
Abstract
Background:
Rapid door-to-balloon times in ST-elevation myocardial infarction patients undergoing primary percutaneous coronary intervention are associated with favorable outcomes.
Objectives:
We evaluated the effects of prearrival direct notification calls to interventional cardiologists on door-to-balloon time for ST-elevation myocardial infarction patients undergoing primary percutaneous coronary intervention.
Methods:
A 24-h hotline was created to allow prearrival direct notification calls to interventional cardiologists when transferring ST-elevation myocardial infarction patients. In an urban, tertiary referral center, patients who visited via inter-facility or the emergency department directly were included. Clinical parameters, time to reperfusion therapy, and in-hospital mortality were compared between patients with and without prearrival notifications.
Results:
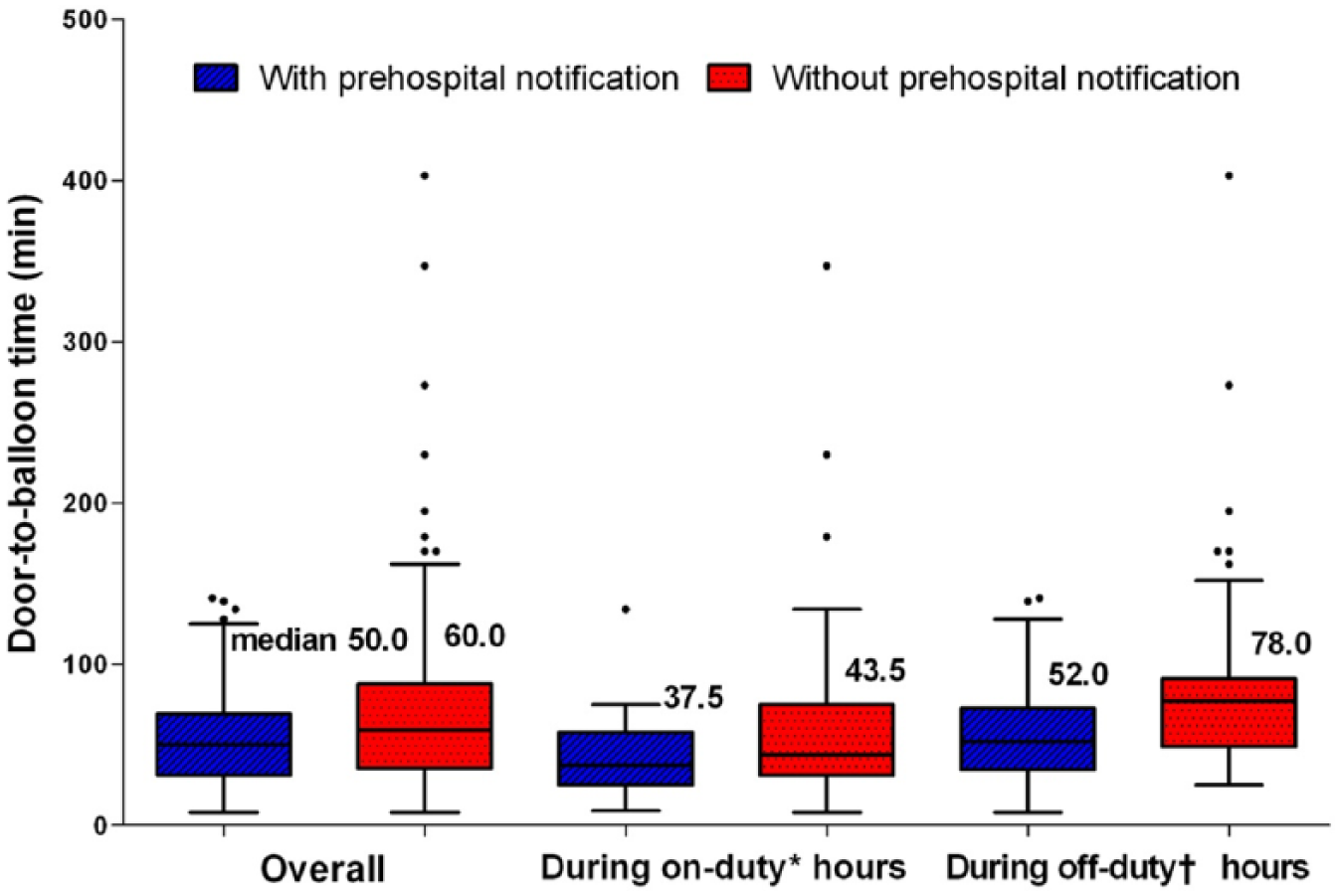
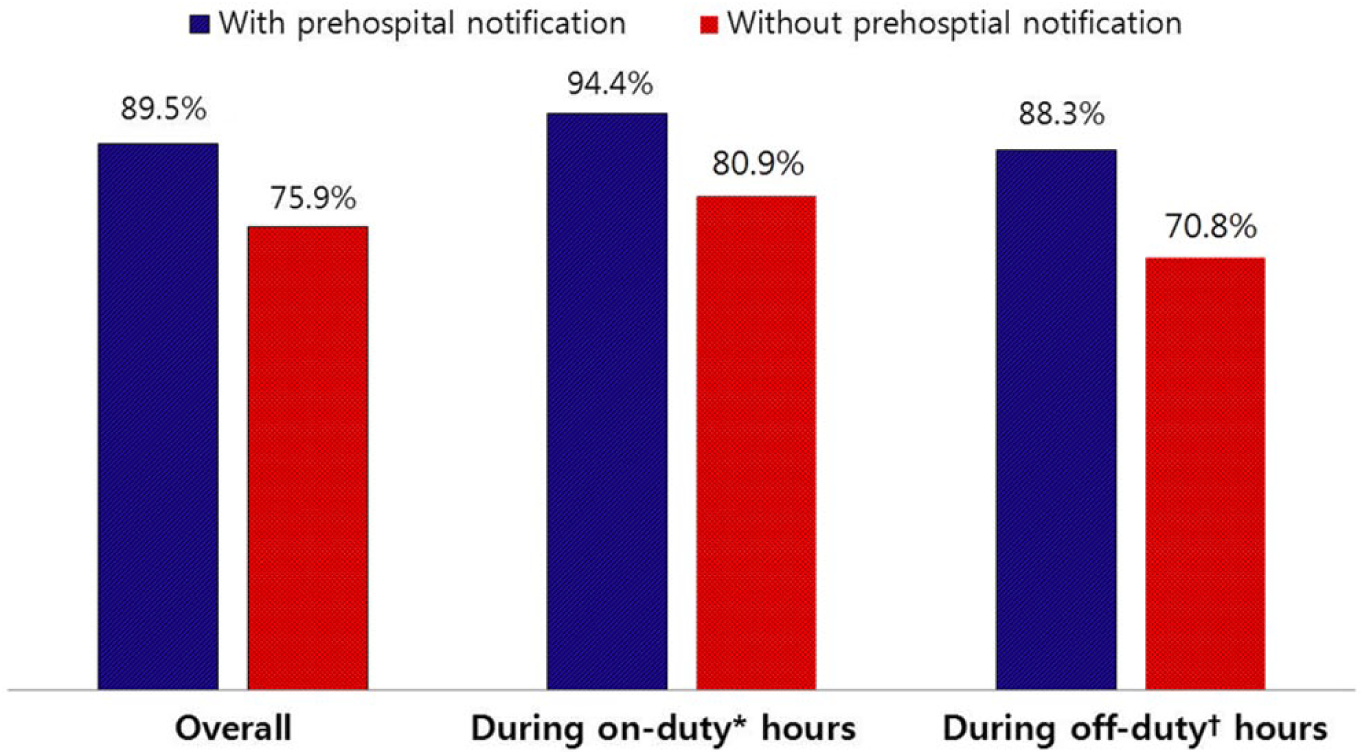
Of 228 ST-elevation myocardial infarction patients, 95 (41.7%) were transferred with prearrival notifications. In these patients, door-to-balloon time was shorter (50.0 vs 60.0 min, p = 0.010) and the proportion of patients with door-to-balloon time < 90 min was higher (89.5% vs 75.9%, p = 0.034) than patients without notifications. These improvements were more pronounced during “off-duty” hours (52.0 vs 78.0 min, p = 0.001; 88.3% vs 72.3%, p = 0.047, respectively) than during “on-duty” hours (37.5 vs 43.5 min, p = 0.164; 94.4% vs 79.4%, p = 0.274, respectively). In addition, door-to-activation time (–39 vs 11 min, p < 0.001) and door-to-catheterization laboratory arrival time (33 vs 42 min, p = 0.007) were shorter in patients with prearrival notifications than those without. However, in-hospital mortality was similar between the two groups (6.3% vs 6.8%, p = 0.892).
