
Abstract
Introduction:
No definitive answer has been given to the question ‘who should teach cardiopulmonary resuscitation?’ Healthcare professionals and high school teachers are mostly the trainers, but medical students are increasingly being used for this purpose.
Methods:
We divided 296 high school students in three groups based on trainer professional level. Medical students, anaesthesia and intensive care residents, and anaesthesia and intensive care specialists provided basic life support training. We tested their theoretical knowledge with the help of a multiple-choice question questionnaire and practical abilities with the help of a medical simulator, recording chest compression frequency as the primary outcome parameter.
Results:
The study shows comparable results in all groups, with the exception of the chest compression frequency which was higher in the students’ and residents’ groups (students: 134.7/min ± 14.1; residents: 137.9/min ± 15.9; specialists: 126.3/min ± 19.3). Increased rates were not associated with lower depths (39.0 mm ± 8.2, 40.5 mm ± 9.7, and 38.1 mm ± 8.2), so the quality of compressions provided may be seen as equivalent in all the study groups.
Conclusion:
Our data suggest that medical students may be as effective as anaesthesia and intensive care specialists and residents in cardiopulmonary resuscitation training.
Introduction
Cardiovascular mortality is responsible for 30% of global deaths, 1 with an average survival rate of out-of-hospital cardiac arrest of 5%–7% in adults1,2 and 5.8% in paediatric patients. 2 Although most out-of-hospital cardiac arrests occur at home, many of them occur in public places such as train stations, shopping malls, museums and sport-related facilities3,4 which are frequented by teenagers. Increasing the number of potential rescuers in out-of-hospital cardiac arrest in public places is one of the goals that have been largely accepted and discussed.5–8 Offering effective and low-cost mass-training to lay-rescuers is an ideal embraced by trainers, researchers and society. 9 One of the most important steps in increasing the rate of bystander resuscitation worldwide, emphasised in the new resuscitation guidelines, is to educate all school children. 10 High school students seem to be a good target for training programmes 11 because young people have a positive attitude towards learning 10 and their presence in public areas is significant. Key elements in this type of training programmes are the ability of the trainee to quickly recognise cardiac arrest and to be able to apply good chest compressions with an appropriate depth and frequency of compressions.5,12 Different trainers have been used for these programmes: trained high school teachers, medical students, resident doctors, specialist doctors, nurses;9,11,13–17 the only common request is compliance with the key elements described.
Using medical students to train cardiopulmonary resuscitation (CPR) to high school students is an attractive idea and has been proven to be effective.13,16,18 They are seen as a good trainer alternative as they are perceived as role models by high school students. The low age difference between them and the trainee is believed to be beneficial. 17 Also it seems that acting as trainers could also be beneficial for the medical students who subsequently improve their own CPR skills. 19 Recently, it has been proposed that teaching basic life support (BLS) should be part of their medical training curriculum. 13 No definitive conclusion has been drawn until now whether the medical competence of the trainer makes any difference with regard to CPR training of high school students. 12 The current guidelines do not include a recommendation regarding who should do the training. 10
In our hometown, Cluj-Napoca, Romania, we developed a volunteer-based programme to train high school students in basic CPR skills. The trainers were medical students, with basic CPR training completed during the ‘Medical First Aid’ discipline, mandatory in the first year of their medical school. All the volunteers received basic training in theoretical teaching and practical training of CPR to others, offered by a member of the Anaesthesia and Intensive Care Department experienced in ‘train the trainers’ programmes. So far, in the 3 years of running the programme, we have trained more than 1300 high school students. We wanted to know whether we could expect different results of this training using trainers with a higher medical competency level.
Methods
Study design
After obtaining the approval from the local educational authority (Cluj County School Inspectorate), and Târgu Mureș University of Medicine and Pharmacy’s Ethical Committee, we randomly selected 12 tenth-grade high school classes to receive training in BLS. The trainer groups consisted of four medical students, four resident doctors and four specialists. All of them were members or collaborators of the Anaesthesia and Intensive Care Department of the University. The students were members of the on-going volunteer programme offering CPR training to high school students; they were selected from the third and fourth year in the medical university; they were trained in teaching CPR by a member of the Anaesthesia and Intensive Care Department and they had previously participated as trainers in standardised CPR training sessions. They were selected based on their willingness to participate in the study. The residents were part-time staff from the Anaesthesia and Intensive Care Department; selected from the fourth and fifth training year and they had a minimum of 1 year of experience as trainers in the ‘practical abilities’ laboratories where they had been demonstrating the specific manoeuvres from the curriculum to the third- and sixth-year medical students. The specialists were full-time or part-time members of the Anaesthesia and Intensive Care Department and were experienced in teaching students from the ‘Anaesthesia and Intensive Care Discipline’ curriculum and the ‘First Aid for students’ discipline. The trainers were randomly assigned to one of the high school classes using an online application (Research randomiser – https://www.randomizer.org/). The intervention occurred at the cluster (class) level and outcomes were measured at the individual level. A formal sample size calculation was conducted using the software located at http://www.sealedenvelope.com/power/binary-noninferior/. We designed the study as a non-inferiority trial test.
