
Abstract
Objective
Ultrasound provides real-time, high-resolution imaging and is increasingly recognized as a valuable diagnostic tool for clavicle fractures. Compared with traditional imaging modalities, ultrasound offers advantages such as point-of-care accessibility, absence of radiation exposure, and rapid diagnosis capability, making it particularly useful in emergency settings. However, the diagnostic performance of ultrasound across different clinical studies remains inconsistent. Therefore, this study aimed to systematically assess the diagnostic accuracy of ultrasound for clavicle fractures through a meta-analysis of existing studies.
Methods
A systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. A comprehensive search of PubMed, Scopus, Embase, Cochrane Library, and Web of Science was performed until 25 February 2025. Studies reporting the sensitivity, specificity, and overall diagnostic performance of ultrasound for clavicle fractures were included. Data extraction and statistical analysis were performed using Stata version 18.0.
Results
A meta-analysis of seven eligible studies showed a pooled sensitivity of 92% (95% confidence interval: 87%–95%) and pooled specificity of 95% (95% confidence interval: 91%–98%), indicating relatively high diagnostic accuracy. Sensitivity showed low-to-moderate heterogeneity, whereas specificity demonstrated significant heterogeneity. Fagan plot and likelihood ratio analysis supported the clinical utility of ultrasound for both confirming and excluding clavicle fractures. The likelihood ratio scattergram indicated that ultrasound shows good performance in ruling in clavicle fractures but only moderately good performance in ruling them out.
Conclusion
Current evidence indicates that ultrasound is a promising, noninvasive diagnostic modality for clavicle fractures, especially in emergency settings. Its diagnostic accuracy, coupled with its safety profile, makes it a potentially valuable tool. Nevertheless, standardization of scanning protocols and further validation in diverse populations are needed. Future studies are warranted to standardize scanning protocols, evaluate operator-dependent factors, and validate findings across broader clinical settings.
Introduction
Clavicle fractures are among the most common skeletal injuries encountered in the emergency department (ED), frequently resulting from falls, sports-related trauma, motor vehicle accidents, and birth-related injuries in neonates.1,2 Notably, the incidence of neonatal clavicle fractures related to birth trauma ranges from 0.2% to 4.4% in developed countries and from 0.14% to 0.46% in developing regions.3–6 Prompt and accurate diagnosis is critical for guiding appropriate management; preventing complications such as malunion, nonunion, or neurovascular injury; and ensuring timely pain relief and immobilization. 7
Traditionally, X-ray has been the standard imaging modality for diagnosing clavicle fractures across all age groups, owing to its low cost, wide availability, and rapid acquisition. However, compared with ultrasound, X-ray has several limitations, including greater radiation exposure to both patients and healthcare workers and the possibility of missed diagnoses, especially in cases of subtle or nondisplaced fractures.1,8 In contrast, computed tomography (CT) provides high-resolution three-dimensional reconstructions, making them especially useful for evaluating complex fractures and assessing fracture displacement with greater precision. However, the higher radiation dose and cost associated with CT limit its feasibility for routine use, especially in neonatal and pediatric populations.9,10
Considering these limitations, clinicians increasingly seek reliable, noninvasive imaging methods—such as ultrasound—as an alternative to X-ray and CT for at-risk groups (e.g. neonates, children, and pregnant patients). Ultrasound imaging has increasingly gained recognition as an effective diagnostic modality for fracture evaluation, supported by a growing body of evidence demonstrating its accuracy and clinical utility.1,7,11 It enables point-of-care diagnosis, allowing emergency physicians to rapidly assess suspected clavicle fractures at the bedside without exposing patients to ionizing radiation.11,12 This is particularly advantageous for pediatric and pregnant patients, in whom radiation exposure should be minimized.13,14 Furthermore, ultrasound can reduce diagnostic delays, expedite clinical decision-making, and serve as an alternative when X-ray or CT is unavailable or impractical. 12 Additionally, ultrasound is sometimes used to detect occult fractures in pediatric patients, particularly when X-ray and CT fail to provide a definitive diagnosis. 15 The advantages of ultrasound include its radiation-free nature, real-time imaging capability, and excellent visualization of soft tissue injuries, making it a valuable supplementary tool in fracture assessment. 16
Despite its growing use, variability exists in the reported diagnostic accuracy of ultrasound, largely due to differences in operator expertise, scanning protocols, and reference standards (X-ray vs. CT) across studies.11,12,17–21 This inconsistency highlights the need for a comprehensive assessment of ultrasound’s diagnostic performance to inform clinical decision-making. Therefore, a systematic evaluation of existing evidence is necessary to determine the true diagnostic performance of ultrasound for clavicle fractures in the ED. This meta-analysis aimed to compare the pooled sensitivity, specificity, and overall diagnostic accuracy of ultrasound with those of conventional imaging, providing evidence for its clinical utility and potential integration into emergency care protocols.