Conclusion:
Prearrival direct notification calls to interventional cardiologists significantly improved the door-to-balloon time and the proportion of patients with door-to-balloon time < 90 min through rapid patient transport in primary percutaneous coronary intervention scheduled hospital and readiness of the catheterization laboratory.
Keywords
Introduction
Timely primary percutaneous coronary intervention (PCI) is the optimal reperfusion strategy for ST-elevation myocardial infarction (STEMI) patients. 1 Studies have shown that shortened treatment times for STEMI patients who underwent primary PCI, such as door-to-balloon (DTB) time and transfer time, are strongly associated with improved cardiac function and favorable outcomes.2–4 STEMI patients presenting to a PCI-capable hospital should be treated with primary PCI within 90 min of the DTB time, while STEMI patients in non-PCI-capable hospitals should be transferred immediately for primary PCI if the time from the first medical contact (FMC) to device insertion is expected to be within 120 min. 1 To minimize the transfer time for rapid reperfusion and to achieve guideline-stated target DTB times, several authors have suggested various efficient and coordinated regional strategies, such as prehospital electrocardiographic diagnosis, early activation of cardiac catheterization laboratory (CCL), and direct referral to a PCI-capable center.5–13 We evaluated the effect of prearrival direct notification calls to interventional cardiologists on DTB time when transferring STEMI patients for primary PCI.
