
Abstract
Background:
Hollow organs perforation is a life-threatening condition. Early diagnosis and emergent intervention are important. Bedside ultrasound may be an alternative diagnostic tool for this condition.
Objective:
The aim of this study was to explore the diagnostic value of ultrasound of pneumoperitoneum in emergent or critical conditions through meta-analysis.
Methods:
PubMed, EMBASE, and Cochrane Library were systematically searched for potential studies. Then, two reviewers performed the processes of study selection, data extraction, and quality assessment independently. Finally, diagnostic indexes were analyzed with STATA 12.0 software (Serial No. 40120519635).
Results:
A total of five studies with moderate to high quality were eligible for meta-analysis. The pooled sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio and their 95% confidence interval were 0.91 (95% confidence interval = 0.86–0.94), 0.96 (95% confidence interval = 0.75–0.99), 22.05 (95% confidence interval = 3.10–156.96), and 0.10 (95% confidence interval = 0.07–0.15), respectively. The area under the summary receiver operating characteristic curve was 0.92 (95% confidence interval = 0.90–0.94).
Conclusion:
Abdominal ultrasound is a useful alternative tool in diagnosing of pneumoperitoneum. However, due to limited evidence, it is not yet indicated for routine clinical use.
Background
Hollow organs perforation is a life-threatening condition and may need emergent intervention. 1 The abdominal upright posteroanterior abdominal X-ray is traditionally regarded as the first choice for these patients. However, only 55%–85% of pneumoperitoneum could be detected by abdominal X-ray plain film.2,3 Computed tomography is more accurate than plain radiography, but it is not cost-effective and associated with more radiation exposure.3,4
Ultrasonography, because of its mobility and ease of use, may be an alternative choice for diagnosing of pneumoperitoneum. Several studies with limited sample size reported the ability of ultrasonography in diagnosing of pneumoperitoneum.4–8 But there was significant controversy among these studies. The aim of this meta-analysis was to explore the diagnostic value of ultrasound of pneumoperitoneum in emergent or critical conditions.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement (Supplementary Appendix 1) was used to perform this study. And this study was not registered.
Literature search
The search strategy was developed according to the following inclusion criteria:
Patients. Patients who were suspected of hollow viscera perforation.
Intervention. Abdominal ultrasound.
Control. Surgery, abdominal plain film, abdominal computed tomography, or follow-up.
Outcome. True-positive number, true-negative number, false-positive number, false-negative number, or other indicators, which could be used to calculate the above-mentioned endpoints. PubMed, EMBASE, and Cochrane Library were systematically searched from their inception to 2017. In addition, the bibliography of related original articles and reviews were examined for additional articles. Besides, we searched Clinicaltrial.gov for ongoing and unpublished studies. There was no language limitation. The following key words were used: pneumoperitoneum, perforation, ultrasound, ultrasonography, ultrasonographic, and sonographic.
Study selection and data extraction
Two authors performed the study selection and data extraction processes independently. And the study selection was done rigorously through three steps. Step 1: Excluding duplicated articles obtained by different databases; Step 2: Excluding non-relevant articles according to titles and abstracts; and Step 3: Selecting eligible studies by reading the remaining articles in full-text. Then, the first author name, country, study type, sample size, maneuver of abdominal ultrasound, golden standard, the above-mentioned outcome endpoints, and other indicators, which were necessary for study quality assessment, were extracted. Any disagreement was resolved by discussion.
Quality evaluation
The quality of eligible studies were assessed using The Quality Assessment of Studies of Diagnostic Accuracy included in Systematic Reviews-2 (QUADAS-2) tool (http://www.bris.ac.uk/quadas/quadas-2/), which is recommended by The Cochrane Diagnostic Test Accuracy Working Group.
Data analysis
The sensitivity, specificity, and positive and negative likelihood ratios (LR) were pooled using the bivariate mixed-effects binary regression model. And area under the summary receiver operating characteristic (sROC) curve (AUC) was calculated. The heterogeneity was evaluated with I2 statistic quantitatively and Chi-square test qualitatively. And I2 > 50% or p < 0.1 suggested significant heterogeneity. In addition, Fagan plot was developed using Bayes’ theorem to estimate the post-test probability of hollow organs perforation. A Deeks’ funnel plot of the diagnostic odds ratio against study size was used to evaluate publication bias if the number of included studies is more than 10en (http://training.cochrane.org/handbook).
Results
Study identification and characteristics
A total of 530 studies were retrieved. After removing irrelevant articles, 13 studies were read in full test. Finally, five studies were eligible for meta-analysis,4–8 and the whole procedure of literature screening is shown in Figure 1.
