
Abstract
Background:
The world population is experiencing ageing and this phenomenon certainly gives significant impact to the social, economic as well as health care services globally.
Objectives:
This study aimed to determine the prevalence of geriatric patients treated in critical zone in an emergency department of a teaching hospital and the factors associated with special care units admission and in-hospital mortality.
Methods:
A single-centre prospective cross-sectional study was carried out from 1 January 2016 to 31 December 2016 at the Emergency Department Hospital at Universiti Sains Malaysia, Malaysia. All patients aged 60 years and above were included. Systematic random sampling was used. Variables were analysed using simple and multiple logistic regressions.
Results:
The total number of patients included in this study was 328, 55.8% were male and the mean age was 70.6 (standard deviation: 7.5) years. The commonly presenting diseases in this study were cardiovascular (31.4%), infectious (29.6%), neurological (14.9%) and respiratory (12.5%). Out of the 328 patients studied, 187 (57.0%) were admitted to general wards and 110 (33.5%) to special care units. A total of 55 patients (16.8%) succumbed within the period of in-hospital treatment. The factors associated with special care units admission were the usage of non-invasive ventilation and the administration of inotropic support. The factors associated with in-hospital mortality were blood urea level, serum albumin level and the application of mechanical ventilation.
Conclusion:
Geriatric patients who presented to emergency department requiring ventilator and inotropic support had been observed to exhibit worse outcome. The associated factors for special care units admission and in-hospital mortality had been identified, and this will enable better settings cater to the needs for critically ill geriatric patients.
Introduction
The human population is ageing and this phenomenon is common throughout the world. The definition of old age or elderly differs in different countries. In Malaysia, the Ministry of Health defined elderly persons as those who are 60 years or older, 1 which is similar to the definition recommended by World Health Organization (WHO).
The proportion of the global elderly population was 9.2% in 1990 and has increased to 11.7% in 2013. The proportion is expected to grow continuously reaching 21.1% by 2050. The number of older persons is anticipated to markedly increase, from 841 million people in 2013 to more than 2 billion in 2050. 2 The ageing society is expected to be accompanied by problems unique to elderly population. This brings new burden to the health care and social services in the country.
In general, Malaysia has quite comprehensive medical and health care services for the general population. Apart from acute conditions, elderly patients often present with chronic diseases and disability which require long-term care. The current health care system is inadequate in providing special and comprehensive services to elderly patients. 3 With increasing demand on health care service among the elderly population, it is important that the health care and social care systems adapt to the situation and aim at promoting health while providing treatment focusing on health care of the elderly population.
The emergency department plays a central role as an advocacy between inpatient and outpatient care within the health care system. This unique position gives important implication in the treatment of the elderly population, apart from serving as a platform for subsequent care to be provided. In the United States, the geriatric emergency department patients represented 43% of hospital admission. 4 As the elderly population increases, the subsequent need for health care in geriatric emergency service also increases. This is evidenced by the larger and ever increasing proportion of geriatric emergency department visits. Thus, there are many challenges faced by emergency health care providers to ensure effective and reliable care delivery in order to improve the outcomes of geriatric patients.
This study aimed to determine the proportion and predictive factors for special care units (intensive care unit (ICU)/high dependency unit (HDU)/cardiac care unit (CCU)) admission and in-hospital mortality among geriatric patients presented to the critical zone of Emergency Department, Hospital Universiti Sains Malaysia.
Methodology
This was a single-centre prospective study, carried out from 1 January 2016 till 31 December 2016, at the Emergency Department, Hospital Universiti Sains Malaysia, Malaysia. All patients aged 60 years and above who were treated in the critical zone of the Emergency Department of Hospital Universiti Sains Malaysia were selected for the study. Critical zone or red zone (three-tier triage category) is the area within the emergency department where severely ill patients and patients with acute condition threatening the airway, breathing, circulation and neurological system receive immediate resuscitation and treatment. Patients presented with injuries caused by external physical force or trauma were excluded from this study. Using Epi Info 7 calculation software (confidence limits of 5%, design effect of 1.0, clusters of 1, confidence level of 95%), the sample size for this study was 461 patients. The patients were recruited based on a computer-generated simple randomization list. The patients were followed up during the period of treatment and stay in hospital. Medical records were reviewed for outcome upon discharge.
Demographic data such as age, gender and race were recorded. Clinical data such as patients’ demographics, comorbidity (diabetes mellitus, hypertension, ischemic heart disease, congestive cardiac failure, chronic obstructive pulmonary disease, history of cerebral vascular accident, chronic kidney disease, anaemia, malignancy), vital signs (Glasgow Coma Scale, mean arterial pressure, quick sepsis-related organ failure assessment (qSOFA) scoring) upon arrival to emergency department, laboratory investigation parameters (blood urea, serum creatinine, platelet, total bilirubin, serum albumin, serum lactate, blood pH, serum bicarbonate level, PaO2/FiO2 ratio) from the first blood sample taken in emergency department as well as treatment (non-invasive ventilation (NIV), endotracheal intubation with mechanical ventilation, inotropic support, cardiopulmonary resuscitation) received in the emergency department were also obtained for the analysis of factors associated with special care units admission and in-hospital mortality.