Methods
According to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement, 22 a systematic literature search was conducted on 25 February 2025. This search was conducted in PubMed, Scopus, Embase, Cochrane Library, and Web of Science databases to identify studies evaluating the diagnostic accuracy of ultrasound for clavicle fractures. This systematic review was prospectively registered in PROSPERO under the registration number CRD 42025643069. The search strategy included a combination of Medical Subject Headings (MeSH), Emtree terms, and free-text keywords to ensure the comprehensive retrieval of relevant studies. The search was limited to peer-reviewed, English-language publications. The following search terms were used with Boolean operators (AND, OR): for the population: “clavicle fracture,” “clavicular fracture,” or “clavicular injuries”; for the intervention: “ultrasound,” “sonography,” “point-of-care ultrasound,” or “POCUS.” Detailed search strategies tailored to each database are provided in Supplementary Attachment 1.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: (a) studies that involved patients with clavicle fractures; (b) those utilizing ultrasound as a diagnostic tool; (c) those reporting diagnostic accuracy metrics (e.g. sensitivity, specificity, and diagnostic odds ratio); (d) original research articles, including cross-sectional and case–control studies; (e) studies conducted in ED settings.
The exclusion criteria were as follows: (a) studies conducted on animals or those focusing on nonclavicle fractures; (b) review articles, editorials, and conference abstracts without original data; (c) studies with incomplete or missing diagnostic accuracy data.
Data extraction and quality assessment
Two independent reviewers screened the titles, abstracts, and full texts of the retrieved studies to identify eligible articles. Any discrepancies were resolved through discussion or by consulting a third reviewer. Extracted data included study characteristics (author, year, country, and population size), diagnostic accuracy metrics (sensitivity, specificity, area under the receiver operating characteristic curve), and methodological details.
The quality of the included studies was independently assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool. 23 This tool evaluated potential risks of bias and applicability concerns across four domains: patient selection, index test, reference standard, and flow and timing. The standardized assessment facilitated an objective evaluation of methodological rigor and helped identify possible sources of heterogeneity.
Statistical analysis
Meta-analysis was performed using Stata software (version 18.0, Stata Corp, College Station, TX, USA). Pooled estimates of sensitivity, specificity, and diagnostic odds ratios (DORs) were calculated using a random-effects model. 24 A summary receiver operating characteristic (SROC) curve was plotted to evaluate overall diagnostic performance. Heterogeneity among studies was assessed using the I2 statistic. 25 To explore diagnostic utility in clinical practice, we also conducted Fagan nomogram analysis and constructed a likelihood ratio scattergram. All statistical analyses were performed using the MIDAS user-written module for diagnostic test accuracy (DTA) meta-analysis. Statistical significance was defined as a P value less than 0.05.
Results
Screening and selection of articles
Employing a predefined search strategy, our systematic literature review initially identified 842 articles. After removing duplicates, 566 articles remained, which were screened based on their titles and abstracts. Of these, 551 articles were excluded as they consisted of case reports, conference abstracts, editorial comments, and reviews. Subsequently, 15 full-text articles were assessed for eligibility, leading to the exclusion of 8 articles that did not align with the study objectives. Ultimately, seven studies meeting the inclusion criteria were selected for final analysis.11,12,17–21 The entire screening process is summarized in a PRISMA-compliant flow diagram (Figure 1).

PRISMA flow diagram showing the review process. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Characteristics of the included studies and patients
Across the 7 studies, a total of 527 patients with clinically suspected clavicle fractures were included. Key study characteristics are summarized in Table 1. The analysis comprised five single prospective studies and two multicenter prospective studies, conducted in the United States (n = 4), the Netherlands (n = 1), and Turkey (n = 2). Among these, two studies focused exclusively on pediatric patients (<18 years),12,19 one study focused on adult patients, 21 and four focused on both adult and pediatric populations.11,17,18,20 Clinical settings varied across the studies, with five studies conducted in general EDs11,17,18,20,21 and two in pediatric EDs.12,19
Characteristics of the included studies and patients.

CT: computed tomography; ED: emergency department.
The reference standards used for confirming clavicle fractures also differed across studies. Four studies used plain radiography,11,12,17,19,21 one used CT, 20 and one employed a combination of radiography and CT. 18
Ultrasound devices and operators’ backgrounds are presented in Table 2. All studies utilized high-frequency linear transducers (4–15 MHz). All studies used point-of-care ultrasound conducted by emergency physicians.11,12,17–21
Characteristics of ultrasound devices, operators, and diagnostic measures in the included studies.

