
Abstract
Background:
In the early period of spontaneous circulation (ROSC), the body may show severe immunosuppression and excessive activation of inflammatory response, This is very similar to sepsis in many ways.
Objective:
The aim of this study is to observe changes of the early expression of monocyte human leukocyte antigen DR in patients with cardiac arrest, so as to explore the clinical significance of the related immune assessment and prognosis prediction.
Methods:
A total of 43 patients with cardiac arrest who have been treated in the emergency department of Beijing Chaoyang Hospital from January 2015 to February 2018 are selected. By taking the survival rate on the 28th day of hospitalization as the end of observation, the patients are divided into the survival group and the death group. Changes of APACHE-II scores and monocyte human leukocyte antigen DR levels on the first, second, and third day after admission are analyzed.
Results:
On the first, second, and third day after onset, cardiac arrest patients show significantly decreased levels of monocyte human leukocyte antigen DR which are obviously lower in the death group than in the survival group. In addition, human leukocyte antigen DR levels were significantly negatively correlated with APACHE-II scores.
Conclusion:
The expression of monocyte human leukocyte antigen DR is proven to be an ideal indicator to evaluate the immune function and prognosis of cardiac arrest patients. A constantly low expression of human leukocyte antigen DR indicates impaired immune function and increased mortality of patients.
Introduction
Cardiac arrest (CA) is an unnatural pathophysiological state of the body after undergoing complete and systemic ischemia, during which time the body has suffered severe stress reaction. As a result, not only the nerves, endocrines, and vasoactive substances will change but also a large number of cytokines and inflammatory mediators will be produced due to intense pathological stimuli, inducing systemic inflammatory response syndrome. 1 In our recent animal research, it has been found that in the early period of spontaneous circulation (return of spontaneous circulation (ROSC)), the body may show severe immunosuppression and excessive activation of inflammatory response.2,3 This is very similar to sepsis in many ways, for they may both result in elevated levels of cytokines and inflammatory factors. 4
Previous studies have found that CA patients tend to show sepsis-like manifestations, that is, systemic inflammatory response, suppressed immune function, and severe secondary infection, leading to serious multiple organ dysfunction syndrome (MODS). Such post-resuscitation immunosuppression may be closely related to the high mortality rate of CA patients. 5 For this reason, it is of great importance to assess the immune function of CA patients as soon as possible and to provide proper interventional treatment. As a marker of monocyte activation, human leukocyte antigen DR (HLA-DR) is a molecule that initiates a specific immune response in human body. It has been widely used as one of the assessment indicators of immune function in clinical practice. 6 By observing changes of the early expression of monocyte HLA-DR in CA patients, this study intends to explore the clinical significance of the related immune assessment and prognosis prediction.
Materials and methods
Case selection
A total of 43 patients with CA who had been treated in the emergency department of Beijing Chaoyang Hospital from January 2015 to February 2018 were selected, including out-of-hospital cardiac arrest (OHCA) cases sent to the emergency department and in-hospital cardiac arrest (IHCA) cases occurring in the emergency department. The protocol was approved by the Ethics Committee of Beijing Chaoyang Hospital (Permit Number: 2015 S-133). CA criterion was identified in accordance with 2015 International Consensus on Cardiopulmonary Resuscitation (CPR). The following cases are excluded from the research scope: (1) unspecified time of CA, (2) age < 14 years, (3) families refusing to take CPR, and (4) incomplete data. The normal control group consisted of 15 healthy checkup participants in the same period.
Research methods
Resuscitation
According to the 2015 International Consensus on CPR, chest compressions, airway opening, and respiratory support were quickly performed on CA patients. Early defibrillation was carried out when heart rate defibrillation was applicable and intravenous passage ways were established. Epinephrine and advanced life support were provided after resuscitation.
CPR registration
By referring to the Utstein model and epidemiological requirements, a CPR registration form was designed for relevant data registration of CA patients with the initiation of CPR procedure. Contents of registration mainly included patients’ data, CA data, and resuscitation effect. Specifically, patients’ data included age, gender, and condition. CA data included the place, time, etiological agent and witnesses of CA, the starting point and duration of CPR, and the initially monitored heart rate. Resuscitation effect (end of observation) included the ROSC and the 24-h and 28-day survival and death rates.
Experimental procedures
All subjects’ vital signs, such as body temperature, respiration, heart rate, and blood pressure on the first, second, and third days after admission, were recorded. Routine examinations such as blood routine tests, biochemical tests, needed image logical examination, and culture of body fluid specimens were performed. APACHE-II (acute physiology and chronic health evaluation) scores were calculated on all included patients. Serum samples were collected on the first, second, and third days, and patients’ CD14 + monocyte HLA-DR was monitored.