The study was approved by the Human Research Ethics Committee of Universiti Sains Malaysia (USM/JEPeM/15110480). Permission from the Director of Hospital Universiti Sains Malaysia was obtained to review the medical records. All data were managed and analysed by IBM SPSS Statistics for Windows, version 22.0 (released in 2013; IBM Corp., Armonk, NY). Descriptive statistics were expressed as frequency and percentage for categorical variables and mean and standard deviation (SD) for numerical variables. Multiple logistic regression was used to examine the association between demographic and clinical factors with special care units admission and in-hospital mortality. A p value of <0.05 was considered as statistically significant for all statistical analyses in this study and will be applied to determine the associated factors of mortality in hospitalized geriatric patients (Figure 1).
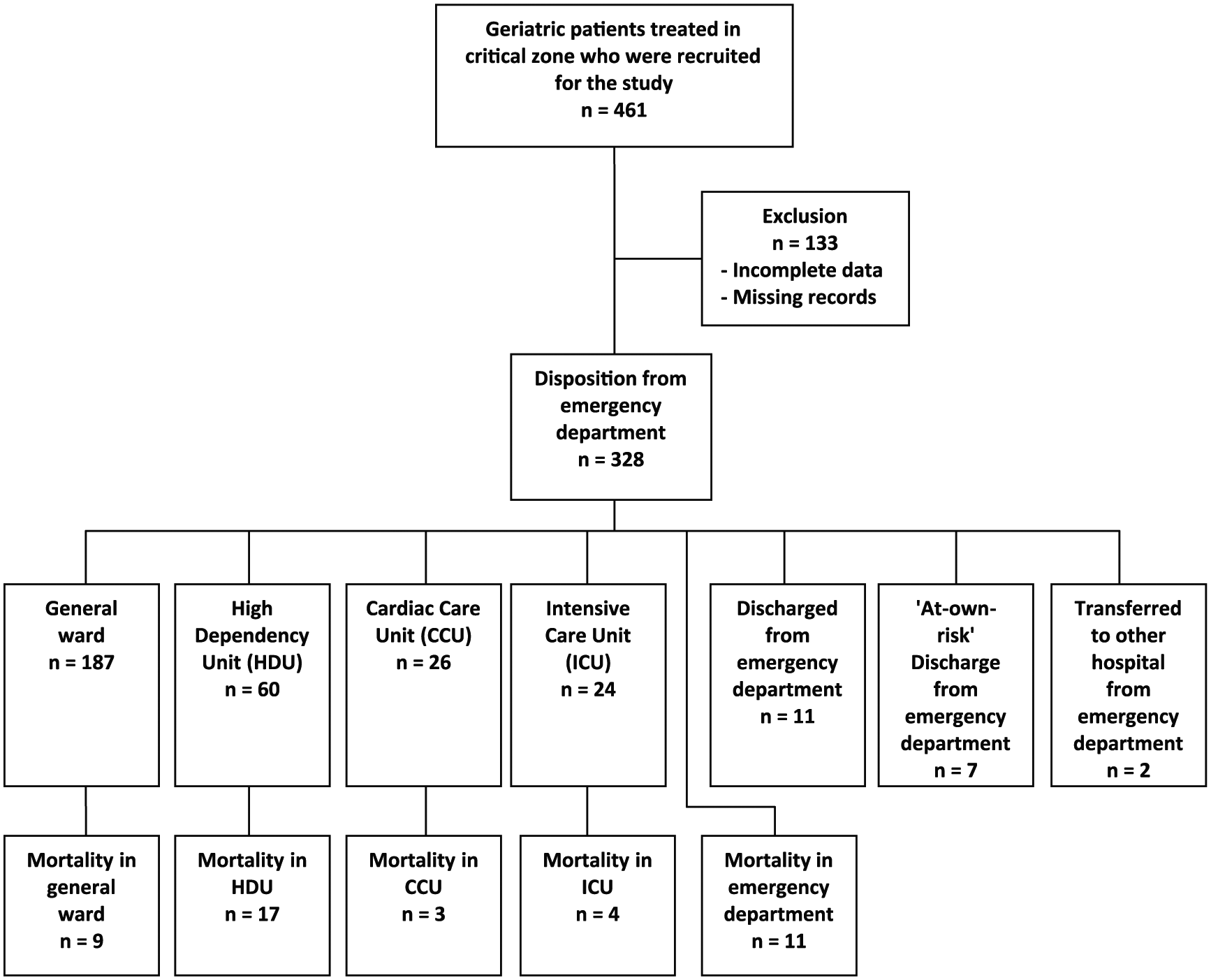
Flowchart of the study.
