination to assess whether the instructors’ training influenced the quality of the participants’ basic life support.
Results:
The response rate of the questionnaire was 82% on average. No differences were found between intervention and control group concerning theoretical basic life support training. The intervention instructors scored significantly higher on practical basic life support training according to student evaluations (p < 0.001). The pass rate on basic life support examinations did not differ significantly (p = 0.669). Appreciation of given feedback was independent of instructors’ educational training.
Conclusion:
This study is the first to establish that the 12-h train-the-trainer course following European Resuscitation Council guidelines improves students’ appreciation of practical basic life support training. The additional course did not influence appreciation of theoretical basic life support training or perceived feedback.
Introduction
Immediate initiation of basic life support (BLS) is crucial for survival in cases of sudden cardiac arrest. 1 Successful management of sudden cardiac arrest is based on the concept of the chain of survival;2,3 correct performance of BLS is a pivotal step in this chain. 4 The term BLS refers to maintaining airway patency and supporting breathing and circulation with chest compressions and mouth-to-mouth ventilation. 5 Correct performance of BLS is an important determinant of survival in case of sudden cardiac arrest6–8 and a core skill required of all (undergraduate) healthcare professionals. However, it has been widely documented that most healthcare professionals9,10 and medical students11–13 fail to demonstrate adequate resuscitation skills. Tan et al. 14 reported that only one-third of medical students felt competent providing BLS, and once taught, long-term retention is poor. 15
Every medical school in the Netherlands teaches BLS according to European Resuscitation Council (ERC) guidelines. An obligatory BLS and first-aid course has been designed for first-year medical students at Radboud university medical center (Radboudumc). Instructors of this course are senior medical students who have received an in-service training. According to a systematic review by Harvey et al., 16 medical students are as effective as medical doctors as first-aid instructors and accepted by their students. At Radboudumc, it was decided to gradually professionalize part of the staff of instructors through an officially accredited train-the-trainer course following the 2005 ERC guidelines that were current at the time of the study. 17 The Dutch Resuscitation Council (DRC) provided this train-the-trainer course.
The goal of this study was to assess the effect of this course on students’ perceptions of instructors’ theoretical and practical BLS teaching skills. The BLS examination scores of both instructor groups were compared. This study was conducted to examine whether accredited train-the-trainer courses improve the quality of BLS training.
Methods
Subjects and setting
This prospective randomized controlled trial was conducted between October 2010 and May 2011 at the scientific educational institute of Radboudumc in the Netherlands. First-year medical students participating in the BLS and first-aid course were eligible for the study.
The BLS and first-aid course consisted of eight training sessions that took place for 2 h a week in groups of 15 students. Theoretical and practical BLS training began in the first lesson and continued during the course following deliberate practice as learning strategy. 18
Each student should have passed a theoretical and practical examination a week after the last class in order to successfully complete the course.
The 24 participating instructors were randomized in two groups by an independent third party. The instructors were second- to sixth-year medical student instructors, all of whom had attended an in-service instructor training. This in-service training consisted of three 3-h instructional evenings delivered by certified first-aid instructors from the Orange Cross. The Orange Cross is a first-aid and BLS provider for lay people in the Netherlands. The training focused on BLS instruction and providing feedback for course participants. The control group of instructors received the in-service instructor training only.
The intervention group of instructors received the same in-service instructor training and an additional train-the-trainer course. This 12-h train-the-trainer course provided by the DRC involved 2 days in which professional instructors trained the peer instructors. The focus of the first day involved practical teaching of BLS, including the four-step Peyton approach. The focus on the second day was aimed at providing immediate and post-event feedback. Written consent was obtained from all participating students and instructors. The institutional review board concluded that study approval was not necessary.
Study design
Age, sex, nationality, and first-aid experience of the students were recorded during the first lesson. Students were randomized to receive training from an instructor from the intervention group (n = 144) or an instructor from the control group (n = 193). All groups were taught in accordance with ERC guidelines 2005, 17 since the 2010 guidelines were released during the course of the study. Students were blinded for the previous educational course(s) of their instructor. Instructors were asked not to communicate about having attended the additional train-the-trainer course.