Methods
Study population
Our study region was the southeastern city of South Korea, which consisted of 766 km2 and served a population of 3.6 million inhabitants. This prospective observational study was conducted at a university hospital—a 1200-bed, urban, tertiary referral center. From January 2009 to December 2010, we included consecutive patients presenting to the emergency department (ED) with a clinical history and electrocardiographic changes consistent with STEMI who were candidates for primary PCI. Patients were excluded if they visited by walking, were treated with fibrinolysis, delayed PCI due to comorbidities, refused PCI, or died before PCI.
Study setting and protocol
Our hospital’s CCL is available 24 h a day, 7 days a week. During weekdays (07:00–18:00), all members of the PCI team are physically present in the hospital, while during weekends and at nights, an on-call interventional cardiologist is available within 20 min.
Since January 2009, we have implemented a 24-h hotline system with the Emergency Medical Information Center (EMIC) in our city to ensure that an on-duty interventional cardiologist receives a direct notification call from the EMIC in order to reduce inter-hospital transfer delay.
When a patient with chest pain arrives at a community hospital without PCI capability and acute STEMI is suspected, the physician in the community hospital diagnoses acute STEMI based on cardiac biomarker values, symptoms, and electrocardiographic findings and calls the EMIC to transfer the patient immediately to a primary PCI-capable hospital. If our on-duty interventional cardiologist receives a notification call from the EMIC licensed provider, he or she decides whether or not to activate the PCI team with a single call for performing to prepare for emergency coronary angiography with or without primary PCI while the patient is enroute to our hospital. The on-duty interventional cardiologist and PCI team members are required to arrive in the CCL within 20 min after the activation call. When the patient arrives at our hospital, he or she is evaluated briefly in the triage area and transported rapidly to the CCL.
When a STEMI patient is transferred to our hospital without a notification call from the EMIC, or visits the ED directly, an emergency physician evaluates the patient briefly, calls the on-duty interventional cardiologist, and activates the PCI team with a single call.
Primary PCI is performed according to current treatment guidelines for STEMI patients, and other practices including hospital care and medications for the prevention of secondary events are followed. After discharge, all patients are prescribed medications and followed up by their clinicians regularly. Patients who developed angina-like symptoms undergo complete clinical evaluation. If deemed necessary, the patients receive hospital care and revascularization.
For comparison, the study population was classified into patients with a prearrival direct notification call to the interventional cardiologist (prearrival notification group) and those without such calls (no prearrival notification group). All medical data were collected by trained study coordinators using a standardized case report form and protocol. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected by prior approval for this study by the ethics committee of our hospital. Written informed consent for the use of data was obtained from each patient.
Definitions and study endpoints
The primary endpoint was DTB time. Secondary endpoints included the proportion of patients meeting the current guidelines of DTB time <90 min, symptom onset-to-door time, and components of DTB time. Furthermore, DTB times were compared between “on-duty” and “off-duty” hours. “On-duty” hours were defined as a period from 07:00 to 18:00 during Monday through Friday. “Off-duty” hours were all other times or days, including public holidays. “False-alarms” were defined as no lesion on coronary angiography or canceled the activation by decision of emergency physician or interventional cardiologist.
Statistical analysis
Sample size calculations with an effect size of 0.5, alpha-error probability of 0.05, and power of 0.9 require 172 subjects to detect significant effects (G*Power 3.1.9.2, University of Kiel). 14 Taking into account a possible dropout rate of one-tenth, we considered a sample size of 189 subjects as appropriate to study effects. Categorical variables were expressed as numbers with percentages and compared using Chi-square’s test or Fisher’s exact test, where appropriate. Continuous variables were expressed as mean ± standard deviation or median with interquartile ranges and compared using the independent t-test or Mann–Whitney test, where appropriate. To adjust for known confounding factors, we performed the multivariate regression analysis with DTB time as a dependent variable. The adjusted covariates included age, gender, hypertension, diabetes mellitus, prior ischemic heart disease, Killip class, left ventricular ejection fraction, time of arrival (on-duty or off-duty hours), extent of coronary disease, culprit vessel location, lesion type, initial thrombolysis in myocardial infarction flow grade, and vascular access site. p < 0.05 was considered statistically significant. All analyses were performed using SPSS 17.0 for Windows (SPSS Inc., Chicago, IL).
Results
A total of 228 consecutive STEMI patients who underwent primary PCI during the study period were included in this study. Of these, 95 patients (41.7%) were referred with prearrival direct notification calls from the EMIC, and 133 patients (58.3%) were either transferred without such calls or visited the ED directly. No significant differences were noted in the baseline clinical characteristics between the two groups (Table 1). The prearrival notification call was more common during “off-duty” hours than during “on-duty” hours (81.2% vs 18.9%, p < 0.001). Angiographic and procedural characteristics did not differ between the two groups (Table 2). In addition, of 95 patients with prearrival notification, false alarms occurred in 14 patients (14.7%).