Outcome measures
The purpose of this non-inferiority trial was to compare medical students with residents and specialist doctors as trainers for CPR, with the objective of showing non-inferiority. We considered our primary outcome measure to be ‘compression rate’, and we defined ‘success’ a compression rate over 100/min. We used the significance level of 5% and power of 80%; 20 we assumed equal percentage of ‘success’ rates in both control and experimental groups of 95%, and we accepted a confidence interval ‘delta’ of 10%. The computed value was 59 minimum participants per group. We included four classes per group to compensate the effect of the ‘follow-up loss’. 20 Our anticipated sample size per arm was also comparable to previous studies with a similar design.21,22 All the students and at least one of their parents signed an informed consent. The principal of the high school and the teachers were informed and the study was approved.
All the students received the same multiple-choice questions (MCQ) questionnaire to test their previous knowledge in CPR to be sure that there was homogeneity between the groups. After the MCQ test, they received 1 h of theoretical training sustained by the designated trainer. After 1 week, they received practical training, with the same trainer. The Little Anne® CPR training manikin (Laerdal, Norway) was used for training. The sessions were conceived according to the European Resuscitation Council Guidelines 2010, and they were focused on correct steps in diagnosing cardiorespiratory arrest, activating emergency response and providing correct CPR with thoracic compressions only. While completing the study, European Resuscitation Council Guidelines 2015 were made available. The new guidelines include the same key recommendations relating to BLS and training, so we did not perform changes in our study, considering it was still actual and of interest. The Anaesthesia and Intensive Care Department members and collaborators use the same curricula when they are teaching CPR to non-medical personnel, so all of the trainers participating in the study were familiar with the content of the course. Before the start of the study, a briefing was organised with all the trainers. The trainers were given the same presentation as support for the lectures and instructions to teach as they normally do and were given the freedom to personalise their teaching skills as long as they respected the resuscitation protocol. For the practical session, they were instructed to focus on the correct steps in diagnosing cardiorespiratory arrest, activating emergency response and providing correct CPR with thoracic compressions only. They were instructed to demonstrate the procedure and to allow trainees to practise under the trainers’ supervision. They were also instructed to allow time for individual practice for every student until they both, the trainer and the trainee, were satisfied with the trainee ability to provide CPR. They were allowed to demonstrate the manoeuvres again during the training sessions as many times as they considered necessary. The trainees were told that in the following weeks, not later than 4 weeks, their knowledge and skills regarding CPR would be evaluated, and they were asked not to prepare. The trainees were evaluated by an independent evaluator 2 weeks after the completion of the training. They were asked to complete another MCQ test, different from the initial test. All students in the three groups were asked the same questions. To exclude bias, the initial and final MCQ questionnaires were conceived by an independent evaluator who had not taken part in the training of students and the trainers were not permitted access to these beforehand. Following the test, the CPR skills were evaluated, using a Resusci Anne® (Laerdal, Norway) manikin with a SkillReporter™ (Laerdal, Norway) device attached. The SkillReporter™ (Laerdal, Norway) device had been previously used for the objective assessment of CPR training23,24 and allowed us to record objective data regarding the trainee’s ability to provide CPR: compression frequency, flow fraction, no flow time and mean compression depth. The software SkillReporter™ (Laerdal, Norway) device records data in a graphic and numeric mode that can be analysed later with Session Viewer Software. Objective data regarding the CPR skills of each of the participants were recorded. The scenario lasted 120 s.
Statistics
The recordings of MCQ tests and the data recorded by the SkillReporter™ were separated into three groups: trained by students (Students), trained by residents (Residents) and trained by specialist (Specialists). Imputation was performed using Excel® (Microsoft Corporation, Redmond, WA, USA). Statistical analysis was performed by GraphPad Prism® 6 software: we analysed the distribution of recorded data with the D’Agostino Pearson normality test and we compared the groups using the student t-test, Kruskal–Wallis test and analysis of variance (ANOVA) test accordingly.