Results
A total of 461 patients were recruited in this study. However, 133 samples were excluded from the study due to incomplete data. Only 328 patients were included in this study. Out of these 328 patients, 55.8% were male; their age ranged from 60 to 108 years (mean: 70.6, SD: 7.5); 88 patients (26.8%) were 75 years and older (Table 1). The ethnicity of the patients showed that 91.2% of the patients were Malay, 7% were Chinese, 1.2% were Siamese and 0.6% were of other ethnicity.
Demographic characteristics of the entire study group (n = 328).
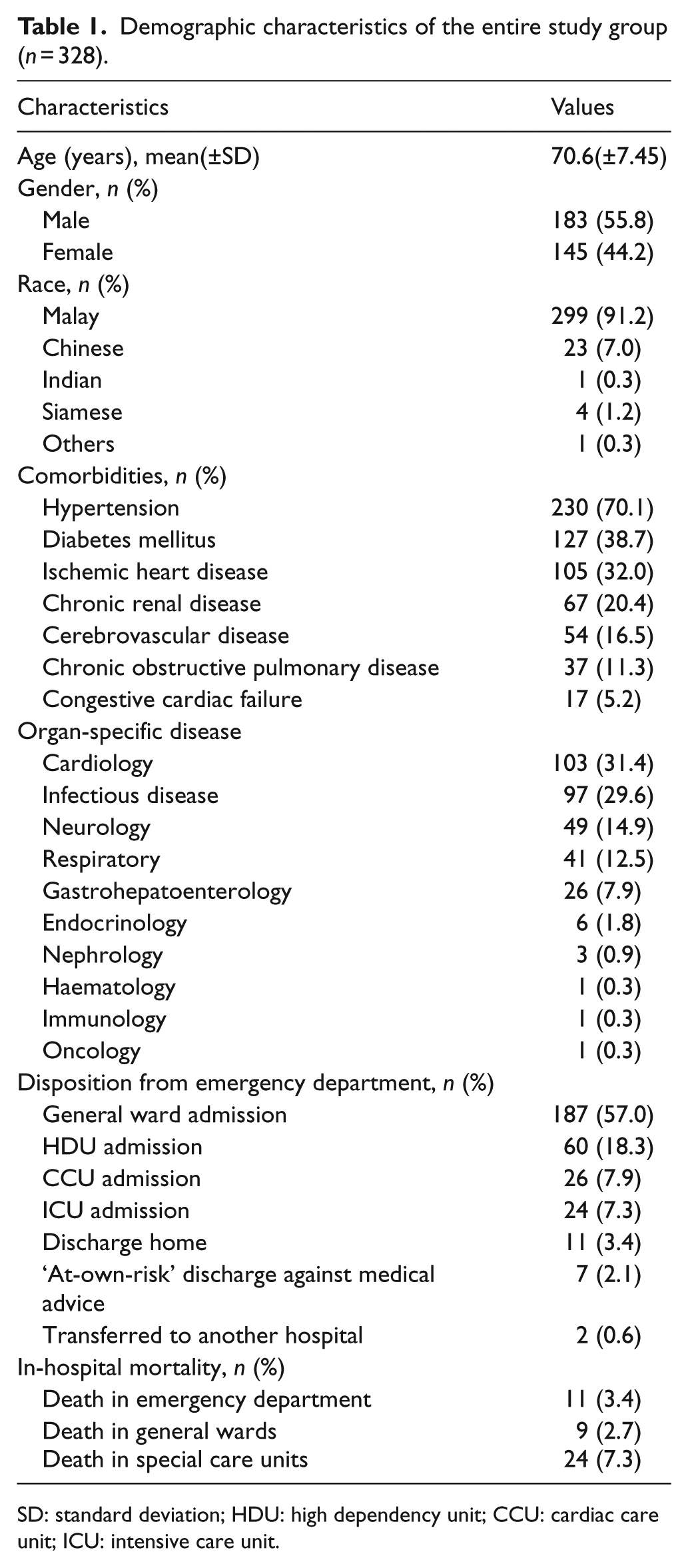
SD: standard deviation; HDU: high dependency unit; CCU: cardiac care unit; ICU: intensive care unit.