Baseline clinical characteristics.
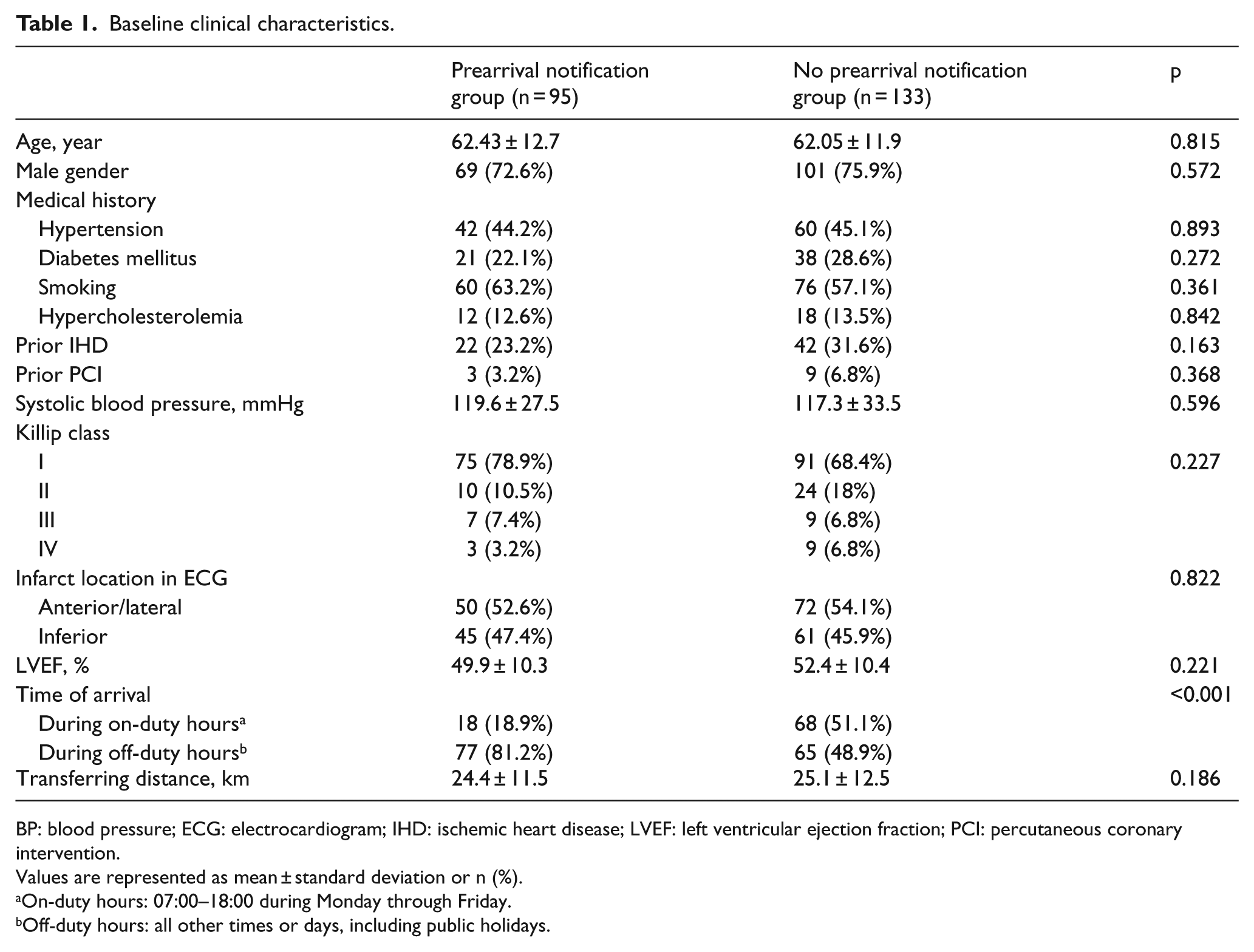
BP: blood pressure; ECG: electrocardiogram; IHD: ischemic heart disease; LVEF: left ventricular ejection fraction; PCI: percutaneous coronary intervention.
Values are represented as mean
On-duty hours: 07:00–18:00 during Monday through Friday.
Off-duty hours: all other times or days, including public holidays.
Angiographic and procedural characteristics.