Results
The initial study group consisted of 296 high school students, aged around 15 years (91 in the Specialist group with a mean age of 15.4 years; 108 in the Resident group with a mean age of 14.8 years and 97 in the Student group with a mean age of 15.1 years) who had returned the informed consent signed by themselves and their parents and had agreed to be included in the study. There were 55.6% girls in the Specialist group, 57.4% girls in the Resident group and 55.7% girls in the Student group. All of them answered the preliminary MCQ test and received practical and theoretical training. None of the participating students had been previously trained in providing CPR. The results from the initial test showed means of 39.2% (standard deviation (SD): 10.8%) correct answers in the Specialist group, 40.7% (SD 11.5%) correct answers in the Resident group and 39.5 (SD 12.4%) in the Student group indicating poor knowledge of CPR. Because of the normal distribution of every group evidenced by the D’Agostino Pearson normality test, the ANOVA test was used to compare the means, and a p value of 0.415 was computed, indicating no statistically significant difference between the three groups.
We did not want the students to prepare for the examination, so we did not announce the precise examination date and time. For the post-course MCQ test, 222 students from the initial study group were available, 64 in the Specialist group, 94 in the Resident group and 64 in the Student group. The means were 76.8% (SD 10.7%) correct answers in the Specialist group, 78.5% (SD 7.4%) correct answers in the Resident group and 78.5% (SD 8.9%) correct answers in the Student group (Table 1) Because of the abnormal distribution in the Student and Resident group, the Kruskal–Wallis test was used to compare the means, and the p value of 0.819 was computed, showing no statistically significant difference between the groups.
Results of MCQ tests after the lecture (percentages of correct answers).
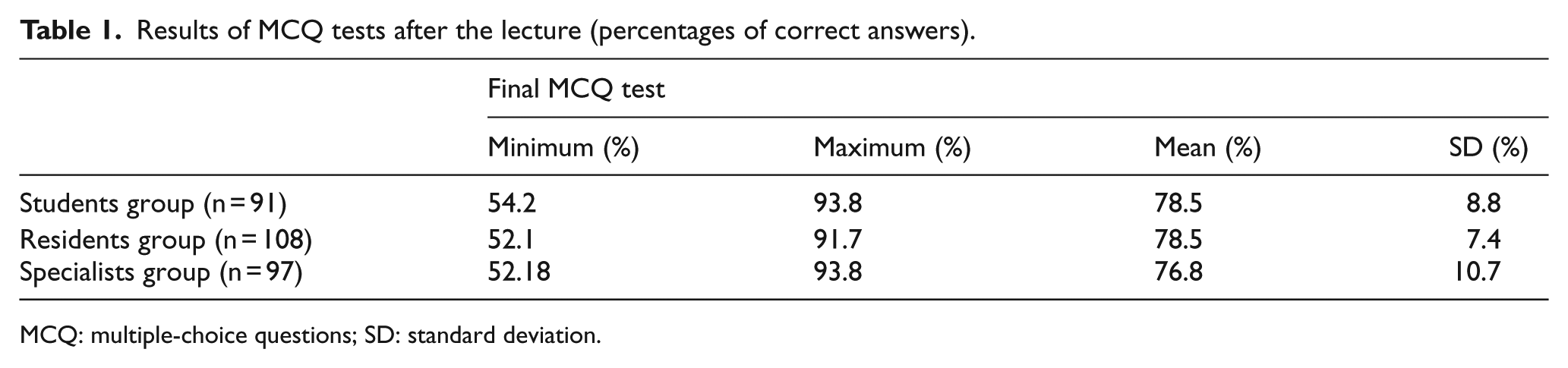
MCQ: multiple-choice questions; SD: standard deviation.
Only 204 students from the initial study group were available for practical evaluation, 62 in the Specialist group, 73 in the Resident group and 69 in the Student group. The recordings for the flow fraction, no flow time and mean compression depth were similar in all three groups (Table 2). We compared the means with the use of the Kruskal–Wallis test for the flow fraction and the no flow time and with the ANOVA test for the mean compression depth, as indicated by the p values on the D’Agostino & Pearson omnibus normality test. The p values computed when comparing the means were 0.271 for the flow fraction, 0.795 for the no flow time and 0.277 for the mean compression depth showing no statistically significant difference between the three groups.