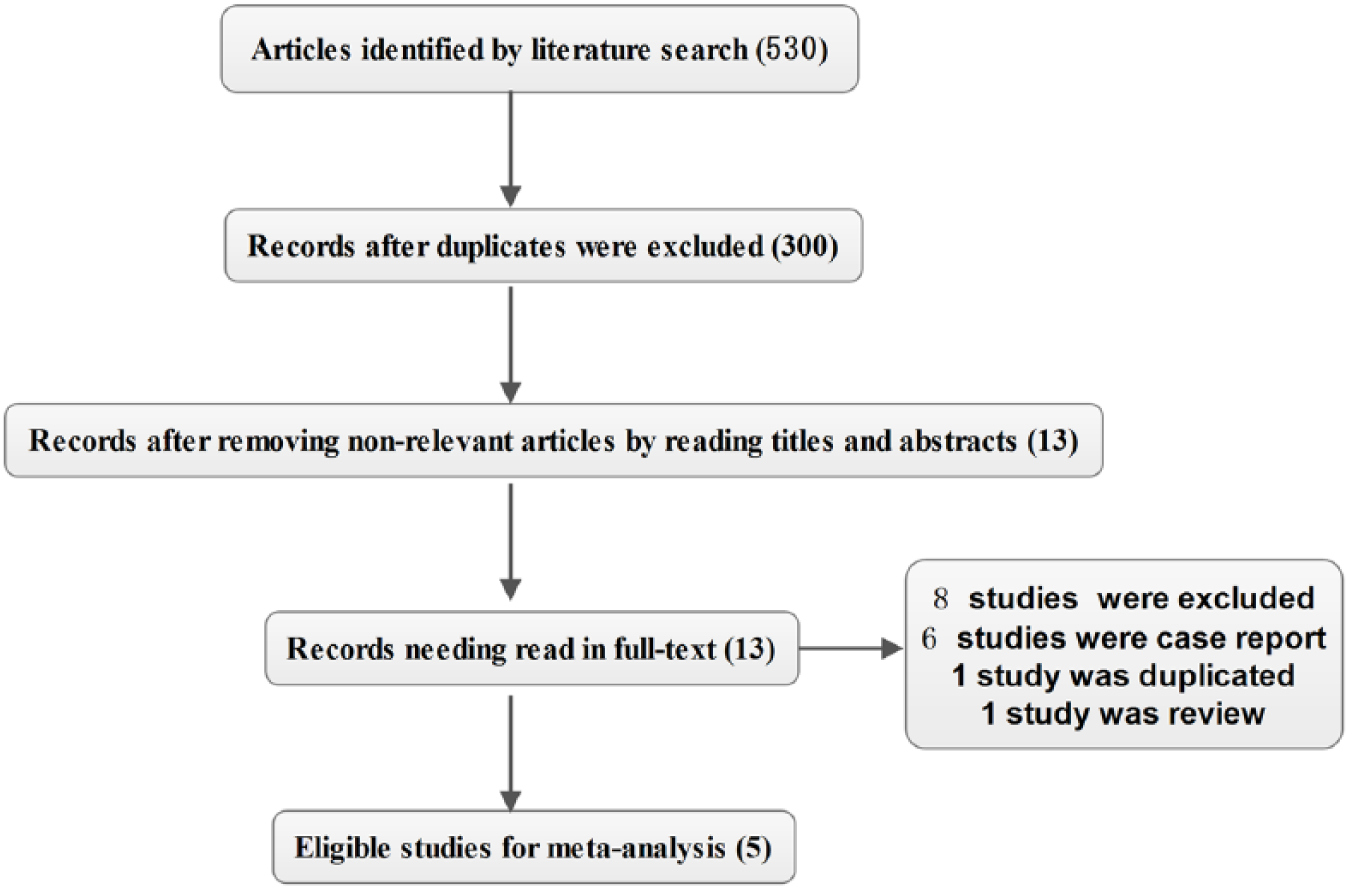
Flowchart of study selection for inclusion in the systematic review.
These included studies published between 2002 and 2015. The sample size ranged from 22 to 600. Patients with acute abdominal complaints or abdominal trauma history or who were suspected of hollow organ perforation were included. Tables 1 and 2 show the detailed information of included studies.
Characteristics of included studies.