US: ultrasound.
POCUS operators included attending physicians, sports-medicine fellows, residents, and a fourth-year medical student.
Publication bias
To evaluate potential publication bias, Deek’s funnel plot asymmetry test was performed. The results indicated no significant publication bias among the included studies (P = 0.38), as shown in Figure 2.

Deek’s funnel plot asymmetry test.
Risk of bias and overall quality assessment
The QUADAS-2 assessment (Table 3) showed that most studies presented a moderate risk of bias, primarily in the domains of patient selection and flow and timing.
QUADAS-2 quality assessment of the included studies.

CT: computed tomography; QUADAS-2: Quality Assessment of Diagnostic Accuracy Studies-2.
Diagnostic performance analysis
Figure 3 shows the SROC curve of all included studies. The pooled sensitivity among the studies was 92% (95% confidence interval (CI): 87%–95%), and the pooled specificity was 95% (95% CI: 91%–98%), reflecting high diagnostic accuracy. The area under the curve (AUC) was 0.98 (95% CI: 0.96–0.99), indicating excellent test performance. Most studies clustered in the upper left quadrant of the SROC plot, suggesting consistently high diagnostic value despite variations in population and setting.

SROC curve for the diagnostic accuracy of ultrasound for clavicle fractures. AUC: area under the curve; SENS: sensitivity; SPEC: specificity; SROC: summary receiver operating characteristic.
Quantitative data synthesis
Forest plots and summary statistics are presented in Figure 4. The pooled sensitivity ranged from 0.82 to 1.00, with low heterogeneity across studies (Q = 6.75, df = 6, P = 0.34; I2 = 11.14%, 95% CI: 0%–100%) (Figure 4(a)). Specificity values ranged from 0.88 to 1.00, indicating low between-study heterogeneity (Q = 7.07, df = 6, P = 0.31; I2 = 15.12%, 95% CI: 0%–76.63%) (Figure 4(b)). Positive likelihood ratios ranged from 6.86 to 68.63, with no significant heterogeneity (Q = 6.10, df = 6, P = 0.41; I2 = 0%, 95% CI: 0%–100%) (Figure 4(c)), indicating strong diagnostic utility across most studies. Negative likelihood ratios ranged from 0.04 to 0.19, reflecting consistent diagnostic performance in ruling out clavicle fractures (Q = 7.42, df = 6, P = 0.28; I2 = 19.15%, 95% CI: 0%–82.01%) (Figure 4(d)).

Forest plot and summary statistics of the diagnostic test accuracy meta-analysis across all included studies. CI: confidence interval; DLR: diagnostic likelihood ratio.
Diagnostic score (DS) and DOR
Figure 5(a) illustrates the DS, which varied from 3.74 to 6.62, with substantial heterogeneity (Q = 5.33, df = 6, P = 0.50; I2 = 0%, 95% CI: 0%–100%). DOR values ranged widely from 63.00 to 751.33 (Figure 5(b)), reflecting marked differences in diagnostic strength. The pooled DOR showed extreme heterogeneity (Q = 16.8, df = 6, P = 0.01; I2 = 64.44%).

Forest plot and summary statistics of diagnostic score and diagnostic odds ratio in the diagnostic test accuracy meta-analysis. CI: confidence interval.
Likelihood ratio scattergram and Fagan plot
The likelihood ratio scattergram (Figure 6(a)) demonstrated that ultrasound shows good performance in ruling in clavicle fractures but only moderately good performance in ruling them out.