Flow fractions, no flow time, frequency of compressions and mean compression depth analysis.
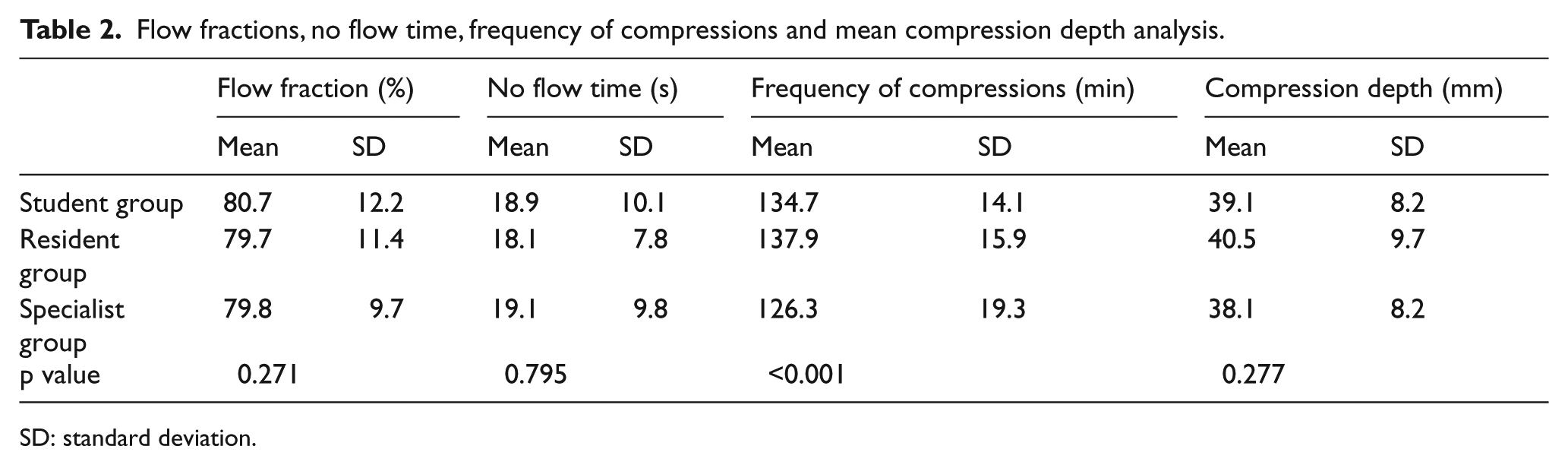
SD: standard deviation.
Analysing the mean frequency of compressions, we found that the Student group had a mean of 134.7 compressions per minute (SD: 14.1/min), the Resident group had a mean of 137.9 compressions per minute (SD: 15.9/min) and the Specialist group had a mean of 126.3 compressions per minute (SD: 19.3/min; Table 2). Because of the normal distribution in all three groups, we compared the means using the ANOVA test, and we obtained a value of p < 0.001, showing a significant difference between the three groups. Turkey’s multiple comparison test was applied for post hoc analysis and the following adjusted p values were obtained: p = 0.0002 Specialists versus Residents, p = 0.01 Specialists versus Students and p = 0.46 Residents versus Students. These results are showing a significant difference between the Student and Specialist groups and between the Resident and Specialist groups and no difference between the Student and Resident groups; 6.5% of the students trained by specialist doctors and 2.7% of the students trained by resident doctors recorded chest rates lower than 100/min, but all the students trained by medical students recorded higher than 100/min chest rates.
Discussion
Good quality chest compressions are considered the core element of the BLS curriculum. 10 Quality of chest compressions is related to the trainee’s ability to adhere to the recommended rate and depth. When evaluating the quality of chest compressions in real situations, studies have shown that this is often suboptimal 25 although it is improved after implementation of 2010 protocols. 26 The European Resuscitation Council recommends in the current resuscitation guidelines that chest compressions should be provided at a rate of 100–120/min to increase survival. One major finding of our study is that the students trained by specialist doctors performed CPR with a lower frequency, closer to the one recommended by the European Resuscitation Council. We believe that several explanations could be possible: First, specialist doctors, when teaching, could be more aware about the importance of keeping the frequency of chest compressions in the 100–120/min interval, whereas for junior doctors and medical students, ‘push hard, push fast’ seems acceptable. Second, it is possible that junior doctors and medical students are not aware of the difference between a higher and a lower frequency.