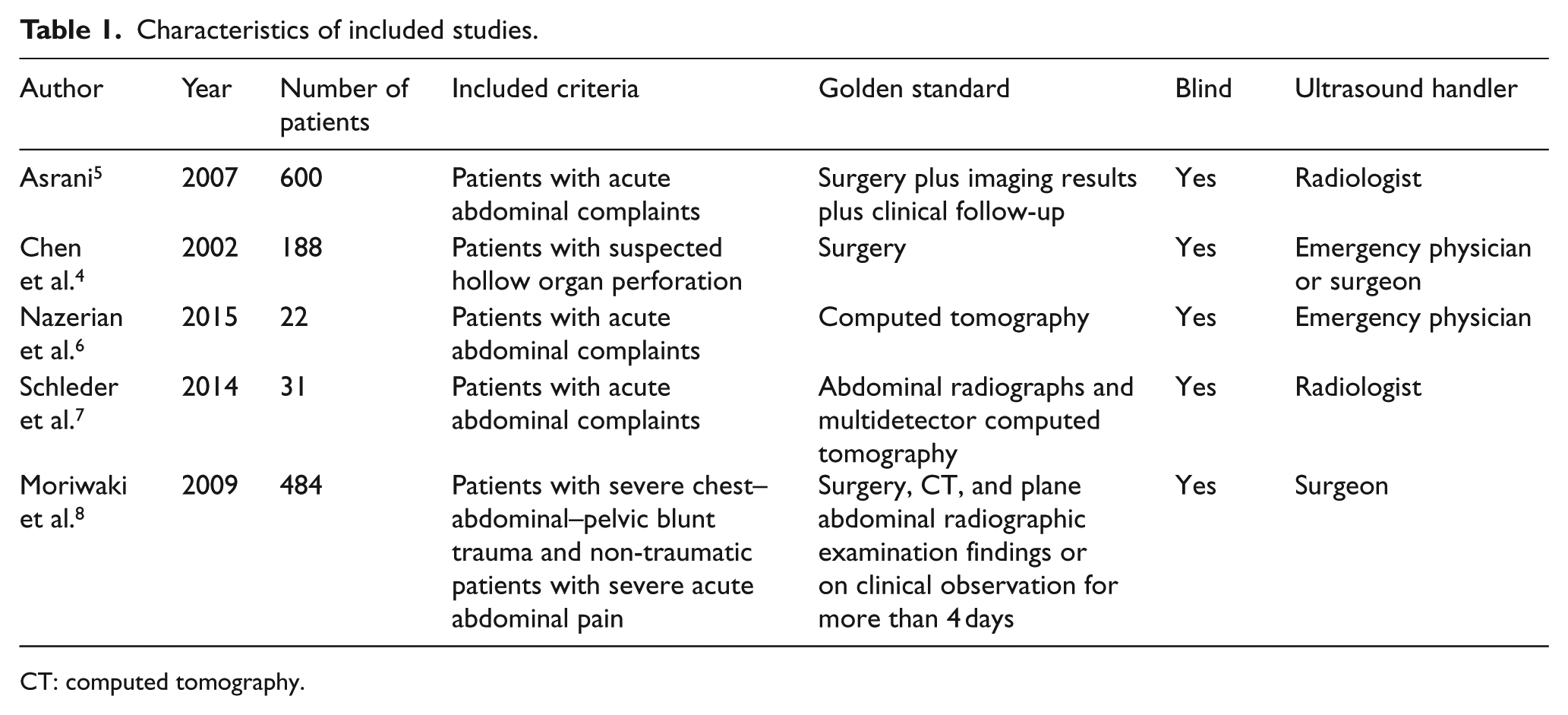
CT: computed tomography.