Detection method
Flow cytometry (Beckman Coulter, Pasadena, CA, USA) was used to detect the monocyte HLA-DR of CA patients. Gallios version 1.0 was used as the software for flow analysis (Beckman Coulter). All antibodies were purchased from BD Bioscience (San Jose, CA,USA). 100 µL of anticoagulant was put into the tube with the addition of fluorescein isothiocyanate (FITC) conjugated mouse anti-human HLA-DR monoclonal antibody. The tube was then stored at room temperature in the dark for 20 min. After the antibody reaction was completed, the test tube was taken out and added with 2 mL of 1× hemolysin before swirling Then, the tube was kept at room temperature in the dark for 8 min. After that, it was centrifuged at 300g for 5 min at a room temperature of 20°C. After centrifugation, the tube was taken out and the supernatant was poured out vertically before swirling. A solution of 2 mL of phosphate-buffered saline (PBS) was added to the tube with swirling and centrifugation again at 300g for 5 min at a room temperature of 20°c. The sample tube was added with 0.5 mL of PBS, fully swirled and mixed, and then detected with the flow cytometry within an hour.
Statistical processing
In this study, SPSS 20.0 was used for statistical analysis. All quantitative data in line with normal distribution was denoted as x ± s. Independent sample t-test was applied to two different groups. Paired sample t-test was conducted for inter-group changes before and after a time point. Pearson’s correlation analysis was used to analyze the correlation between two variables. p < 0.05 was considered statistically significant.