The ‘push hard push fast’ approach is acceptable in some training programmes for lay persons. Studies show that it may increase the effectiveness of chest compressions,23,27 but some researchers and trainers may not agree. 28 The latter may be tempted to affirm that medical students and residents should not be allowed to do CPR training because they tend to train to push too fast. Yet, we need to notice that while the Specialist group is closer to the European Resuscitation Council recommendations, a small number of participants from this group recorded chest compressions rates lower than the generally acceptable limit of 100/min, while none of the Student group passed this lower limit. It is hard to draw any conclusions of this finding at the population level and we suggest that supplementary studies are needed. We suggest that proper training may adjust the training skills and medical students and residents may be as effective trainers as specialist doctors. Also additional solutions could be taken into consideration such as using a metronome 29 or the rhythm of a well-known song.30,31 The main advantage in using medical students is their availability and eagerness to volunteer which makes them a valuable resource for this type of training programmes.
Because we did not use the same test for pre- and post-course evaluation of knowledge, and the tests we used were not validated, we suggest that the data reported for theoretical knowledge should not be used as a measure of the effectiveness of the training provided. The role of the first test was to investigate whether the students in all the three groups had the same level of previous knowledge and the final test was intended to investigate whether the effect of the training is similar, regarding the professional level of the trainer. We found no statistically significant difference between the groups regarding the knowledge level of trainees suggesting that when teaching CPR, the medical degree of the trainer is not a factor. However, we observed that the Specialists group had a tendency to a smaller mean and a higher SD after training. Although not statistically relevant, we suggest that this is happening because specialist doctors use a different language when teaching, more technical, making the individual background of every student important in knowledge acquisition.
We found no difference in flow fraction, no flow time and mean compression depth between the study groups. This demonstrates that the BLS skills of trainees are similar regardless of the medical competency level of the trainer. We believe that the values we recorded for chest compressions around 40 mm (Table 2) are acceptable as they are similar with the values recorded by other authors studying CPR training in the same age population, 22 and it is accepted that manikin accelerometers record lower values for depth. 32 Also, we found no study to compare the depth of the same individual in manikin versus humans, and the current recommendation to push 50–60 mm was not proven to be superior in terms of survival to the older recommendation to compress 38–51 mm. A large study of out-of-hospital cardiac arrest shows better survival rates for the depth interval of 40.3–55.3 mm suggesting that the current recommendation to push 50–60 mm may be too high. The uniform recommendation to push 50 mm might not be appropriate because residual internal chest depth might be too low in some adults. 33 The usefulness of a fixed chest compression depth should be the content of further investigations. 26
Limitations
In our study, the endpoint for compression rates is higher than 100/min according to previous guidelines, available when the study was initiated. In the new guidelines, European Resuscitation Council recommends that the compression rate should be maintained between 100 and 120/min stating that a higher compression rate was found to be associated with a declining compression depth.34–36 In our study, higher rates in the Residents and Students groups were not associated with lower depths, so the quality of compressions provided may be equivalent in all the study groups.
We faced a high level of dropping out when we tested the students, which might be a major limitation for our study (Table 3). The reason for that may be that we did not announce a precise date or time when we would test our subjects because we did not want them to prepare anything to reduce the bias. We wanted to test only the effect of the initial training not the effect of self-studying and supplementary preparation. The unwanted result of this approach was that during the examination, some students had different appointments they could not postpone or they were just simply missing their classes that day. This explains the high level of dropping out. Another limitation may be the fact that we used the 120-s scenario for the final evaluation; we did that to avoid recording a fatigue effect. CPR provider fatigue is an accepted factor that decreases the effectiveness of CPR, and it is has been proven that it can be installed as early as 1.5 min after the beginning of chest compressions. 37 We found no data regarding the fatigue installation on a 15-year-old rescuer providing uninterrupted chest compressions but we assumed that using a 120-s scenario might be a reasonable approach.
Numbers of participants/study arm in each stage of the study.

MCQ: multiple-choice questions.
Conclusion
We conclude that medical students are an acceptable alternative as CPR trainers for high school students. Involving them in training programmes may increase the number of educated potential life-saviours, without decreasing the quality of training provided.
Footnotes
Acknowledgements
The authors would like to thank the following: all the students from the Road Safety Team for their dedication in teaching BLS, the members of the Anaesthesia and Intensive Care Department of the Iuliu Hațieganu University of Medicine and Pharmacy, Cluj-Napoca for their consent to teach in the programme and to Sally Wood Lamont for reviewing the English version of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.