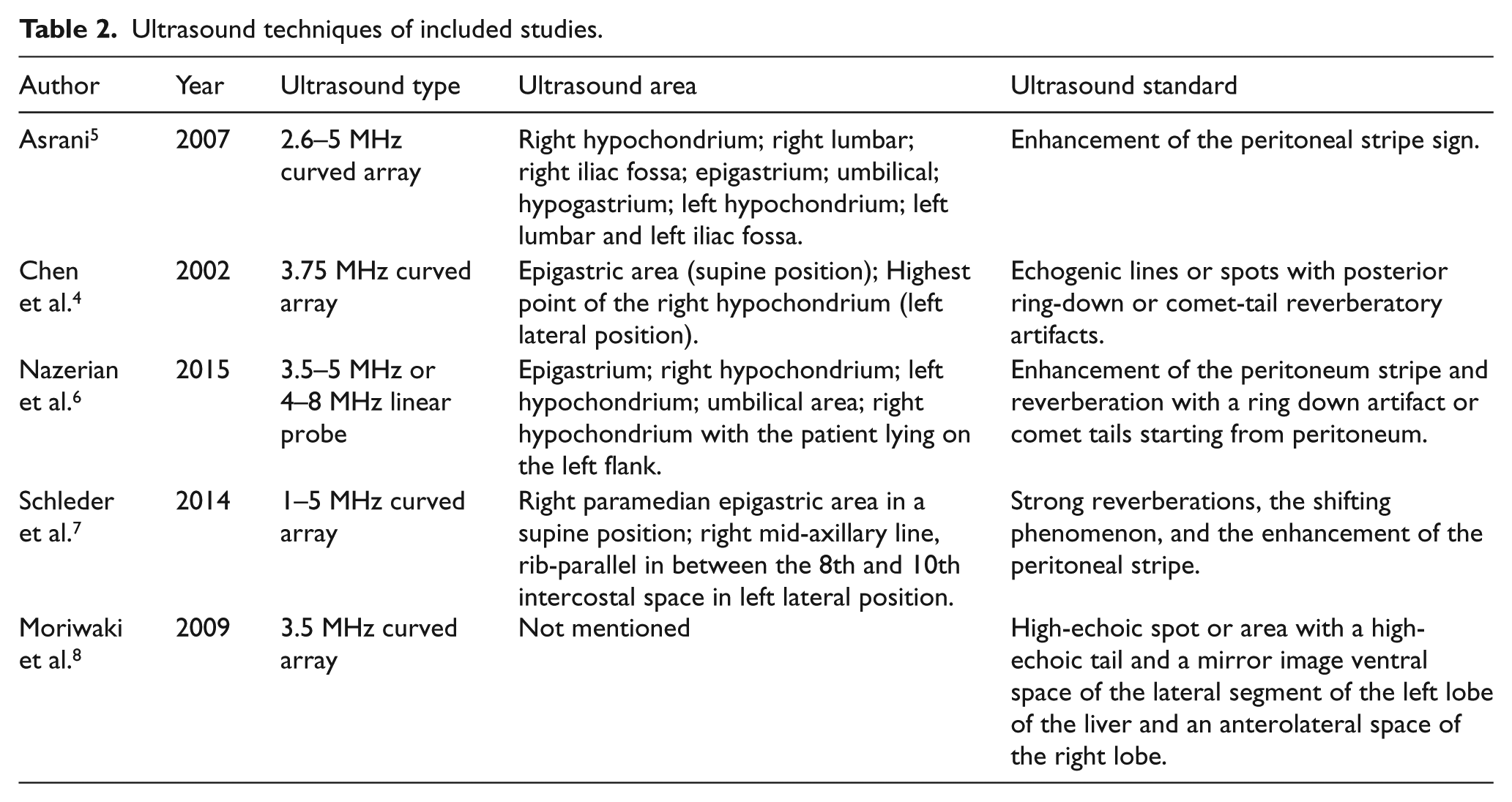
Ultrasound techniques of included studies.
Quality of included studies
The detailed information of included studies’ quality is shown in Supplementary Appendix 2.
Meta-analysis
There was significant heterogeneity between studies, and random-effect model was used. The pooled sensitivity, specificity, positive LR, and negative LR and their 95% confidence interval (CI) were 0.91 (95% CI = 0.86–0.94), 0.96 (95% CI = 0.75–0.99), 22.05 (95% CI = 3.10–156.96), and 0.10 (95% CI = 0.07–0.15), respectively (Figures 2 and 3). In addition, AUC was 0.92 (95% CI = 0.90–0.94; Figure 4).