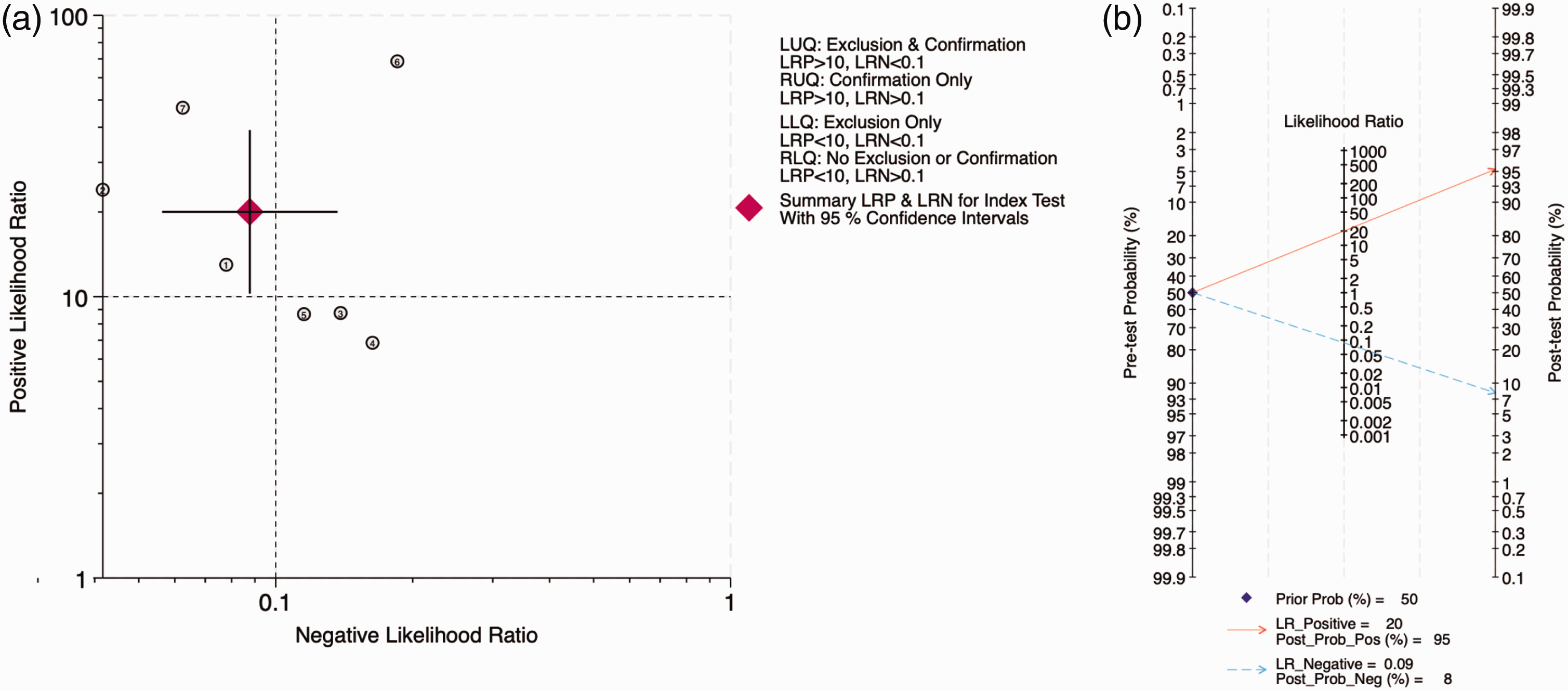
Likelihood ratio scattergram and Fagan plot. (a) Likelihood ratio scattergram of all included studies indicating moderate-to-high test performance suitable for both exclusion and confirmation purposes and (b) Fagan plot analysis using summary sensitivity and specificity results of the meta-analysis of all included studies and a hypothetical pre-test probability of 50%. LRN: likelihood ratio negative; LRP: likelihood ratio positive; LUQ: left upper quadrant; RUQ: right upper quadrant.
Fagan plot analysis (Figure 6(b)) revealed that assuming a pre-test probability of 50%, ultrasound yielded a post-test probability of 95% following a positive result and 8% following a negative result, supporting its clinical utility in decision-making.
Discussion
This meta-analysis suggests that ultrasound is a potentially valuable diagnostic tool for clavicle fractures in emergency settings, with a pooled sensitivity of 0.92 and specificity of 0.95. Sensitivity and specificity demonstrated low heterogeneity, indicating substantial variability in test performance among studies. Despite this, both the Fagan plot and likelihood ratio analysis support the practical clinical utility of ultrasound for confirming or excluding clavicle fractures. The likelihood ratio scattergram further indicated that ultrasound may provide moderate-to-high diagnostic performance, highlighting its applicability as a rapid and noninvasive tool in ED.
Ultrasound imaging is a readily accessible and user-friendly modality, particularly suited for superficial bones such as the clavicle. 7 To the best of our knowledge, the earliest study comparing ultrasound and X-ray for pediatric clavicle fractures was conducted by Blab et al. 26 in 1999, which found no significant statistical differences between the two imaging modalities. Subsequent studies have confirmed these results in children of any age.19,20 Its bedside application facilitates swift diagnosis, making it especially beneficial in emergency and neonatal care. 1 Given the clavicle’s superficial anatomical position, high-frequency linear probes offer high-resolution imaging, enabling comprehensive visualization of bone structures. Enhanced visualization aids in detecting subtle fractures and identifying key diagnostic indicators, particularly cortical bone discontinuities.