The common comorbidities among the patients were hypertension (70.1%), diabetes mellitus (38.7%), ischemic heart disease (32.0%), chronic renal disease (20.4%), cerebrovascular disease (16.5%), chronic obstructive pulmonary disease (11.3%) and congestive cardiac failure (5.2%). The common presentations were associated with cardiovascular (31.4%), infectious (29.6%), neurological (14.9%) and respiratory (12.5%) diseases. A total of 187 patients (57.0%) were admitted to general wards, 112 (34.1%) to special care units, 24 (7.3%) to ICU, 26 (7.9%) to CCU and 60 (18.3%) to HDU. In total, 44 patients (13.4%) succumbed to their illnesses within the period of in-hospital treatment. Among them, 11 patients (3.4%) died in the emergency department. Two patients (0.6%) were transferred to another hospital, 11 (3.4%) were discharged home and 7 (2.1%) requested ‘at-own-risk’ discharge against medical advice from the emergency department.
The factors associated with special care units admission were the usage of NIV (p = 0.004) and the usage of inotropic support (p < 0.001) (Tables 2 and 3). On the other hand, the factors associated with in-hospital mortality were blood urea level (p = 0.018), serum albumin level (p = 0.015) and the application of mechanical ventilation (p < 0.001) (Tables 4 and 5).
Associated factors of predictors with special care units admission by multiple logistic regression.
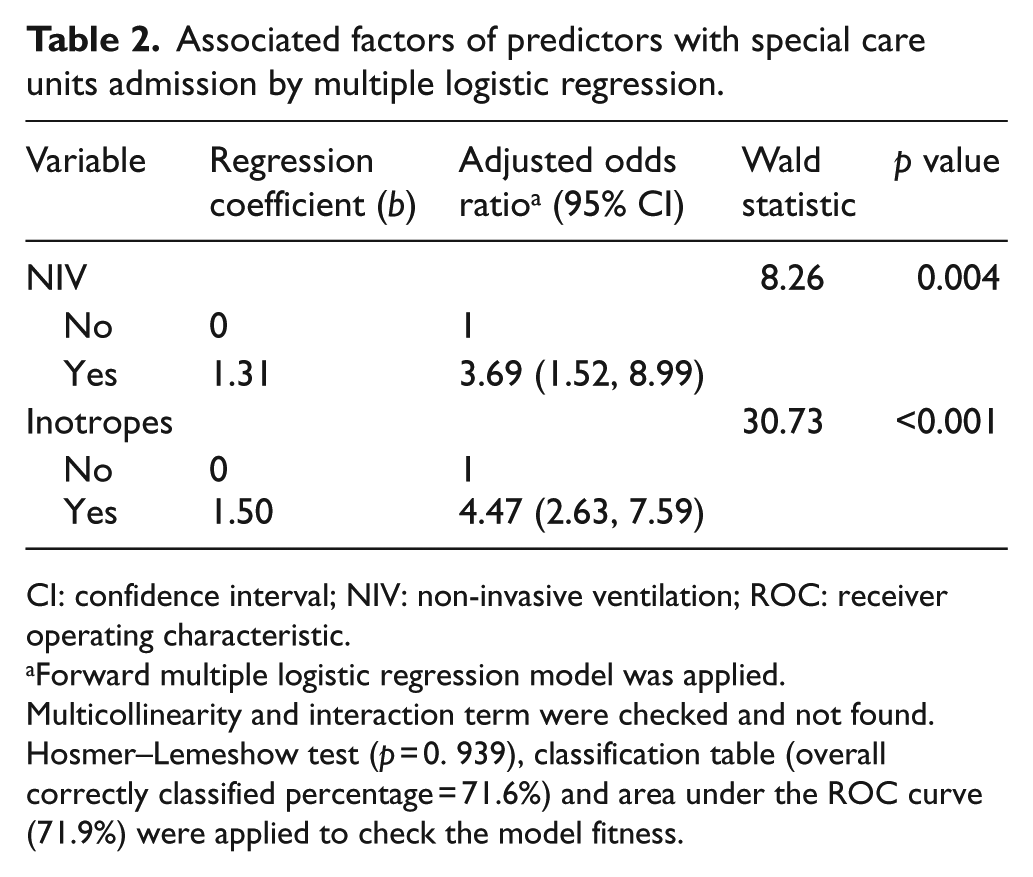
CI: confidence interval; NIV: non-invasive ventilation; ROC: receiver operating characteristic.
Forward multiple logistic regression model was applied.
Multicollinearity and interaction term were checked and not found.
Hosmer–Lemeshow test (p = 0. 939), classification table (overall correctly classified percentage = 71.6%) and area under the ROC curve (71.9%) were applied to check the model fitness.
Associated factors of predictors with special care units admission by simple and multiple logistic regression.
