
Abstract
A 52-year-old man without systemic disease presented to the emergency department with sudden-onset epigastric pain for 2 h. He had vomiting for several times without fever, diarrhea, or recent abdominal trauma. Point-of-care ultrasound revealed flap in the superior mesenteric artery. Percutaneous endovascular stent placement was arranged due to refractory upper abdominal pain and poor response to medical treatment.
Case history
A 52-year-old man with no past medical history presented to the emergency department due to sudden-onset epigastric pain and vomiting for 2 h. Physical examinations revealed a soft abdomen and epigastric tenderness on palpation without rebound tenderness. Point-of-care ultrasonography of the abdomen was performed (Figure 1(a) and (b)).
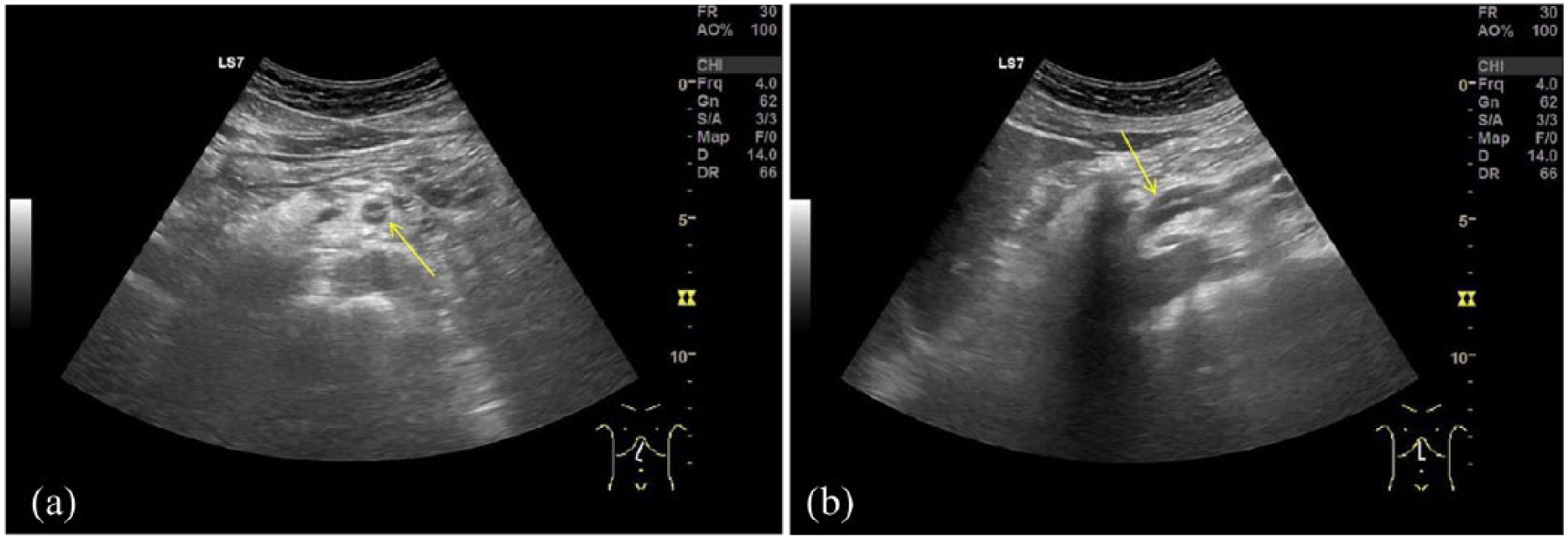
Ultrasonography of the (a) short-axis of upper abdomen and (b) long axis of upper abdomen.
Questions
What are ultrasound findings?
What is the diagnosis and treatment?
What is the clinical importance of point-of-care ultrasound for patients with acute abdominal pain?
Answers
Ultrasonography of the short axis and long axis of upper abdomen showing an intimal flap in the superior mesenteric artery (Figure 1(a) and (b), arrow).
The diagnosis was superior mesenteric artery dissection. Computed tomography (CT) of abdomen confirmed the diagnosis (Figure 2). The patient was treated with heparinization, hydration, pain control, and bowel rest. Due to persistent pain, endovascular stent was inserted and patient was discharged under stable condition.
Point-of-care ultrasound is an easy accessible and noninvasive screening modality that can be used in the emergency department to evaluate for patients presenting with acute abdominal pain related to vascular emergencies such as abdominal aortic aneurysm, dissecting aortic aorta, or superior mesenteric artery dissection.