Clinically, the diagnostic accuracy observed in this meta-analysis underscores the potential of ultrasound as an effective adjunct to traditional imaging modalities. Our findings are consistent with those of previous meta-analyses demonstrating the high diagnostic performance of ultrasound for clavicle fractures. Hassankhani et al. 2 reported pooled sensitivity and specificity of 0.94 and 0.98, respectively, with particularly strong performance in pediatric populations, albeit with slightly lower specificity compared with that in adults (P = 0.01). Galimberti et al. 1 further confirmed ultrasound’s value in neonates, achieving 100% diagnostic accuracy (135/135), and recommended it as the gold standard due to its safety and real-time capabilities. In a broader context, Popat et al. 14 found that point-of-care ultrasound (POCUS) yielded a sensitivity of 93% and specificity of 94% for clavicle fractures, reinforcing its utility in emergency settings for rapid, radiation-free diagnosis. By enabling early identification or exclusion of clavicle fractures, ultrasound may help optimize imaging strategies, potentially minimizing unnecessary radiation exposure in select patient groups. Together, these findings support the integration of ultrasound into routine clinical workflows, especially in pediatric and resource-limited environments.
The accessibility and radiation-free nature of ultrasound further underscore its suitability in resource-limited settings, particularly in low- and middle-income countries where advanced imaging technologies may be scarce. Unlike X-ray or CT, ultrasound can be repeatedly utilized safely for monitoring fracture healing. 26 Although neonatal clavicle fractures often require minimal intervention, ultrasound monitoring provides reassurance regarding fracture healing, particularly among concerned parents. Compared with adult bones, pediatric bones have greater elasticity, cartilage content, and lower density, enhancing ultrasound penetration and clarity of fracture imaging. 27 Pediatric patients’ smaller clavicle size and lower body mass further facilitate high-resolution imaging, supporting ultrasound’s diagnostic superiority in this population. 28 Consequently, ultrasound offers an optimal combination of safety, accuracy, and practicality for pediatric fracture detection, advocating its routine integration into pediatric and emergency clinical settings.
Despite these promising insights, this meta-analysis had several important limitations. First, the limited number of high-quality studies raises concerns, as several included studies had methodological flaws such as convenience sampling and unclear blinding, which may affect reliability. Second, the observed heterogeneity in specificity likely reflects differences in operator skill and reference standards (X-ray vs. CT). Third, the generalizability of results is constrained by the limited inclusion of older and high-risk populations. Fourth, variability in ultrasound training and diagnostic criteria across institutions may further contribute to inconsistent performance. Furthermore, the lack of standardized ultrasound protocols across studies reduces reproducibility and may contribute to variability in diagnostic outcomes.
Future research should address these limitations and focus on the following priorities: (a) developing standardized scanning protocols to improve consistency across clinical settings; (b) conducting large-scale, prospective, multicenter studies to validate ultrasound’s diagnostic performance across diverse populations; (c) evaluating operator training needs and learning curves to establish minimum competency standards; and (4) investigating the potential of artificial intelligence to assist in ultrasound interpretation, reduce interoperator variability, and enhance diagnostic accuracy in real-time clinical environments.
Conclusion
This meta-analysis highlights ultrasound’s potential role as an adjunct or primary diagnostic tool for clavicle fractures in emergency settings, given its relatively high diagnostic accuracy, radiation-free profile, and point-of-care applicability. Despite variability in operator expertise and reference standards, the findings support ultrasound’s clinical value, especially in pediatric and resource-limited contexts. Further rigorous research is essential to standardize protocols, improve diagnostic consistency, and confirm ultrasound’s role in routine emergency workflows.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251351273 - Supplemental material for Evaluation of the diagnostic performance of ultrasound for clavicle fractures in emergency settings: A meta-analysis and systematic review
Supplemental material, sj-pdf-1-imr-10.1177_03000605251351273 for Evaluation of the diagnostic performance of ultrasound for clavicle fractures in emergency settings: A meta-analysis and systematic review by Bin Lin, Danqin Yuan, Weiting Chen, Ying Liu and Xiaozhen Ji in Journal of International Medical Research
Footnotes
Acknowledgments
This manuscript was polished for language clarity using Grammarly Premium and ChatGPT (OpenAI).
Author contributions
Writing—original draft preparation, Bin Lin; writing—review and editing, Danqin Yuan and Xiaozhen Ji; supervision, Ying Liu and Weiting Chen. All authors have read and agreed to the published version of the manuscript.
Data availability statement
Data are contained within the article.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Funding
This research received no external funding.
Institutional review board statement
Not applicable.
Informed consent statement
Not applicable.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.