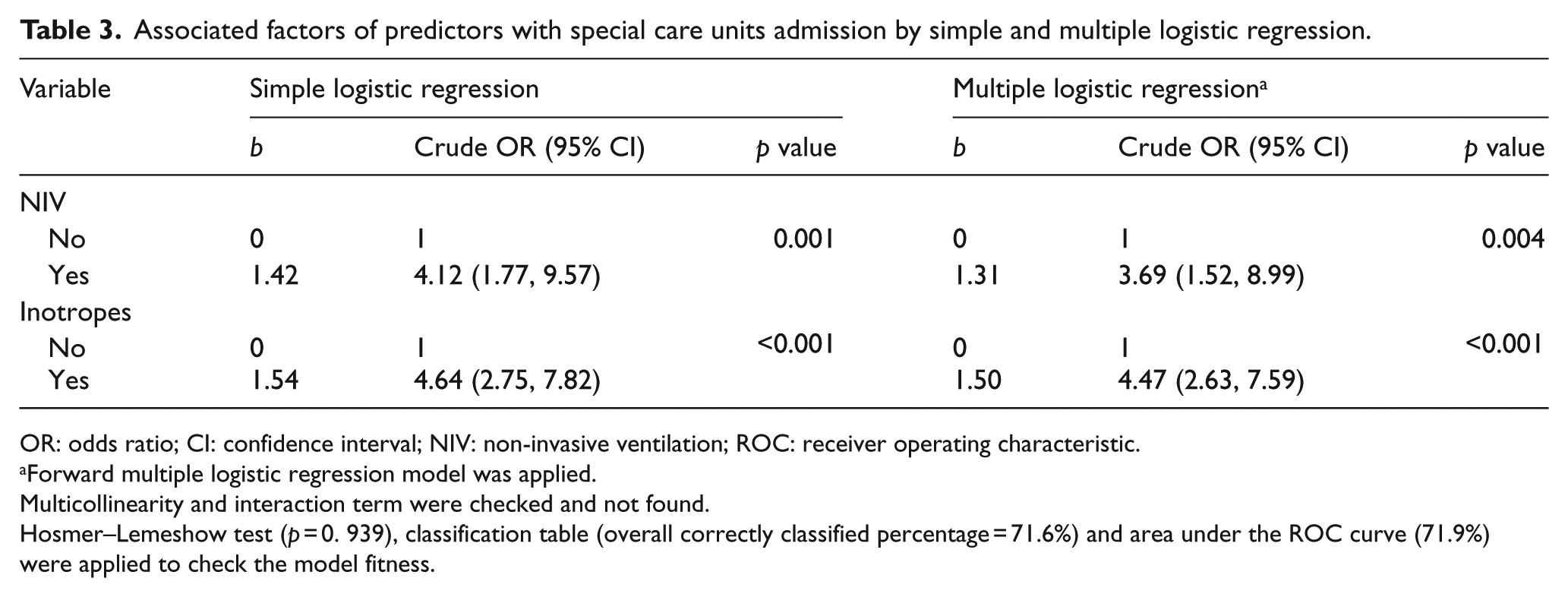
OR: odds ratio; CI: confidence interval; NIV: non-invasive ventilation; ROC: receiver operating characteristic.
Forward multiple logistic regression model was applied.
Multicollinearity and interaction term were checked and not found.
Hosmer–Lemeshow test (p = 0. 939), classification table (overall correctly classified percentage = 71.6%) and area under the ROC curve (71.9%) were applied to check the model fitness.
Associated factors of predictors with in-hospital mortality by multiple logistic regression.
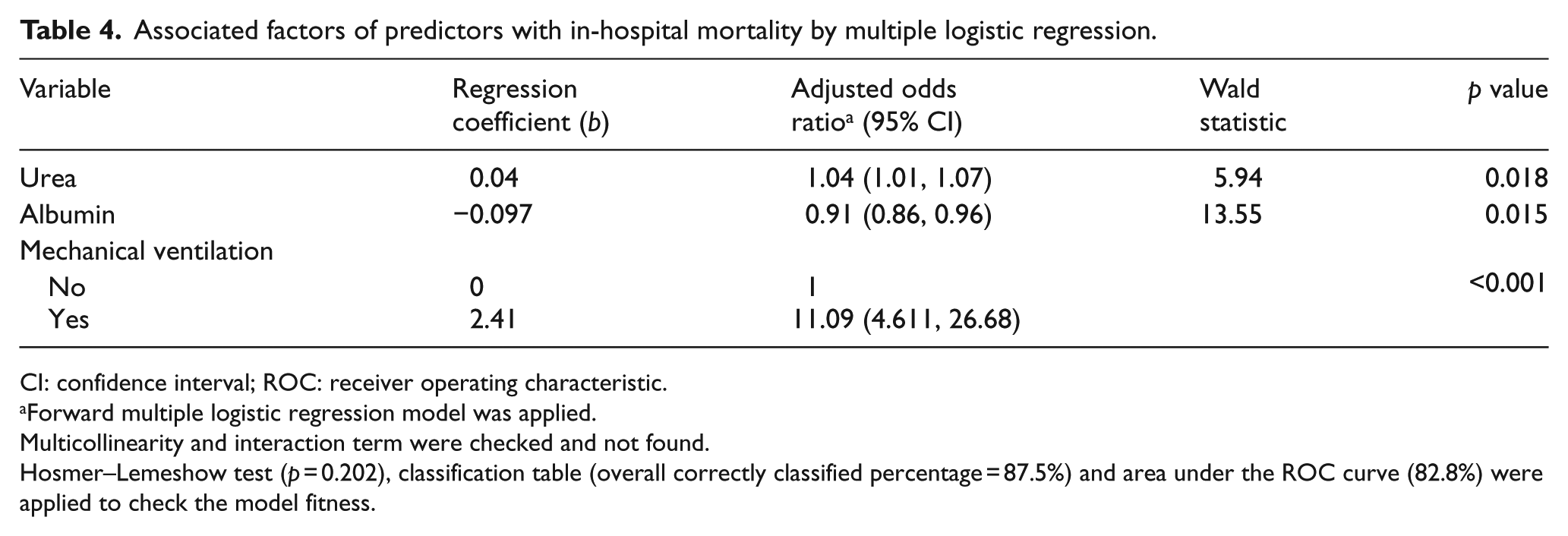
CI: confidence interval; ROC: receiver operating characteristic.