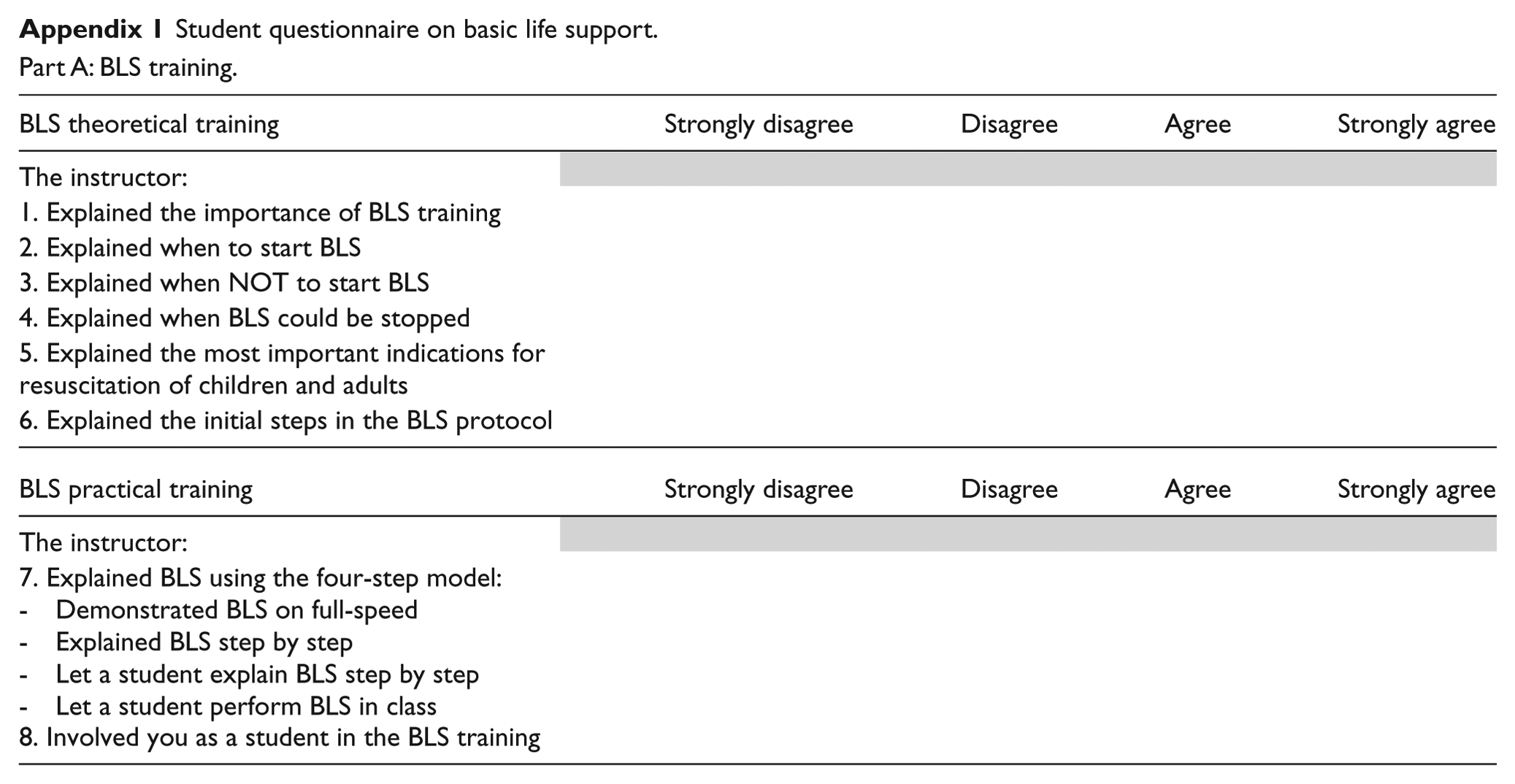
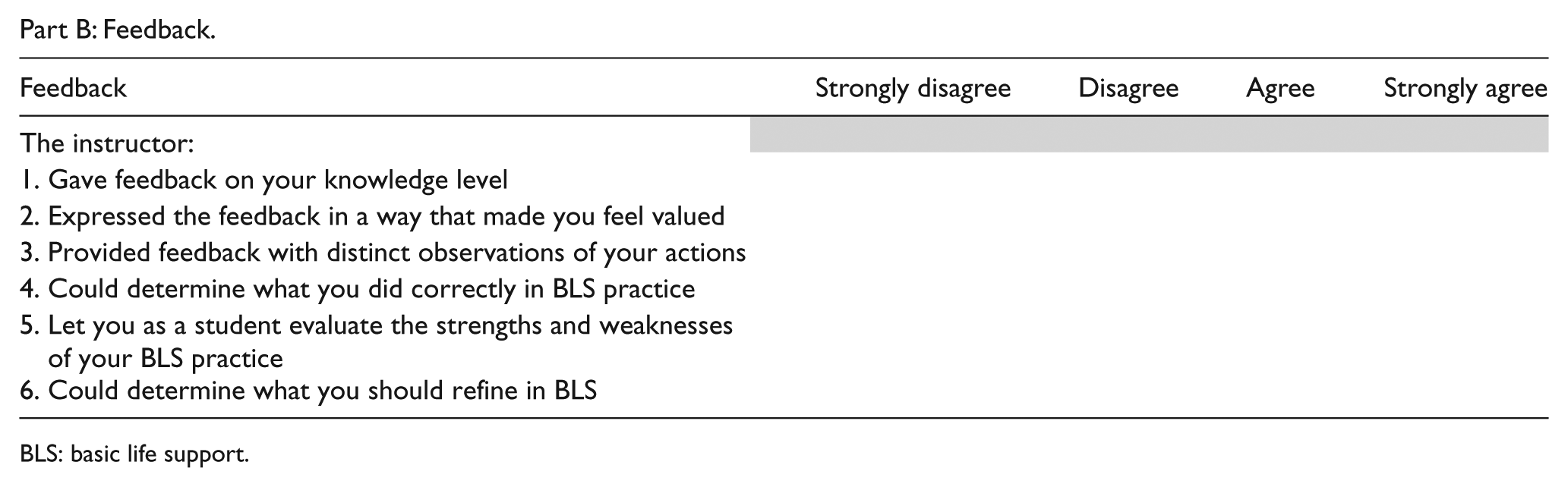
Every student completed a questionnaire (Appendix 1) after the first, fourth, and eighth lessons. This newly designed questionnaire was based on Turner et al.’s 19 study and expert opinions on assessment of feedback. 20 The questionnaire explored students’ opinions on instructors’ skills regarding theoretical and practical BLS training and on provided feedback. The questionnaire consisted of 15 items in two domains of BLS training (6 theoretical and 2 practical items) and feedback (7–8 items). Answers were indicated on a 4-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree). Also, all instructors filled in a questionnaire concerning self-assessment on didactical and practical resuscitation skills, derived from a didactical assessment used by the DRC to examine BLS instructors (Appendix 2).
Examinations of practical BLS consisted of six cycles of compressions and ventilations on an Ambuman C (Ambu, Ballerup, Denmark) with an Ambu CPR Controller printer that allowed variable data to be collected on a printout of the performed examination. BLS skills were assessed using modified Berden criteria 21 because these criteria were the last validated tool for assessing BLS in the algorithm in which the students were trained (without automatic external defibrillation). The study design is displayed in Figure 1.