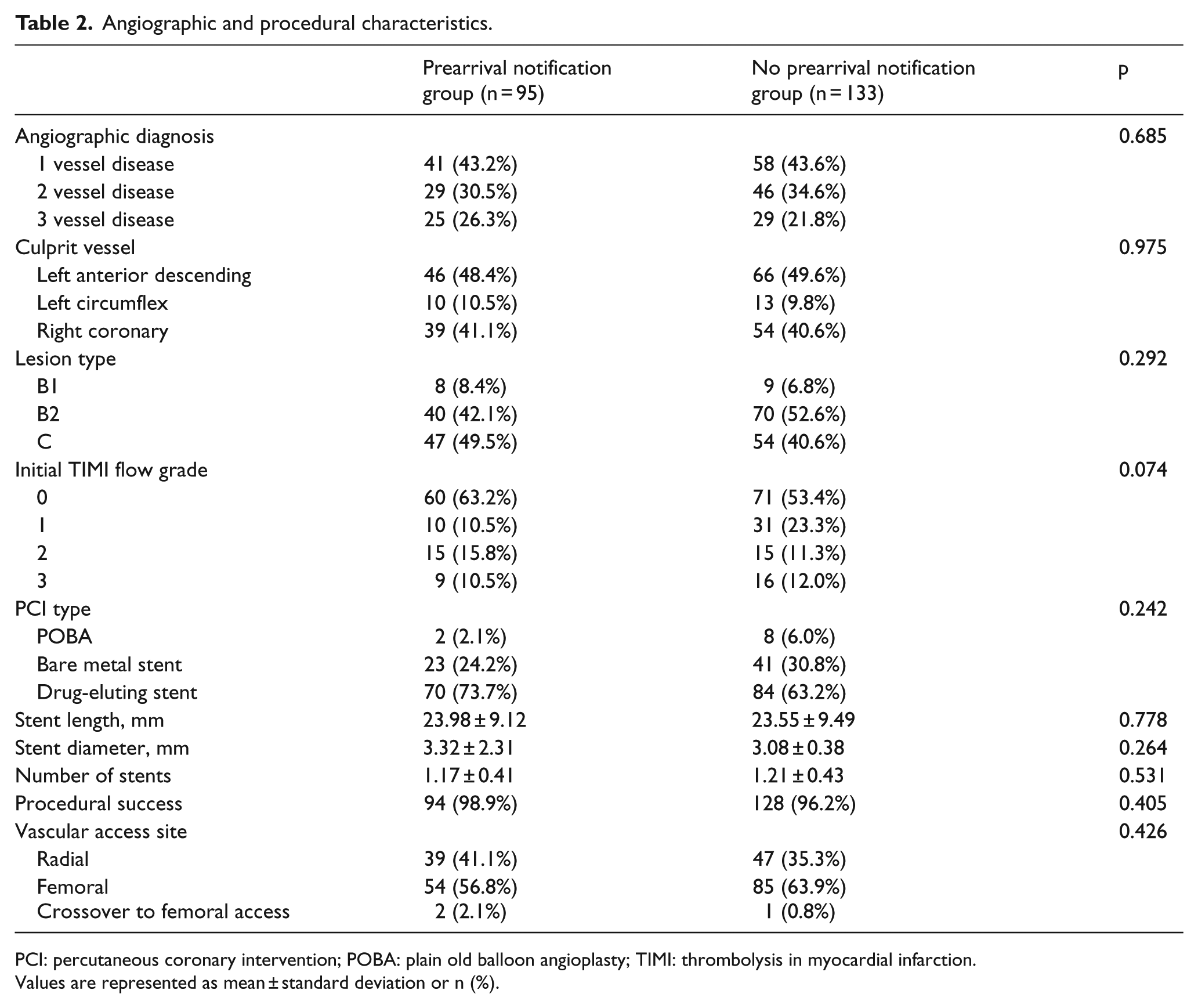
PCI: percutaneous coronary intervention; POBA: plain old balloon angioplasty; TIMI: thrombolysis in myocardial infarction.
Values are represented as mean
The DTB time was significantly shorter in patients with prearrival notification compared to patients without it (Table 3). The improvement in DTB time was greater during “off-duty” hours than during “on-duty” hours (Table 3, Figure 1). The proportion of patients with DTB time <90 min was significantly higher in the prearrival notification group compared to the no prearrival notification group. The increase in the proportion of patients with DTB time < 90 min was greater during “off-duty” hours than during “on-duty” hours (Table 3, Figure 2).
Comparison of door-to-balloon time.
The proportion of patients with door-to-balloon time <90 min.
Comparison of door-to-balloon time and PCI stratified by door-to-balloon time.