Forward multiple logistic regression model was applied.
Multicollinearity and interaction term were checked and not found.
Hosmer–Lemeshow test (p = 0.202), classification table (overall correctly classified percentage = 87.5%) and area under the ROC curve (82.8%) were applied to check the model fitness.
Associated factors of predictors with in-hospital mortality by simple and multiple logistic regression.
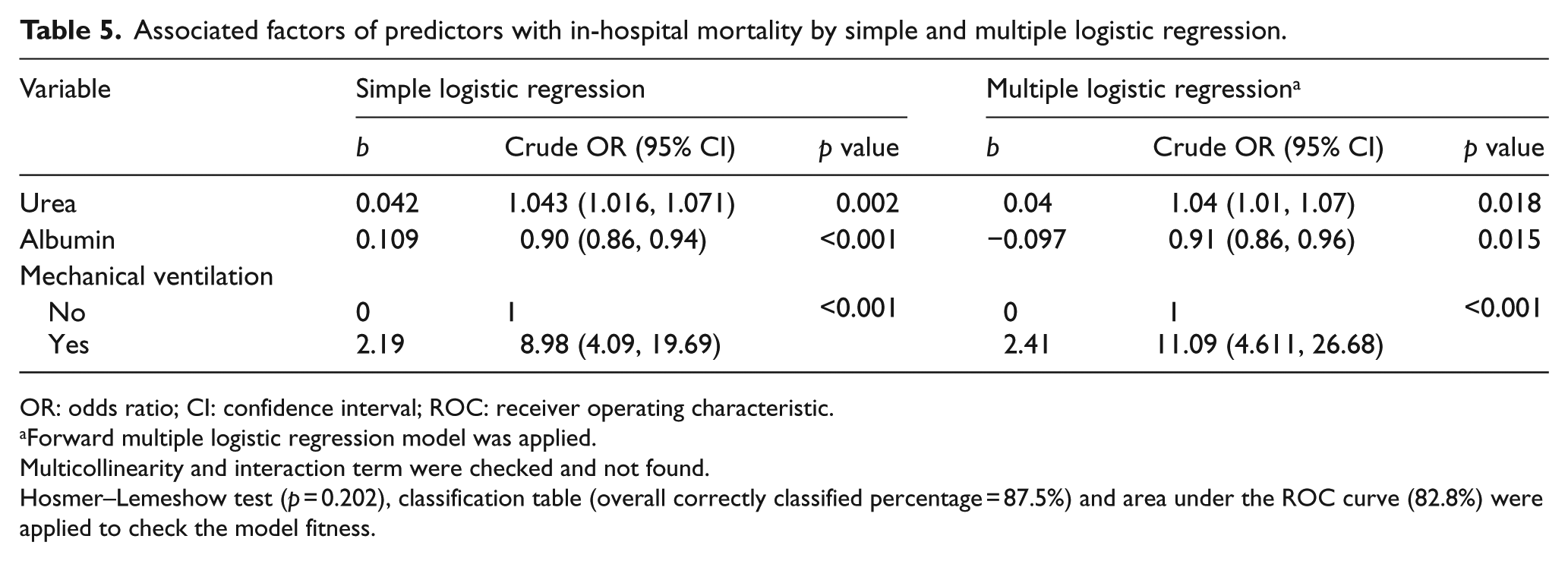
OR: odds ratio; CI: confidence interval; ROC: receiver operating characteristic.
Forward multiple logistic regression model was applied.
Multicollinearity and interaction term were checked and not found.