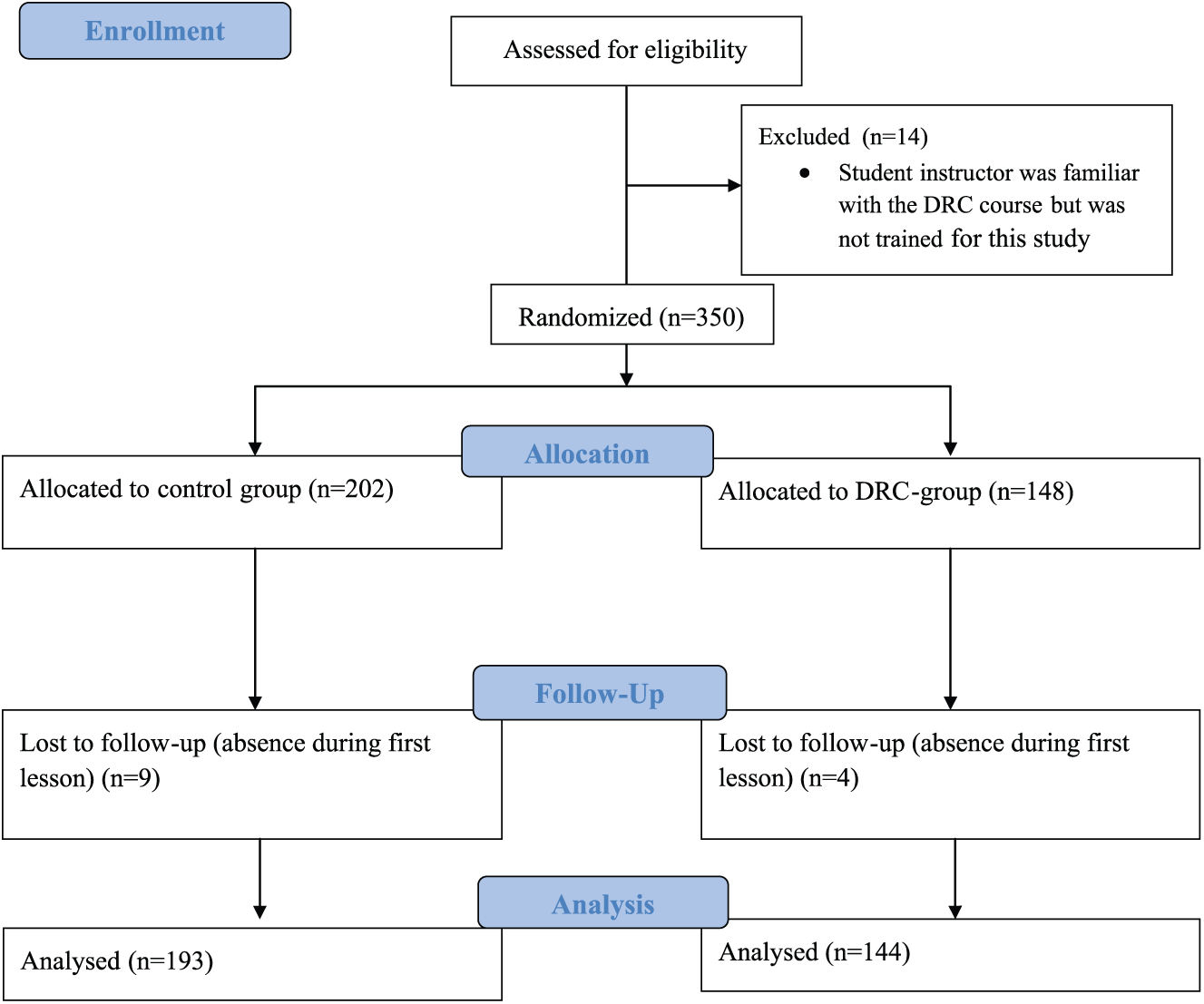
Flowchart of study subjects. The flow of students through the study is shown. Fourteen students, who were initially assessed for eligibility, were excluded before initial testing because the instructor was not randomized to receive the train-the-trainer course of the DRC, but did attend to it. During the course, 13 students were lost during follow-up because of their absence in the first lesson.
An expert panel consisting of one trauma surgeon, one emergency medical physician, one nurse anesthetist, and one educational specialist viewed training videos of all instructors in initial BLS training (the first lesson in BLS). The expert panel completed the didactical assessment used by the DRC to examine BLS instructors (Appendix 2).
Outcomes
The primary outcomes were the results of the “Student’s Questionnaire on Basic Life Support” on theoretical and practical BLS training and the results of the expert panel. The secondary endpoint was the results of the BLS examination performed by the students scored using the modified Berden criteria.
Statistical analysis
Statistical procedures were conducted using the Statistical Package for the Social Sciences (SPSS, version 18.0.01, SPSS Inc., Chicago, IL, USA). Data verification was performed by checking 10% of the data for accuracy and inconsistencies; no inconsistencies were found. Cronbach’s alpha was calculated for the total questionnaire and valued at 0.850. For analysis, the 16 items on the questionnaire were divided into three subcategories: theoretical and practical BLS training and feedback. In addition, repeated measurement analysis (generalized least squares) was conducted to assess students’ scores concerning perceived feedback across three time periods (after lessons one, four, and eight) between the control and intervention groups. Comparisons were made between group scores on the BLS examination using Fisher’s exact test. Bland–Altman plots were constructed to graphically overview differences in scores of self-assessments by the BLS instructors and the expert assessment. Mann–Whitney U test was performed to assess mean rank scores between DRC and control instructors. For all statistical testing, p < 0.05 was considered statistically significant.
Results
Characteristics of study groups
In total, 10 instructors in the intervention group and 14 instructors in the control group participated in this study. Both groups of instructors were comparable in sex, age, and prior BLS teaching experience (Table 1). In total, 337 medical students, 108 male (32%) and 229 (68%) female, participated in this study (Table 2). The intervention group consisted of 144 people (43%), and the control group (57%) consisted of 193. Sex, age, physical health status, and prior first-aid experience were comparable in both groups.
Characteristics of instructors.