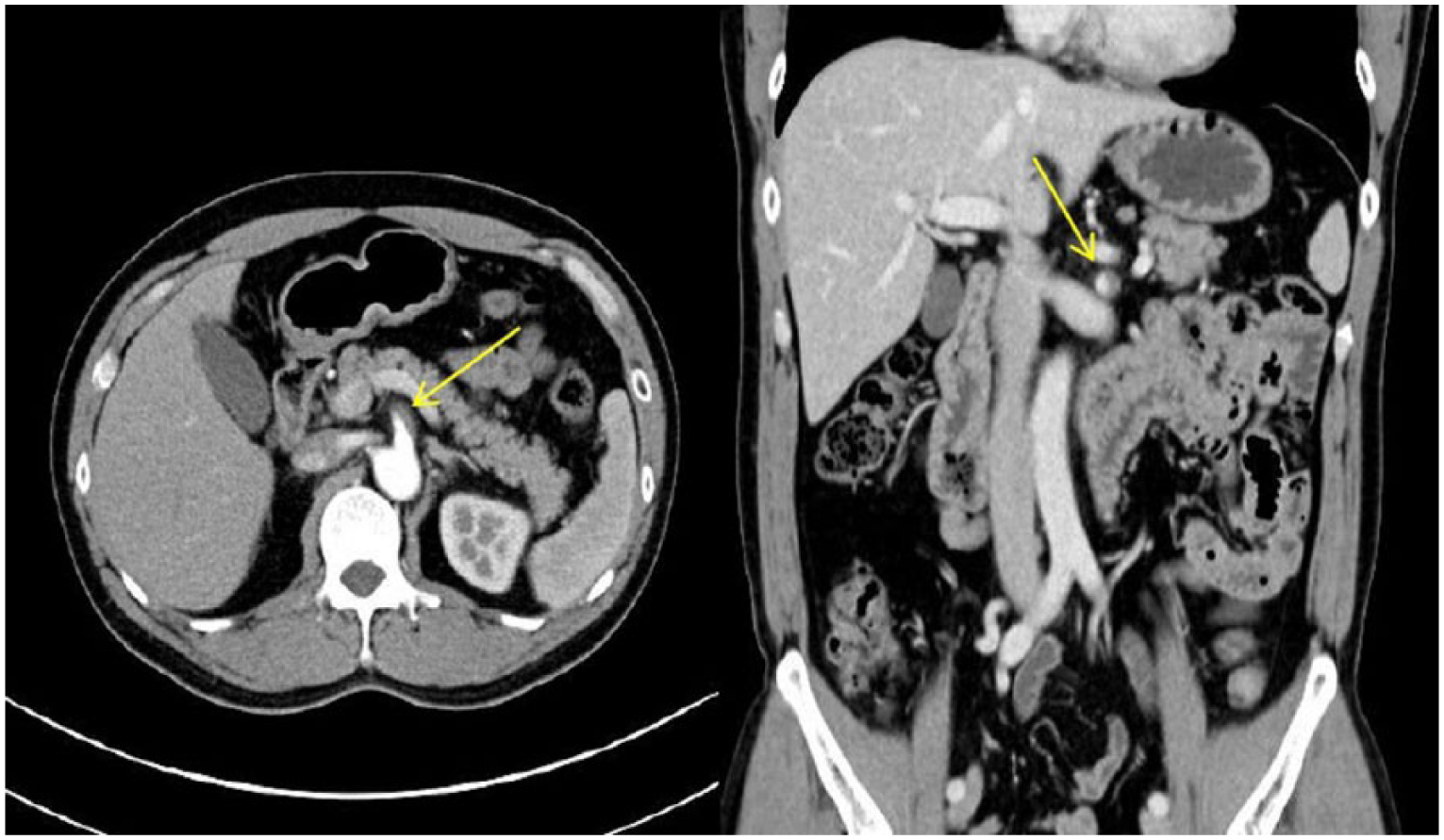
Computed tomography of the abdomen: axial (left panel) and coronal (right panel) CT image demonstrated intimal flap and filling defects (arrow) of the proximal SMA, suggesting SMA dissection.
Discussion
Spontaneous isolated superior mesenteric artery dissection is a rare but potentially fatal disease if not promptly diagnosed. The pathophysiology of superior mesenteric artery dissection was not clearly determined but may be related to iatrogenic or trauma, atherosclerosis, hypertension, cystic medial necrosis, fibromuscular dysplasia, and segmental arterial mediolysis. 1 Most patients with superior mesenteric artery dissection typically present with sudden onset of abdominal pain, which may relate to direct effects of dissection or intestinal ischemia. Patient with bowel ischemia or artery rupture should be managed with emergent laparotomy and repair. 2 Asymptomatic patients or symptomatic patients without evidence of bowel ischemia or artery rupture can be managed with conservative treatment such as bowel rest, blood pressure control, pain control, anticoagulation, and/or antiplatelet agents. Percutaneous endovascular stent placement can be used for symptomatic patients with poor response to medical treatments and high risk for surgery. 3
Footnotes
Acknowledgements
All authors equally contributed to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study procedures were in accordance with ethical standards.