Results
Clinical and demographic characteristics
A total of 55 patients with CA were treated. According to inclusion and exclusion criteria, 43 cases were included in this study. Of the 43 patients in this study, 28 cases and 15 cases occurred in the OHCA and IHCA, respectively. A total of 39 deaths occurred, 23 died of cardiovascular or organ failure and 16 died of neurological dysfunction with treatment withdrawal. Before the arrival of the ambulance, only four patients with OHCA received bystander CPR, and one of them was lucky to finally survive. In the study, 11 patients received mild hypothermia treatment, all patients in the survival group were treated with mild hypothermia, and 3 patients received cardiac revascularization (as shown in Table 1).
Patient characteristics.
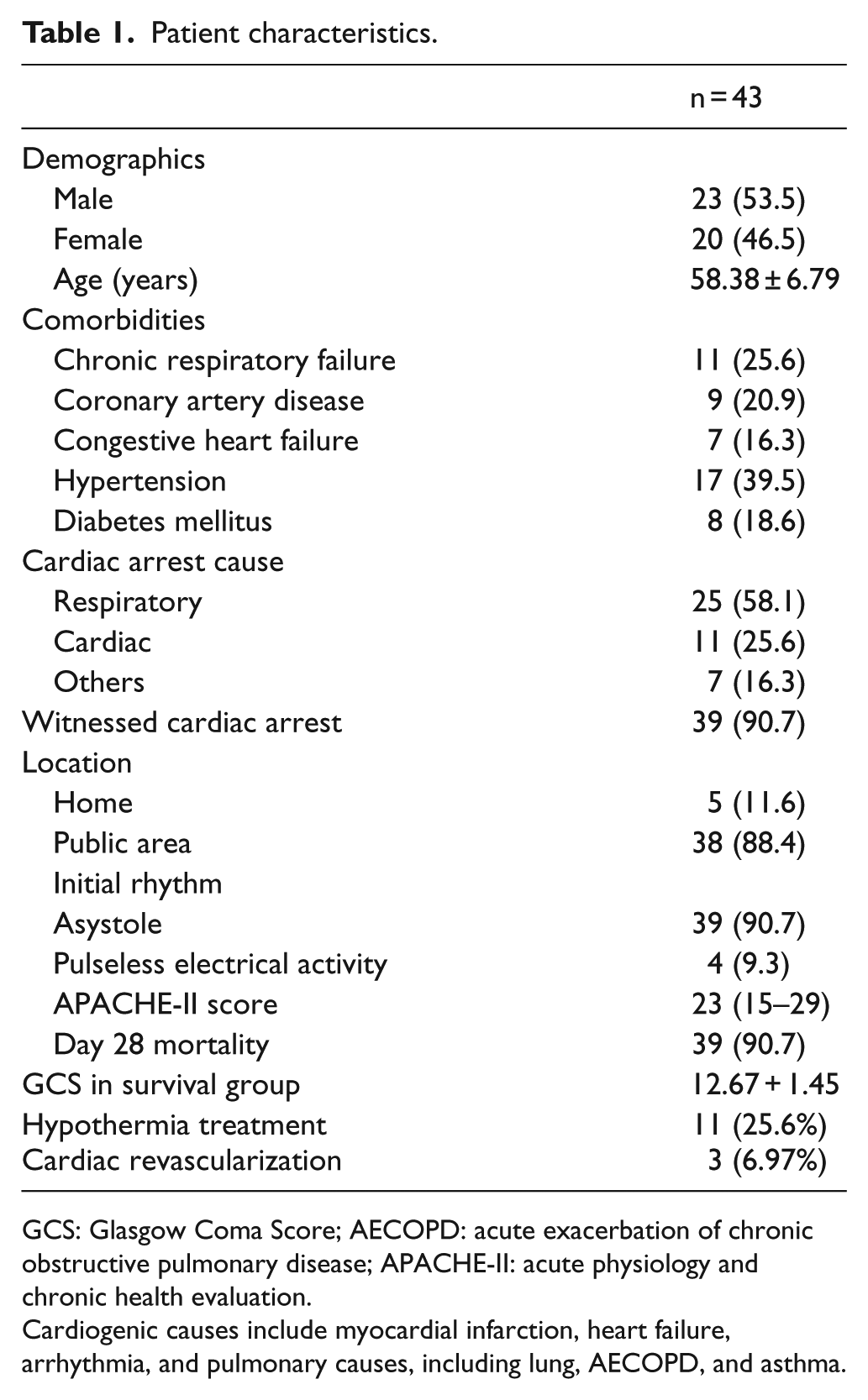
GCS: Glasgow Coma Score; AECOPD: acute exacerbation of chronic obstructive pulmonary disease; APACHE-II: acute physiology and chronic health evaluation.
Cardiogenic causes include myocardial infarction, heart failure, arrhythmia, and pulmonary causes, including lung, AECOPD, and asthma.
The high severity of this cohort is illustrated by the elevated values of APACHE-II scores and the high mortality (91%; n = 4 survivors) (as shown in Table 2).
Correlation comparison of HLA-DR levels and APACHE-II scores between the survival group and the death group on the first, second, and third days after onset.
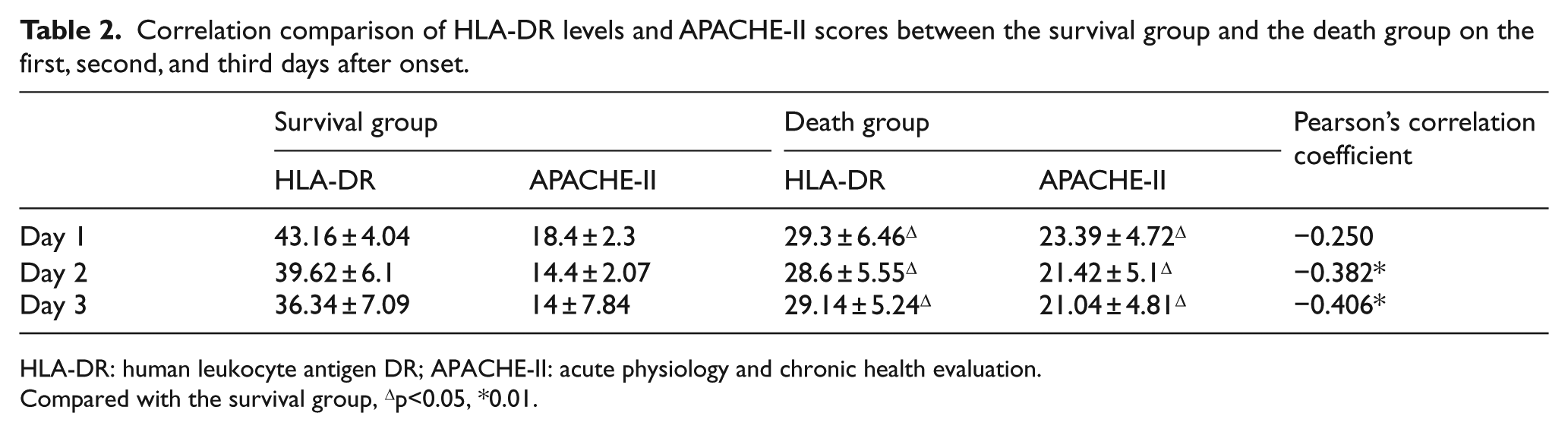
HLA-DR: human leukocyte antigen DR; APACHE-II: acute physiology and chronic health evaluation.