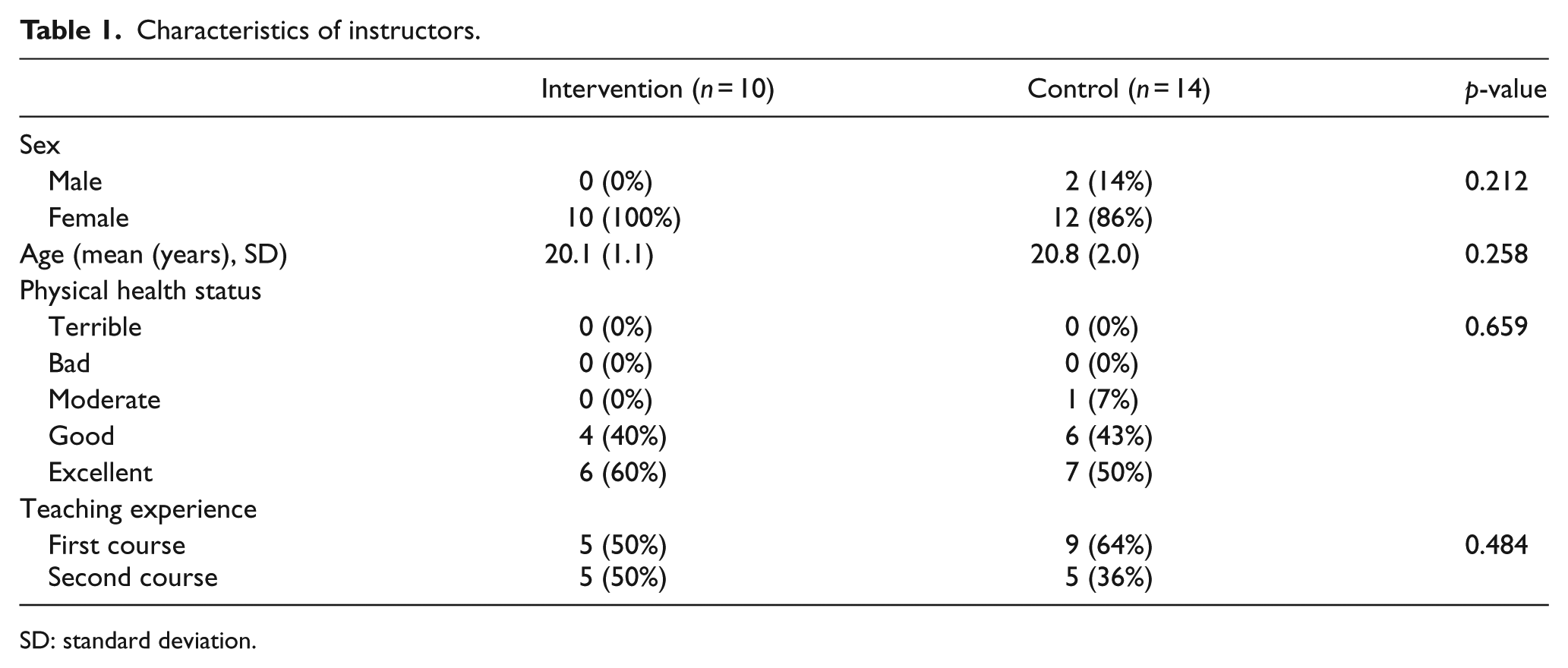
SD: standard deviation.
Characteristics of included students.
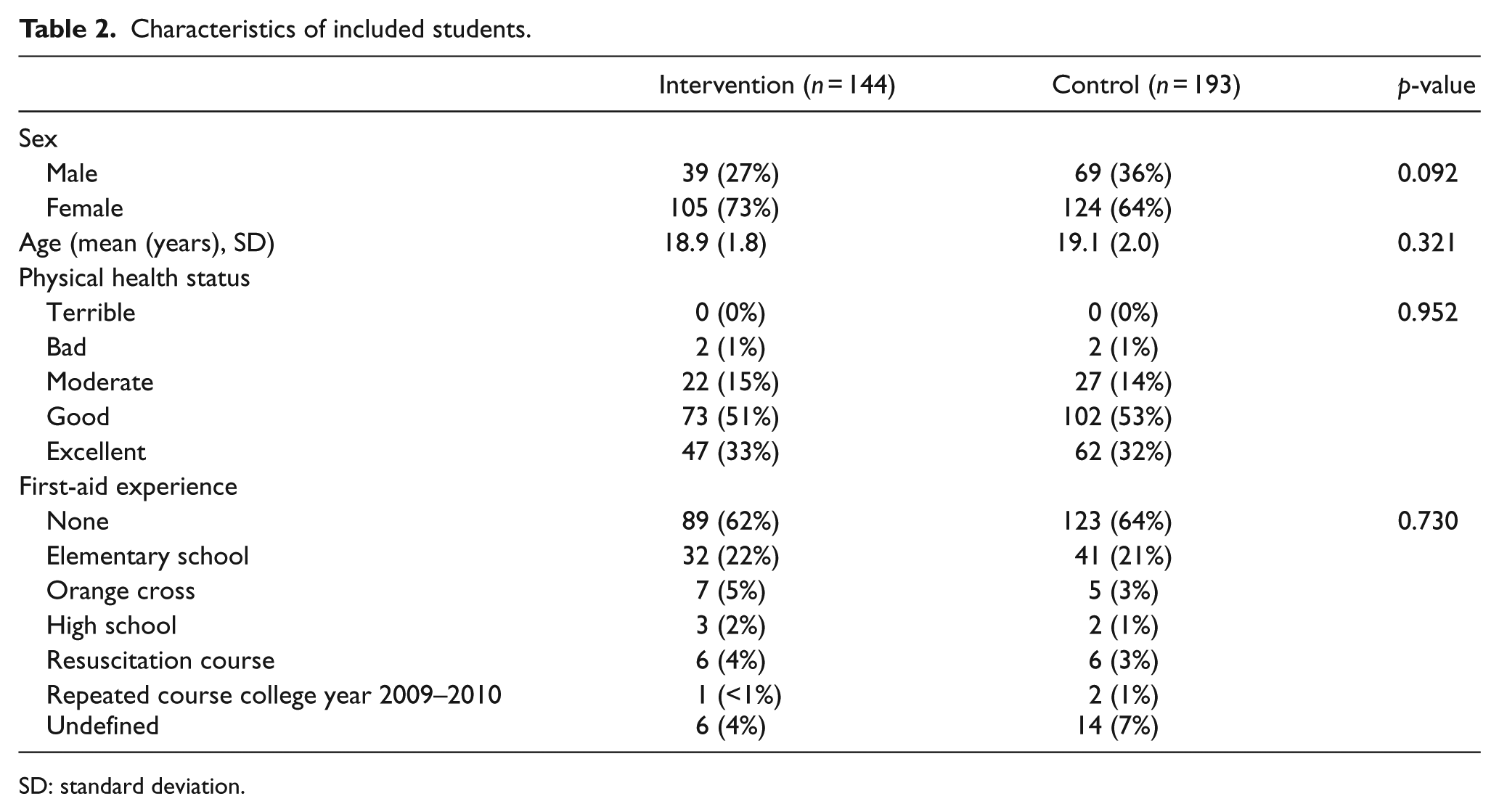
SD: standard deviation.
Theoretical and practical BLS training
The number of students who returned the first, second, and third questionnaires was 337 (100%), 276 (82%), and 281 (83%), respectively. Six items explored theoretical BLS training, and no significant difference was found between the intervention and control groups (p = 0.142, 95% confidence interval (CI): –0.047 to 0.305). Two items addressed appreciation of practical BLS training, and the intervention group scored significantly higher on these items (p < 0.001, 95% CI: −0.531 to −0.192; Table 3).
Results of the students’ questionnaire on BLS.
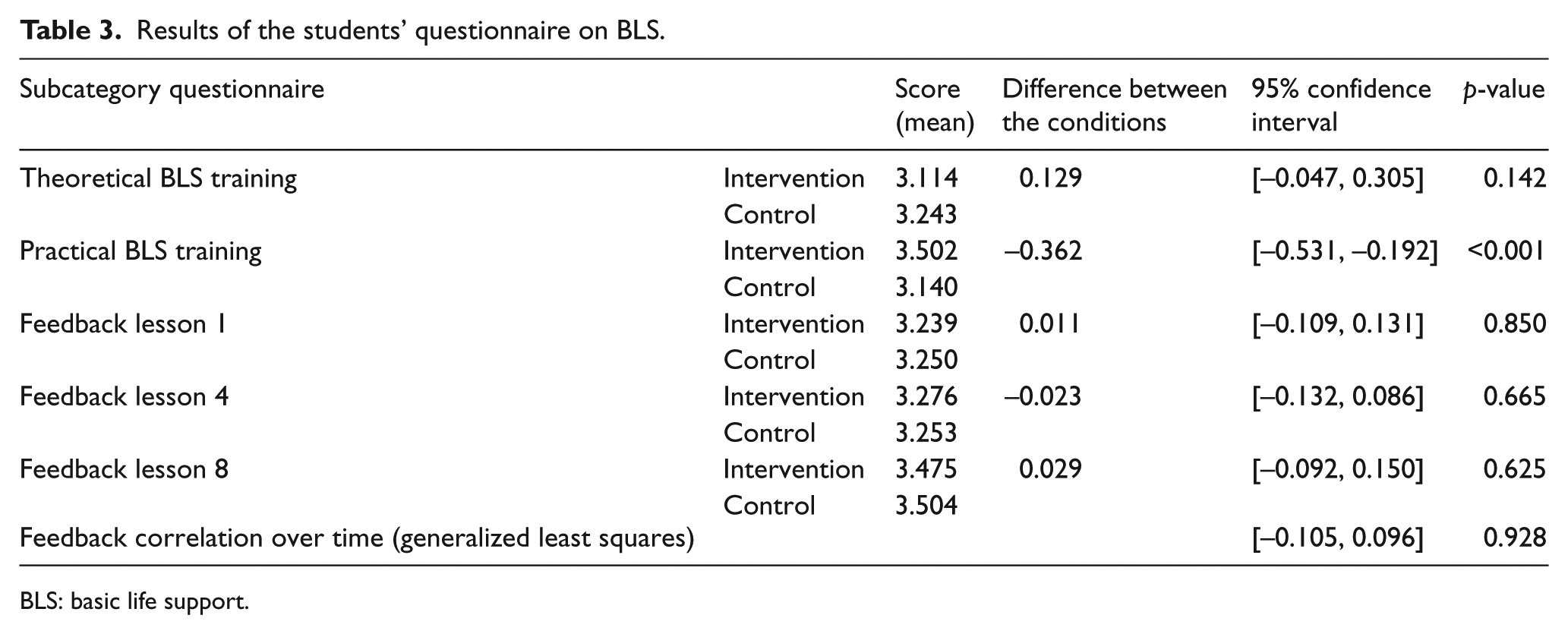
BLS: basic life support.
Eight items explored the quality of perceived feedback after BLS training. Appreciation of given feedback improved during the course in both groups and was independent of instructors’ educational training (p = 0.928, 95% CI: –0.105 to 0.096; Table 3).
Instructor self-assessment and expert observation
No differences were found between instructor self-assessment on resuscitation skills in general and on practical BLS skills between both groups. Expert panel observational assessment of the instructors revealed no differences between the intervention and control groups (data not shown).
BLS examination
In total, 321 students (95%) attended the BLS examination: 138 (96%) students in the intervention group and 183 (95%) in the control group. No differences were found between the groups trained by either the intervention group or control group. Most errors were observed in breathing volume, which was often insufficient. According to the modified Berden criteria, only 14 (10%) intervention group students and 16 (9%) control group students passed the BLS examination (p = 0.669).