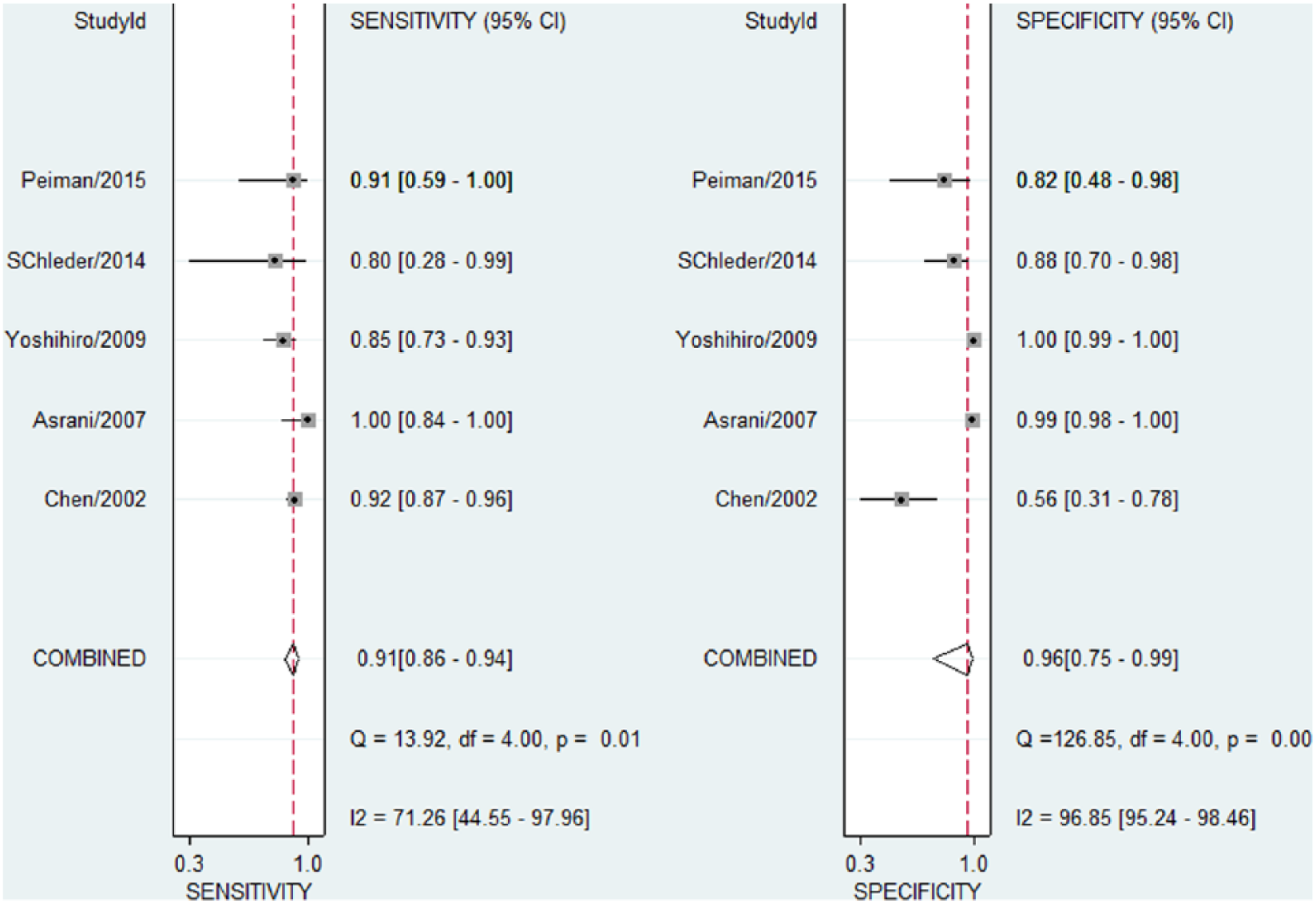
Pooled sensitivity and specificity.
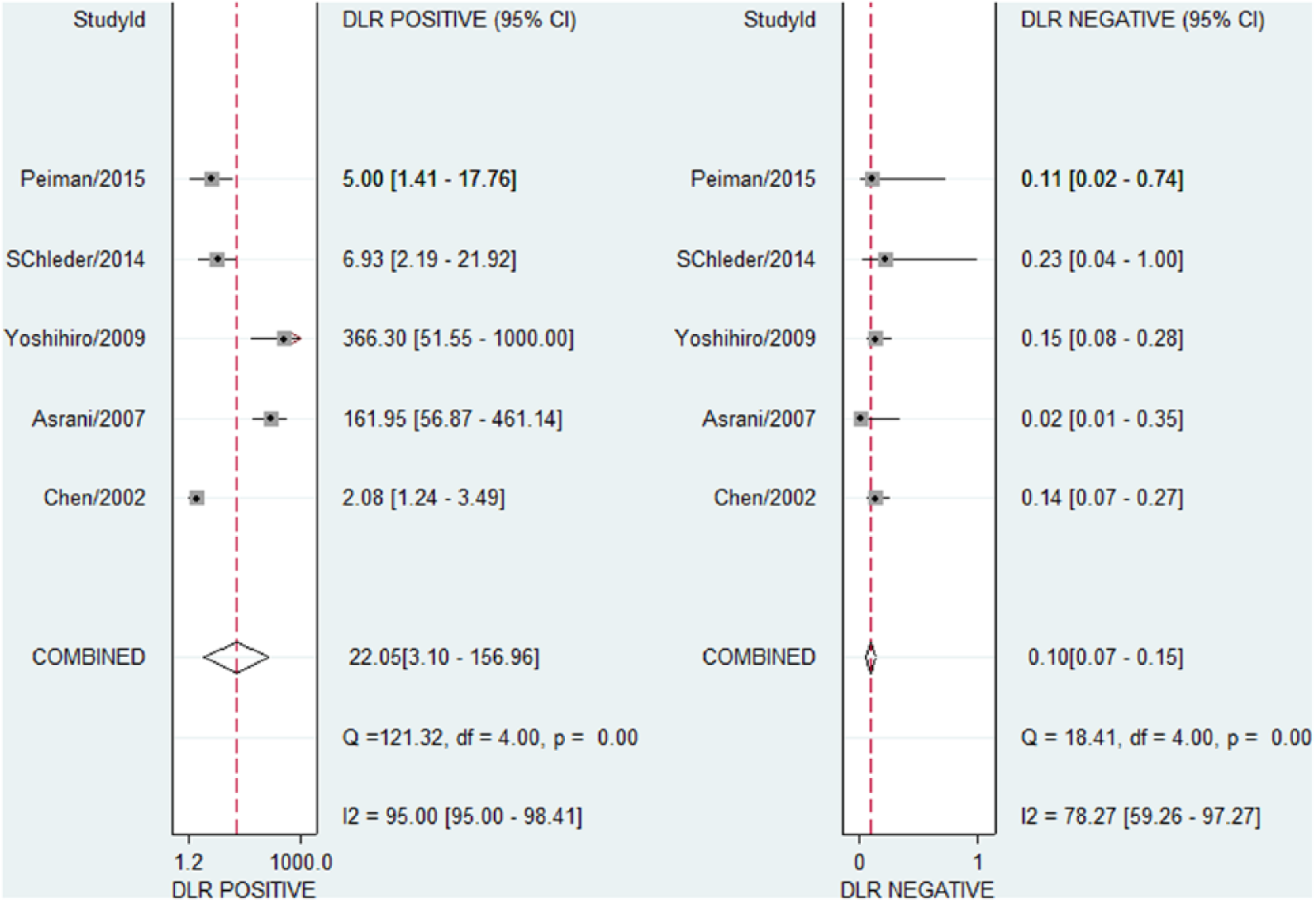