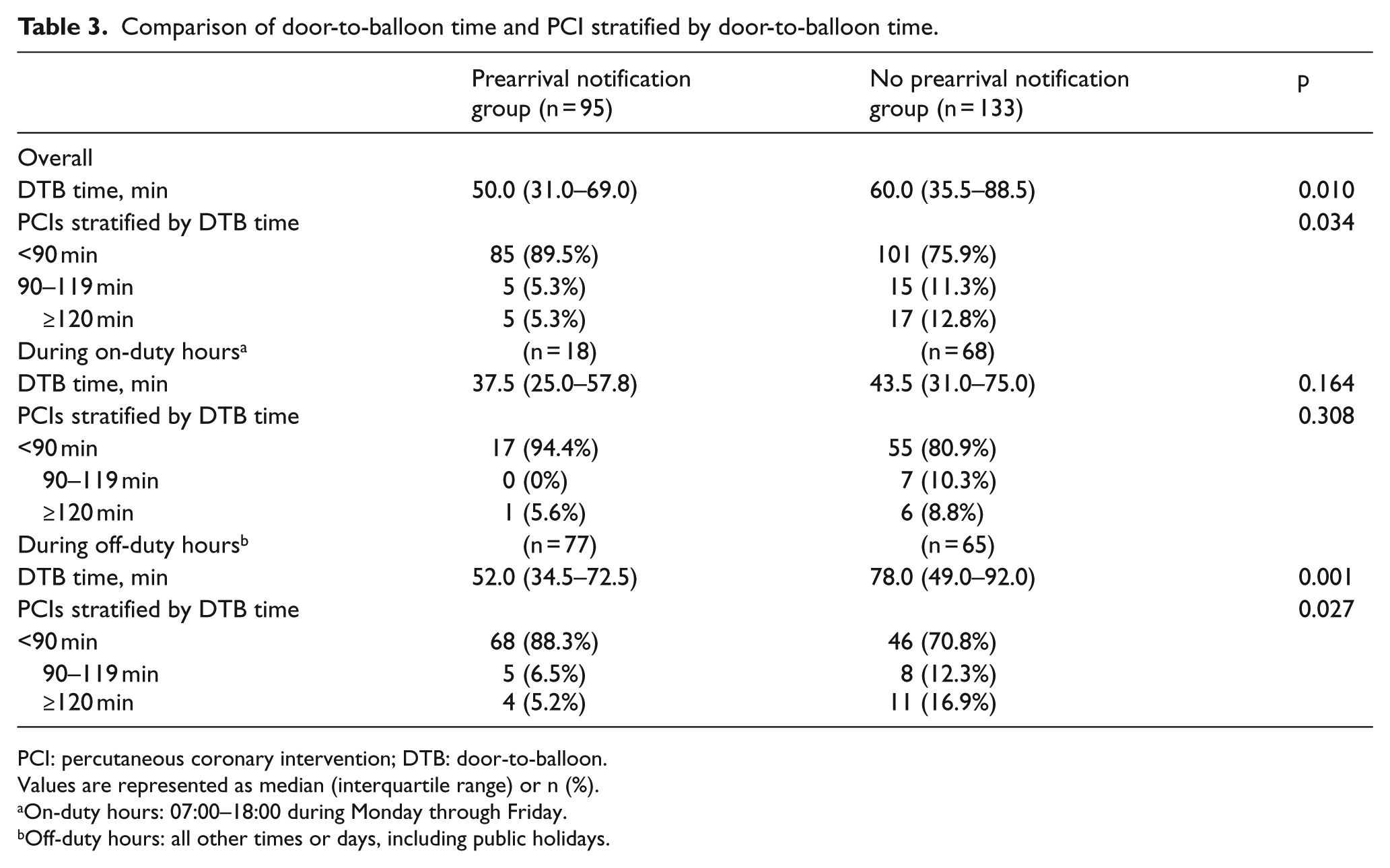
PCI: percutaneous coronary intervention; DTB: door-to-balloon.
Values are represented as median (interquartile range) or n (%).
On-duty hours: 07:00–18:00 during Monday through Friday.
Off-duty hours: all other times or days, including public holidays.
Concerning the components of DTB time, door-to-activation time and door-to-CCL arrival time were significantly shorter in the prearrival notification group than in the no prearrival notification group (Table 4). In the subgroup of both community and PCI-capable hospitals, DTB time, door-to-activation time, and door-to-CCL arrival time were still significantly shorter in the prearrival notification group than in the no prearrival notification group (Table 4). The negative value indicates that the PCI team activation had been completed before the patient arrived at the door of the ED. In multivariate regression analysis, the prearrival notification was associated with improved DTB time (p = 0.021). The in-hospital mortality did not differ between the two groups (6.3% vs 6.8%, p = 0.892).
Comparison of time components of percutaneous coronary intervention.