Discussion
The additional train-the-trainer course had no positive impact on outcome in terms of quality of BLS scored by an expert panel and examination rates. However, practical BLS training had a perceived beneficial effect in the intervention group. In theoretical BLS training, no differences were found. Theoretical BLS training was provided during the first lesson. Hence, the equality in the results for the appreciation of theoretical BLS training might be explained by the possibility that the instructor had yet to evolve in his or her role as a teacher. This possibility is supported by the tendency of a greater appreciation of feedback in lesson eight compared to lesson one.
In general, it has long been known that deliberate practice is an evidence-based strategy for gaining new skills.18,22 Deliberate practice involves repetitive performance of intended cognitive of psychomotor skills in a focused domain coupled with rigorous skills assessment that provides learners with specific informative feedback that results in increasingly better skills performance in a controlled setting.22,23 Both groups were trained through deliberate practice. The instructors in the intervention group gave greater focus to this strategy because skill assessment and feedback, key elements of deliberate practice, were part of the train-the-trainer course. The additional train-the-trainer course may not have had the expected effects because all students were trained with this strong learning strategy, and the in-service instructor training was sufficient for the intended effect.
Considering that psychological factors play a crucial role in BLS training, readiness, participation, relevance, and reinforcement are important predictors of students’ motivation in BLS training.24,25 The instructor’s role to motivate and provide feedback in BLS training is also critical. 26 It is suggested that the characteristics of instructors and students are essential to efficient and appreciated BLS training. Unfortunately, these characteristics were not tested or scored in the study.
The focus alternated between giving feedback in action as well as on action. Although it was expected beforehand, the train-the-trainer course did not result in greater appreciation of the feedback compared to the control group. In addition, observation by the expert team of videos of both instructor groups did not reveal any differences. Perhaps the duration of the train-the-trainer course was too short to improve instructors’ skills in providing feedback. Regarding previous studies, the form of feedback influences results and may have contributed to the lack of difference between the two instructor groups. 4 Wulf and Shea 27 illustrated that complex motor skills such as cardiopulmonary resuscitation are better acquired through continuous objective feedback rather than subjective concurrent or terminal feedback. However, in this study only subjective concurrent and terminal feedback was applied. The possibility that the form of the feedback is more essential than the training of the instructor should be considered.