Pooled positive/negative likelihood ratio.
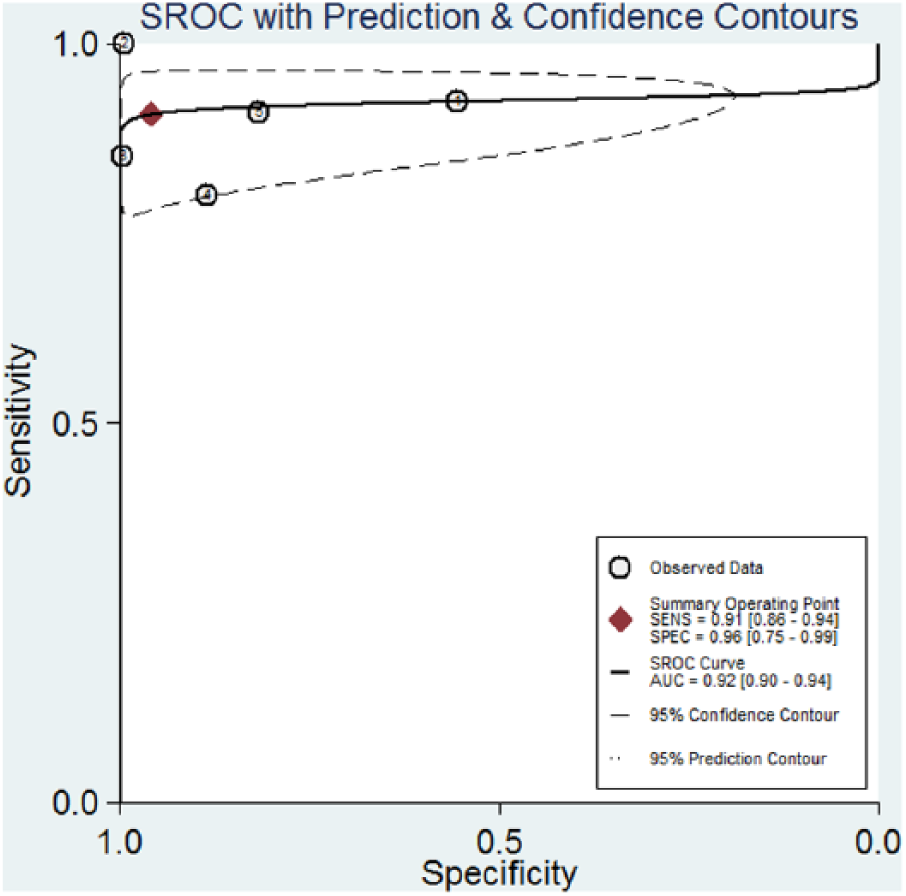
Area under the receiving operating characteristic curve.