Hosmer–Lemeshow test (p = 0.202), classification table (overall correctly classified percentage = 87.5%) and area under the ROC curve (82.8%) were applied to check the model fitness.
Discussion
The mean age of geriatric patients in this study was 70.6 years, with age ranging from 60 to 108 years. Previous reports found the mean age of geriatrics to be 72.8 years and higher, as those reports defined elderly as 65 years and older rather than 60 years in this study. 5 Among the comorbidities, the prevalence of hypertension (70.1%) in this study correlated with the rising prevalence globally at 60%.6,7 The high prevalence of non-communicable diseases was also seen globally with its consequence being the increased burden of these diseases.8–10
This study has reported infectious disease at 29.6% and respiratory disease at 12.5% among geriatric patients which was comparable to a study in medical ICU setting in Singapore. According to Mukhopadhyay et al.’s 11 study, infectious disease was reported at 30.1% and respiratory disease at 16.2%; however, cardiovascular and neurological diseases were reported to be lower than the proportion in this study. The difference was probably due to the inclusion of CCU and neurology ICU in this study. In a different study regarding the outcome of geriatric patient in emergency department in Turkey, cardiology and neurology ward admissions were found to be more common at 7.3% and 6.7%, respectively, when comparing to other subspecialty ward admission. 5
With regard to patient’s disposition from the emergency department, about one-third of geriatric patients were admitted to special care units from the critical zone of emergency department. Besides the fact that a total of 44 patients (13.4%) died within the period of in-hospital treatment, among them 11 patients (3.4%) died in the emergency department. This reflected that geriatric population often presented to the emergency department with more critical condition and special attention was needed during the treatment and care for the geriatric patients.
The factors associated with special care units admission were the usage of NIV (p = 0.004) and the usage of inotropic support (p < 0.001). It was found that patients who had NIV usage were at 3.69 higher odds for special care units admission compared to those without NIV usage (95% confidence interval (CI): (1.48, 9.20), p = 0.005) when adjusted for other variables, while patients who were on inotropic support during treatment in emergency department were at 3.89 higher odds compared to those without when adjusted for other variables. It is not surprising that the patients treated with NIV and inotropic support were admitted to special care units. Although NIV and inotropic support were not available in general wards, certain patients that improved after initial treatment could be taken off from NIV and inotropic support and would be admitted to general wards. For those who were dependent on NIV and/or inotropic support along with the stay in emergency department, special care and attention was essential during the treatment for these critically ill patients despite the fact that the usage of NIV and inotropic support was not associated with in-hospital mortality in this study. However, there were no available data in the literature correlating NIV and inotrope usage with special care units admission. In a different study, both NIV (95% CI: 0.40 (0.28–0.56), p < 0.001) and vasopressor (95% CI: 2.56 (2.00–3.26), p < 0.001) were found to be independent predictors of in-hospital mortality for geriatric patients in ICU. 11 These findings differ from those of this study, which may be due to several variabilities such as the treatment setting (emergency department versus ICU) and the preference of inotropic support and dosage between the institutions in both studies.
On the other hand, the factors associated with in-hospital mortality were blood urea nitrogen (BUN) level (p = 0.018), serum albumin level (p = 0.015) and the application of mechanical ventilation (p < 0.001). After being adjusted for other variables, it was found that an increase of 1 mmol/L in blood urea level was associated with 1.04 higher odds for mortality (95% CI: (1.02, 1.08), p < 0.001). This is supported by previous studies that showed BUN as a significant predictor of all-cause mortality.12–16 Besides the fact that an increase in protein intake increases urea excretion, high ammonia source from urea hydrolysis (CO2 + ammonia) in the colon and amino acid catabolism during protein breakdown provide substrates in hepatocytes for ureagenesis. In the critically ill patients, BUN rises with such condition as malnutrition and starvation, hypovolaemia and renal hypoperfusion from dehydration, gastrointestinal bleeding, reduced cardiac output and sepsis. Glucocorticoids increase amino acid utilization in ureagenesis, while metabolic acidosis increases BUN by increased catabolism of protein and decreased protein synthesis. 12 Increased BUN level is also demonstrated in cases of decompensated heart failure but not in stable patients with milder degree of heart failure, probably representing renal response to systemic hypoperfusion.13,16 High BUN is also associated with an increased risk of blood culture positivity prior to and after ICU admission. 12 It may be explained by the fact that high BUN as an index of catabolic state decreases the immunocompetence of the patients. This reflects a higher risk for severe infections and severity of critical illnesses.