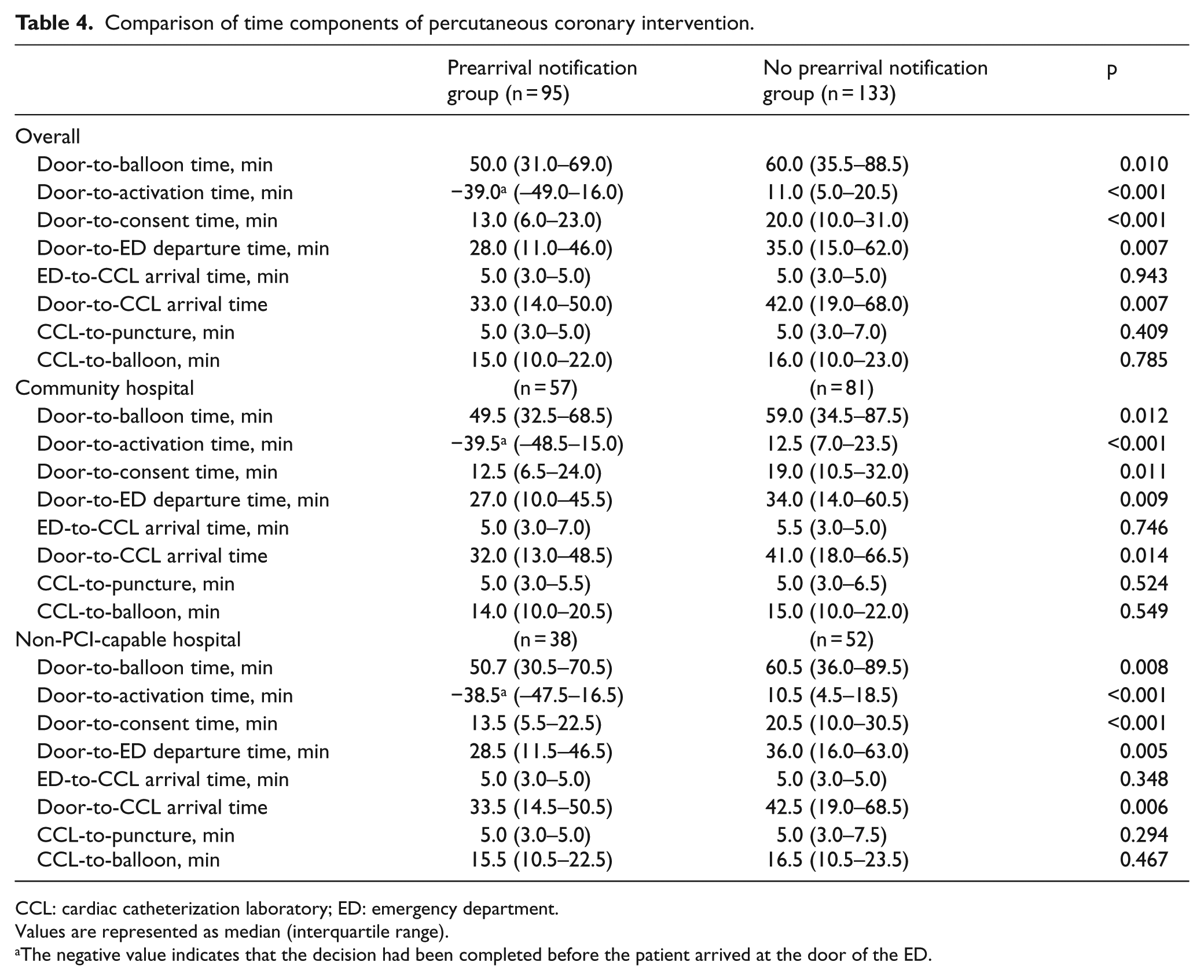
CCL: cardiac catheterization laboratory; ED: emergency department.
Values are represented as median (interquartile range).
The negative value indicates that the decision had been completed before the patient arrived at the door of the ED.
Discussion
The major findings of this study are as follows. (1) In STEMI patients transferred for primary PCI, the DTB time was significantly shorter and the proportion of patients with DTB time <90 min was significantly higher in patients with a prearrival direct notification call to the interventional cardiologist compared with patients without such calls; (2) this improvement in DTB time and the proportion of patients with DTB time <90 min was more pronounced during “off-duty” hours than during “on-duty” hours; and (3) among the components of DTB time, the door-to-activation time and door-to-CCL arrival time was significantly shorter in patients with a prearrival direct notification call to the interventional cardiologist compared with patients without such calls. Based on our analyses, we support that the prearrival notification was strongly associated with better DTB time. Moreover, it can be postulated that the reduction of DTB time was mainly driven by the decreased door-to-activation time and door-to-CCL arrival time. We proved that prearrival notification may contribute to early activation, rapid CCL arrival, and timely reperfusion therapy.
Certain strategies have been suggested for reducing DTB time during primary PCI in STEMI patients. Ting et al. 8 and Diercks et al. 9 reported that prehospital ECG could result in the significant decrease in DTB time. Moreover, prehospital activation of the CCL 10 or cardiologist, 11 prehospital diagnosis and direct transfer to the PCI center, 7 and shorter interval from hospital arrival to STEMI diagnosis and CCL activation 12 were all associated with improvements in DTB time for STEMI patients undergoing PCI. Bradley et al. 5 suggested six strategies that were significantly associated with faster DTB time, including the following: (1) emergency physicians activate the CCL (mean reduction in DTB time, 8.2 min); (2) a single call to a central page operator activates the laboratory (13.8 min); (3) the ED activates the CCL while the patient is enroute to the hospital (15.4 min); (4) the staff arrive in the CCL within 20 min after being paged (19.3 min); (5) an attending cardiologist is always on site (14.6 min); and (6) the staff in the ED and the CCL use real-time data feedback for ongoing training (8.6 min). Herein, if an emergency physician at a non-PCI-capable hospital identified a patient with suspected STEMI, he or she called the EMIC to seek the nearest primary PCI-capable hospital. Then, when the EMIC licensed provider directly called an on-duty interventional cardiologist at the PCI-capable hospital, the interventional cardiologist decided whether to activate the CCL staff members while the patient was enroute to the referral hospital. In our system, the cooperation between the emergency physician at the non PCI-capable hospital, the EMIC licensed provider, and the on-duty interventional cardiologist at the referral PCI-capable hospital was the key in reducing the DTB time. In our no prearrival notification group, the physicians at a non-PCI-capable hospital did not know about this prearrival notification system or thought that a direct transferring of acute STEMI patients would take a shorter time than the transferring after prearrival notification call to interventional cardiologist via EMIC. However, we showed that the prearrival notification call to interventional cardiologist was associated with improved DTB time. Thus, we are planning an extended use of this system in our city.