The Fagan plot showed the relationship between the prior probability, the LR (combination of sensitivity and specificity), and posterior test probability. In this study, the prior probability was set as 1%, based on the study by Nazerian et al. 6 The risk of pneumoperitoneum rose from 1% to 18%, when the results of abdominal ultrasound were positive; and the risk of pneumoperitoneum decreases from 1% to 0%, when the results of abdominal ultrasound were negative (Figure 5).
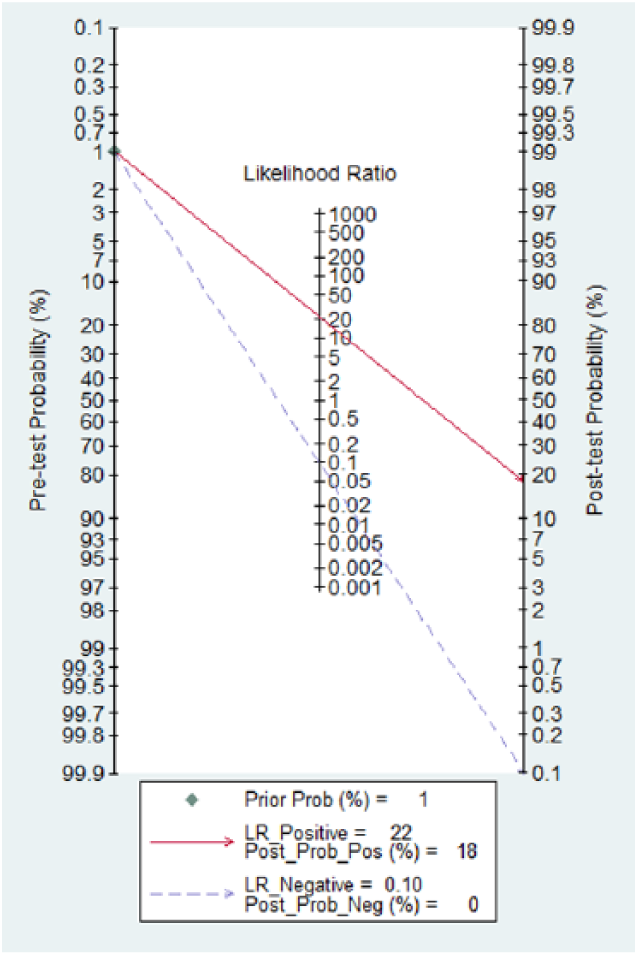
The Fagan plot analysis to evaluate the clinical utility of abdominal ultrasonography for the detection of pneumoperitoneum.
Due to the limited number of included studies, it was difficult to assess the publication bias.
Discussion
Emergent diagnosis and intervention are crucial for pneumoperitoneum, which often results from perforated hollow viscus. Results of the present meta-analysis indicated that the accuracy of ultrasound in diagnosing pneumoperitoneum is high.
Although erect abdominal plain radiograph is regarded as the standard method for diagnosing of pneumoperitoneum. It is reported that 20%–62% of hollow viscus perforation might be missed by abdominal plain film.9,10 In addition, patients are often too sick or debilitated to stand up for erect abdominal plain film. Some researchers reported that a supplementary left lateral decubitus radiograph of the abdomen might be useful, but it could not be used for accurate assessment of the extent of pneumoperitoneum.9,11 Abdomen computed tomography is more accurate in diagnosing pneumoperitoneum than abdomen plain film. Some studies showed that 83%–100% of pneumoperitoneum could be diagnosed through computed tomography scan. 4 However, it could not be performed bedside, is not cost-effective for screening pneumoperitoneum in patients with acute abdomen, and is associated with a higher radiation dose exposure.