It was anticipated that the additional train-the-trainer course would result in higher exam pass rates among students. Nevertheless, the intervention and control groups achieved equally low pass rates. It is possible that many other factors interfere with a student’s performance on an examination, like stress or effort in training. Using the modified Berden criteria, passing percentages in the BLS examination were disappointing (intervention 10%, control 9%). Compared to Perkins et al. 28 and Harvey et al.’s 16 studies, the percentage of students who passed their first exam was low. The modified Berden criteria, developed in 1992, are inconsistent with current ERC guidelines and, for this reason, not taught to the students. Notably, insufficient ventilation was the main cause for failing the examination. This finding is consistent with Spooner et al. 4 and Wenzel et al., 29 who stated that ventilation technique is difficult to acquire. It is important to notice that the modified Berden criteria was not the scoring tool used at Radboudumc during the examination. Radboudumc developed a tool following current ERC guidelines that resulted in a pass rate of 63% in both groups. Because our Radboudumc tool is not validated, it was excluded from this study.
This study has certain limitations. Prior to the start of the first-aid course, the students’ baseline levels of performing BLS were not determined. Although unexpected because of randomization and similar first-aid experience of students in both groups (Table 2), it cannot be ruled out that baseline BLS performance level differed between the two groups. In addition, feedback was only measured subjectively in this study. Continuous objective measurements of feedback with video analysis by a panel of clinical experts could have provided more details about the actual feedback quality of the instructors. Furthermore, intervention instructors received more training hours in total compared to control instructors. Perhaps the significant improvement in appreciation of practical BLS training can be attributed to the number of training hours rather than the quality of the hours. At last, there are no validated examination guidelines following ERC 2005 criteria without automatic external defibrillation. With no other alternatives available, the modified Berden criteria were used during the BLS examination, resulting in very low pass rates.
It is questionable whether the improvements made by the accredited train-the-trainer courses on the BLS training were cost-effective when only a small part of the course was significantly enhanced.
Conclusion
This study is the first to establish that a 12-h train-the-trainer course following ERC guidelines improves the appreciation of practical BLS training. The additional course did not influence appreciation of theoretical BLS training, perceived feedback, or scores on the BLS exam.
Footnotes
Appendix 2
Appendix 1
Student questionnaire on basic life support.
Part A: BLS training.
| BLS theoretical training | Strongly disagree | Disagree | Agree | Strongly agree |
|---|---|---|---|---|
| The instructor: | ||||
| 1. Explained the importance of BLS training | ||||
| 2. Explained when to start BLS | ||||
| 3. Explained when NOT to start BLS | ||||
| 4. Explained when BLS could be stopped | ||||
| 5. Explained the most important indications for resuscitation of children and adults | ||||
| 6. Explained the initial steps in the BLS protocol | ||||
| BLS practical training | Strongly disagree | Disagree | Agree | Strongly agree |
| The instructor: | ||||
| 7. Explained BLS using the four-step model: |
||||
| 8. Involved you as a student in the BLS training |
Part B: Feedback.
| Feedback | Strongly disagree | Disagree | Agree | Strongly agree |
|---|---|---|---|---|
| The instructor: | ||||
| 1. Gave feedback on your knowledge level | ||||
| 2. Expressed the feedback in a way that made you feel valued | ||||
| 3. Provided feedback with distinct observations of your actions | ||||
| 4. Could determine what you did correctly in BLS practice | ||||
| 5. Let you as a student evaluate the strengths and weaknesses of your BLS practice | ||||
| 6. Could determine what you should refine in BLS |
BLS: basic life support.
Acknowledgements
The authors would like to thank P. de Ruijter, C. Fluit, E. van Weel-Baumgarten, T. Klaassen, and all first aid instructors within the Radboudumc first aid and BLS course. Y.B., E.M.R.v.d.P., H.v.G., and E.C.T.H.T. developed the study design. Y.B. and E.M.R.v.d.P. collected and analyzed the data and wrote the article. J.M.Th.D., H.v.G., and E.C.T.H.T. read the article several times and provided feedback on the article. R.D. gave us statistical advice.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets and analysis during the current study are available from the corresponding author on reasonable request.
Ethical approval and consent to participate
The authors contacted the CMO Arnhem-Nijmegen, which is an acknowledged Medical Ethical review commission. After careful examination of the research proposal, the institutional review board concluded that study approval was not necessary, since this research only used questionnaires and so there would be no potential harm to the participants. Furthermore, the anonymity of participants was guaranteed, and informed consent of participants had been obtained prior to the research.