Compared with the survival group, Δp<0.05, *0.01.
Compared with the normal control group, patients in the resuscitation group showed a significant decrease in their monocyte HLA-DR levels on the first, second, and third days after onset (30.91 ± 1.17, 30.05 ± 1.09, 30.23 ± 1.05 vs 55.25 ± 1.19; p < 0.01) (as shown in Figure 1). In addition, on the first, second, and third days after onset, HLA-DR levels of the death group decreased more significantly than that of the survival group (29.30 ± 6.46 vs 43.16 ± 4.04, 28.60 ± 5.55 vs 39.62 ± 6.10, and 29.14 ± 5.24 vs 36.34 ± 7.09; p < 0.01) (as shown in Figure 2).
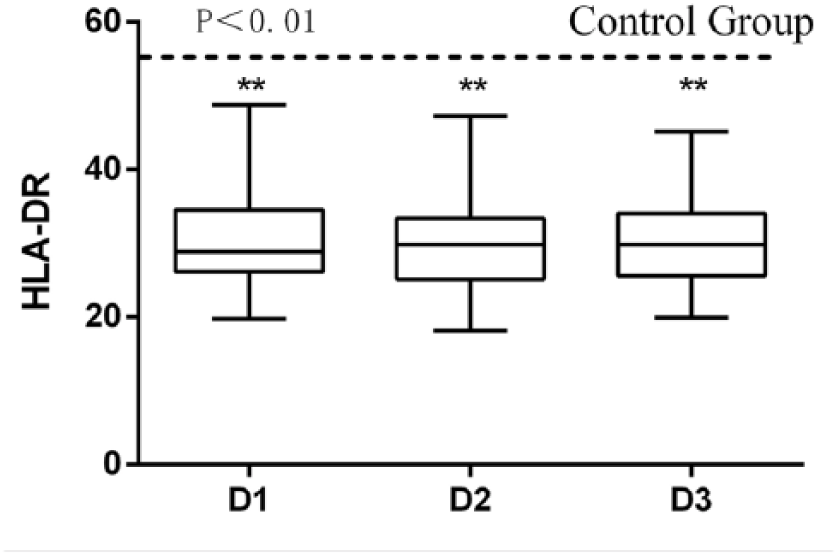
Monocyte HLA-DR expression in 43 patients with cardiac arrest.

Monocyte HLA-DR expression was presented in non-survivors and in survivors according to 28-day mortality.
Results showed that similar to HLA-DR levels, APACHE-II scores of the death group also increased more significantly than that of the survival group on the first, second, and third days after onset (23.39 ± 4.72 vs 18.40 ± 2.31, 21.42 ± 5.10 vs 14.4 ± 2.07, and 21.04 ± 4.81 vs 14.00 ± 7.84; p < 0.01) (as shown in Figure 3). Moreover, except that the correlation coefficient between HLA-DR and APACHE-II on the first day (r = –0.250; p = 0.106 > 0.05) was not statistically significant, the correlation coefficients between the two groups were r = –0.382 (p = 0.018 < 0.05) and r = –0.406 on the second and third days, respectively (p = 0.019 < 0.05), suggesting that there is statistical significance. It indicated that HLA-DR and APACHE-II were obviously negatively correlated on the second and third days, that is, the lower the HLA-DR levels, the higher the APACHE-II scores (as shown in Table 2).
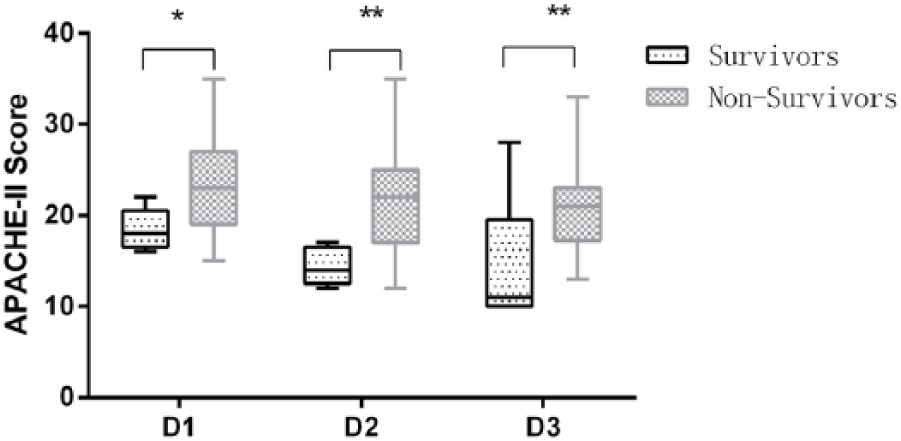
APACHE-II scores were presented in non-survivors and in survivors according to 28-day mortality.