Few studies had found that serum albumin level decreased with age and hypoalbuminaemia was associated with longer hospital stay, more likely for readmissions, and increased risk of in-hospital mortality.17–21 In this study, we found that with a 1 g/L increase in Alb there were 7% lower odds for mortality (95% CI: (1.02, 1.08), p < 0.001). Like BUN level, albumin may be a marker of inflammation and the severity of the underlying disease. It is a negative acute phase protein, and when the albumin level is low, it is associated with the increased serum levels of C-reactive protein, cytokines and other positive acute phase proteins in haemodialysis patients. 20 Besides maintaining colloid osmotic pressure, albumin is involved in binding and transport of free fatty acids, calcium, certain hormones and a number of drugs and toxins. With the thiols in its sulphhydryl groups, albumin scavenges free oxygen and nitrogen radicals. Albumin also plays a role in anticoagulant and antithrombotic effects by binding nitric oxide free radicals. Hypoalbminaemia leads to increased concentration of free lysophosphatidylcholine, hence affecting endothelial cell function, altering erythrocyte structure and blood viscosity, as well as inhibiting nitric oxide–mediated vascular relaxation. As a result, platelet dysfunction, antithrombotic effects and alteration of vascular permeability occur. Despite the anticoagulant and antithrombotic effects of hypoalbminaemia, the Framingham Offspring Study suggests that hypoalbuminaemia may be a risk factor for myocardial infarction, possibly playing an indirect role indicating an underlying chronic condition. 21 Malnutrition, inflammatory states, liver diseases, renal diseases and many conditions may demonstrate hypoalbminaemia and are likely to have decreased immune function and thus increased risk of infection and sepsis. 17 Despite the important functions of albumin, analbuminaemia in humans is found incidentally without presenting as a disease. Thus, it is rather the illnesses that cause hypoalbuminaemia that are associated with morbidity than the effect of hypoalbuminaemia per se, 20 making it a proxy of mortality in critically ill patients.
The patients who were on mechanical ventilation had shown 11.39 higher odds for mortality (95% CI: (2.74, 19.79), p < 0.001) when compared to patients who did not require mechanical ventilation after being adjusted for other variables. Mechanical ventilation was also an independent predictor of in-hospital mortality (95% CI: 2.74 (2.00–3.76), p < 0.001) among geriatric patients in an ICU setting in Singapore. 11 Another study on intensive care for very elderly patients in a university hospital in Belgium reported the mortality rate in the ICU elderly patients who needed mechanical ventilation of 66.7%. 22 Based on a state-wide database in New York, about one half of the patients who were 30–79 years old and needed mechanical ventilation died in the hospital compared with about three-fourths of those aged over 89 years. 23 These reports collectively demonstrate the negative impact of older age combined with the duration of mechanical ventilation on survival. As the age increases, increasingly abnormal clinical parameters and respiratory physiological measures are commonly seen. Among various diseases, acute lung disease led frequently to prolonged mechanical ventilation due to diminished pulmonary protective mechanisms in a very old age. 24 In addition, the increasing burden of chronic illnesses such as chronic lung diseases, cardiac failure, liver diseases and kidney diseases also negatively affects the outcome.
Old age was sometimes a discriminating factor for aggressive treatment either in critical care or in general health care as a whole.25,26 The findings in this study may contribute to making decision on treatment modality and special care units admission for critically ill geriatric patients. They can also serve to inform clinicians, hospital administrators and policymakers of the needs of geriatric patients when formulating local hospital policies.
Conclusion
Geriatric patients’ attendance to emergency department is a common phenomenon and a significant proportion of them require an initial critical care intervention. Patients receiving ventilator and inotropic support had been observed to exhibit worse clinical outcome. The associated factors for special care units admission were the usage of NIV and inotropic support, while in-hospital mortality had been associated with increased blood urea level, reduced serum albumin level and the requirement for mechanical ventilation.
Limitation
This was a single-centre study, and hence the findings may not be generalizable to other emergency departments. Besides that, the investigator did not follow up the patients after discharge from the hospital, and thus the long-term effect after the emergency department visit on patients’ functional status and quality of life after hospital discharge was not explored. Besides that, the role of NIV in reducing in-hospital mortality despite increasing the chance of special care units admission was not analysed in this study and could be a direction for future research. It is also noted that a good number of cases were not included in the analysis due to incomplete data which might affect the results of this study. A multi-centre, larger sample size study may be conducted to explore new grounds in critically ill geriatric patients.
Footnotes
Acknowledgements
This manuscript is submitted solely to HKJEM journal site and was not published or submitted elsewhere. It had been read and approved by all authors. Special gratitude goes out to all nursing staffs and doctors who assisted in the study, with special mention to the Hospital Director of Hospital Universiti Sains Malaysia and the Human Research Ethics Committee for granting the use of patients’ data as well as the approval for study conduct.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The data and materials were enclosed and available for review.
Ethical approval
Ethical approval was granted by the Human Research Ethics Committee (HREC) of Universiti Sains Malaysia (study protocol code USM/JEPeM/15110480).
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.