Other time interval parameters in STEMI patient care have been affected by new practices. Prehospital ECG by wireless systems, computing algorithms, and paramedics training have contributed to improvements in the time to reperfusion therapy, such as FMC-to-door time, door-to-ECG time, and ECG-to-balloon time. 8 Moreover, a prehospital ECG and the subsequent direct transfer to a PCI-capable hospital are known to reduce FMC-to-door time, door-to-CCL time, and FMC-to-balloon time.6,13 Rapid decision-making by prehospital PCI risk calculation would also be associated with improvements in reperfusion time. However, additional studies are needed to assess the effects of prehospital PCI risk calculation on time to coronary intervention. Herein, the inclusion of a prearrival direct notification call to the interventional cardiologist decreased various components of DTB time, including door-to-activation time and door-to-CCL arrival time. We postulate that a prearrival direct notification to the interventional cardiologist leads to a reduction in DTB time by early activation of the CCL team and rapid patient transport to the CCL in our hospital.
The effects of primary PCI during “off-duty” hours versus “on-duty” hours on DTB time and mortality have been inconclusive. Investigators have reported that longer DTB times and higher mortality are found in STEMI patients undergoing primary PCI during “off-duty” hours than during “on-duty” hours.15,16 Holmes et al. 17 and Casella et al. 18 showed improvements in DTB time and mortality during “off-duty” hours by specialized STEMI network strategies. Herein, patients with a prearrival notification call had shorter DTB time and higher rates of patients meeting DTB time <90 min than those without such calls, particularly during “off-duty” hours.
The proportion of “false alarms” in prehospital STEMI diagnosis and activation of CCL teams is substantial, although the definition of “false alarms” has been inconsistent in previous studies. Garvey et al. 19 reported that in CCL activation at 14 primary PCI hospitals participating in a statewide STEMI reperfusion program, inappropriate CCL activations occurred in 596 (15%) of 3973 patients. McCabe et al. 20 observed that 146 false alarms (35.5%) occurred in 411 STEMI activations in patients with suspected STEMI at two primary PCI-capable hospitals. False alarms comprised approximately 15% of patients in our study although an interventional cardiologist decided whether to activate CCL after ECG information was imparted by the EMIC licensed provider. Concomitant transmission of the ECG to a cellphone could reduce the number of false alarms that activate CCL teams in advance. 8
Reducing time to PCI in STEMI patients results in enhanced cardiac function and improved clinical outcomes. CADILLAC trial showed that early reperfusion contributed to the improved left ventricular function, microvascular reperfusion, and survival. 4 McNamara et al. 3 concluded that a longer DTB time was associated with increased in-hospital mortality. A recent study found that the DTB time improved significantly during 4 years of follow-up, however, in-hospital mortality remained unchanged. 21 This study also demonstrated comparable in-hospital mortality between groups, although the DTB time reduced significantly in the prearrival notification group compared with the no prearrival notification group. The reason for no improvement of in-hospital mortality in our study may be attributable to no further reduction of the total ischemia time. Multimedia public education campaigns, feedback to every care provider, and continuous training and education to hospitals and care providers are important methods for reducing the overall ischemic time and achieving improved prognoses.22,23
Limitations
This study has some limitations. First, the sample size was relatively small. Second, this study was limited to a single academic medical center with continuous availability of a CCL and staff. However, this study does serve as a feasibility study for other medical centers. Third, we did not compare the rate of “false alarms” accurately between the two groups. Bradley et al. 24 have reported that in top-performing hospitals, such “false alarms” occur rarely and are acceptable. Finally, the prearrival call to emergency physicians at a primary PCI-capable hospital might decrease the DTB time, but we could not evaluate the impact of prearrival call to emergency physicians on DTB time.
Conclusion
This study showed that prearrival direct notification calls to interventional cardiologists significantly reduced the DTB time and significantly increased the proportion of patients with DTB time <90 min through rapid patient transport in primary PCI scheduled hospital and readiness of the catheterization laboratory. These improvements were more pronounced during “off-duty” hours than during “on-duty” hours. Our results suggest that a regional network using prearrival notifications through an information center may be an effective community-wide strategy for timely reperfusion in STEMI patients, particularly during “off-duty” hours.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.