Discussion
In the early period after ROSC, the body has undergone a process of ischemia-reperfusion, and the reperfusion injury in organs of the whole body may produce a large number of inflammatory mediators such as oxygen-free radicals, lactic acid, and metabolites of arachidonic acid which will be released into the blood, resulting in systemic inflammatory responses and suppressed immune function manifested by a decrease in the number and function of T lymphocytes. 7 This is quite similar to sepsis in many ways, suggesting that immunosuppression after CA may inherently be linked to that of sepsis. These mechanisms may be one of the causes of concurrent severe infection after ROSC as well as one of the possible mechanisms to elevate the mortality of CA patients.
HLA-DR is the antigen expressed on the surface of monocytes. Its function is to deliver the antigens phagocytized and processed by mononuclear phagocytes to T helper cells, so that all immune cells, including T cells, B cells, and phagocytic cells can be activated. Therefore, sufficient expression of HLA-DR is essential for both specific and non-specific immune systems. 8 Upon the invasion of pathogenic microorganisms, effective antigen components will be delivered to T lymphocytes with the help of HLA-DR, monocytes, and macrophages, thereby activating the latter and initiating specific immune response. The expression rate of HLA-DR is closely related to the severity of infections and diseases, and thus it can be used as an immune indicator for the assessment of the severity and prognosis of acute and severe diseases. When the expression of HLA-DR is low, the body will be susceptible to serious infections, leading to poor prognosis.9–11 Compared with the high expression of peripheral blood monocyte HLA-DR in normal situation, the expression level tends to decline significantly in case of severe trauma, burns, or major surgery, and it is closely associated with secondary infections and poor prognosis.12–14
When the microorganism invades the host and leads to sepsis, monocytes will play a key role in immune response. The expression of HLA-DR is crucial in the process of presenting antigen and helping T lymphocytes. Excessively low levels of HLA-DR in the body may cause a decline in immune function. For instance, when the expression of HLA-DR is lower than 30%, the immune function of monocytes can even be paralyzed.15,16 However, APACHE-II scores reflect the state of the environment in vivo and functions of vital organs. It can directly and accurately embody the severity of patients’ condition. Closely related to the mortality of patients, it can be used to evaluate the severity and prognosis of critically ill patients. 17 CA patients in this experiment showed a decrease in HLA-DR levels and an increase in APACHE-II scores in the early period after resuscitation. In addition, HLA-DR levels of the death group decreased more significantly than that of the survival group. The decrease in HLA-DR levels was significantly negatively correlated with the increase in APACHE-II scores, yet they were both closely associated with poor prognosis. A too low expression of monocyte HLA-DR will bring disorder to antigen presentation, making the body unable to produce effective immune response, thus resulting in immunosuppression. If the body shows the complication of serious infection caused by bacteria such as gram-negative bacteria, lipopolysaccharide (LPS) release and intestinal LPS translocation will inevitably take place. Via the integration with the receptor CD14 on the mononuclear macrophage membrane, LPS can combine with the Toll-like receptor 4 (TLR-4), transmitting signals into the cells. As a result, the cells will be activated and various inflammatory mediators will be released, causing a decrease in HLA-DR levels and leading to uncontrolled inflammatory responses in the body. Therefore, serious organ infections are further complicated along with MODS,18,19 which greatly increases the mortality of patients after resuscitation.
In summary, the expression of peripheral blood monocyte HLA-DR in CA patients is an effective indicator to assess the immune function of CA patients. Continuously low expression of HLA-DR may suggest impaired immune function and high probability of secondary infections. Detecting the expression of HLA-DR in CA patients can help to determine the immune status of the body and identify the immunosuppression and sepsis after CA in the early time. Proper anti-infection and immune intervention will be conducive to improving the prognosis of CA patients.
Footnotes
Acknowledgements
The authors thank Dr Jiang Zhang and Haijiang Zhou for their technical assistance and Dr Qian Zhang for the advice in data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Natural Science Foundation (no. 7182055) and Beijing Municipal Administration of Hospitals Incubating Program (no. Px2016022).
Ethical approval
The protocol was approved by the medical ethics committee of Beijing Chaoyang Hospital (Permit Number: 2015-8-19-1).
Informed consent
This study was not a clinical study that involves clinical intervention. The authors only retrospectively reviewed with data collected in the surveillance system.