In recent years, ultrasound is more used in emergency department and intensive care unit for evaluating various conditions. Focused assessment with sonography for trauma (FAST) has been recommended as standard procedure in multiple trauma patients.12–14 Ultrasound used for diagnosis of pneumoperitoneum has been reported in several studies and case reports.4–8,15,16 Some studies even found that ultrasound is as effective as plain radiograph in diagnosing pneumoperitoneum.4–8,17–25 In one study, the authors pointed that ultrasound performed by a surgeon in the emergency department could reduce the number of further examinations and shorten the time to surgery. 15 But due to the limited number of researches and inconsistent reported sensitivity and specificity, ultrasound has not been integrated into the standard diagnostic process of pneumoperitoneum.
Based on the results of the present meta-analysis, ultrasound is not bad in diagnosing pneumoperitoneum compared with plain radiograph. And Chen et al. 4 in their study found that the ability to detect gas was similar between ultrasound and plain film, when the final diagnosis is lower gastrointestinal perforation. However, ultrasound is much superior to plain radiograph in detecting abdominal free air, which comes from perforated upper gastrointestinal tract. 4 The biggest advantage of ultrasound is that it can be done at the bedside, without the need to transport patients. This is important in emergency department and intensive care unit, because most of the patients in these departments are not considered suitable for transport (hemodynamic instability, etc.). In addition, its mobility makes ultrasound desirable in prehospital phase. 26 Third, ultrasound is useful in reflecting the dynamic change of disease, monitoring the effect of therapy and may help to predict the patient outcome. Fourth, ultrasound can find other diseases or injuries, which may be not obvious on plain film.4,11 Finally, ultrasound can be done without radiation exposure.
In addition, several disadvantages of ultrasound should be concerned. It is operator dependent. Both operator and interpreter should receive intensive training. In the United Kingdom, at least level 2 Royal College of Radiology training is necessary for detecting the sonographic features of pneumothorax, localized atelectasis, and pulmonary fibrosis. 27 Besides, ultrasound is also machine dependent. In one study, the authors compared the ability of hand-carried ultrasound and high-end ultrasound, and they found that the above two machines were comparable in diagnosis of pneumoperitoneum. But the image quality was slightly lower for hand-carried ultrasound compared to high-end ultrasound. 7 Ultrasonographic doctors are not always 24 h available in all centers, thus it is necessary to ensure that members of the group have adequate training and methodological support. Based on the principle of the ultrasound, abdominal free air must be differentiated from adjacent air-filled lung, air-filled bowel, and ribs artifacts. Therefore, it is necessary to change the patient’s position from supine to left lateral to confirm the impacts of the echo interference.4,28 Therefore, ultrasound used for diagnosis of pneumoperitoneum may not be the content of primary assessment and should be performed in the secondary assessment phase, after obtaining a guarantee of survival. 8
Limitation
There was significant heterogeneity between studies. Several points may explain the significant heterogeneity: (1) there are great differences in the research objects, (2) practitioners performing sonographic examinations often have different professional backgrounds, and (3) researchers have not yet reached consensus on standard procedures, including the best examination area and the best diagnostic criteria. 6 In addition, the limited number of included study may influence the generalizability of the present results. And further large clinical studies are required.
Conclusion
Abdominal ultrasound can accurately diagnose pneumoperitoneum. Incorporating the evaluation of pneumoperitoneum by ultrasound in the standard abdominal ultrasound protocol is promising. Currently, based on limited evidences, ultrasound should not be the sole tool for ruling in or ruling out the diagnosis of pneumoperitoneum.
Supplemental Material
HKJ805668_appendix1 – Supplemental material for The value of ultrasound in diagnosis of pneumoperitoneum in emergent or critical conditions: A meta-analysis
Supplemental material, HKJ805668_appendix1 for The value of ultrasound in diagnosis of pneumoperitoneum in emergent or critical conditions: A meta-analysis by Libing Jiang, Jing Wu and Xia Feng in Hong Kong Journal of Emergency Medicine
Supplemental Material
HKJ805668_appendix2 – Supplemental material for The value of ultrasound in diagnosis of pneumoperitoneum in emergent or critical conditions: A meta-analysis
Supplemental material, HKJ805668_appendix2 for The value of ultrasound in diagnosis of pneumoperitoneum in emergent or critical conditions: A meta-analysis by Libing Jiang, Jing Wu and Xia Feng in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors would like to thank Yongan Xu, PhD, Department of Emergency Medicine, Second Affiliated Hospital, School of Medicine, Zhejiang University, Jiefang Road 88, Hangzhou, China. Libing Jiang, Jing Wu, and Xia Feng contributed equally to this study.
Availability of data and materials
All data were in the article and supplementary files.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Libing, Jiang receive the funding of Zhejiang medical and health science and technology project (2017ky372). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.