
Abstract
Introduction:
Acute myocardial infarction is one of the most devastating cardiovascular diseases and about 50% of all deaths due to it occur prior to hospitalization. Our study aimed to evaluate the prehospital delay in patients with acute myocardial infarction.
Methods:
We enrolled 682 consecutive patients with acute myocardial infarction from May 2008 to December 2014, with a mean age of 66.6 ± 12.9 years. Detailed information was collected about the symptoms, first medical contact, concomitant clinical conditions, and the socioeconomic data. We analyzed the following prehospital times: (1) onset of symptoms to emergency call, (2) onset of symptoms to first medical contact, (3) first medical contact to hospital admission, and (4) onset of symptoms to hospital admission.
Results:
The first medical contact was with the National Emergency Medical Service in 266 (39.0%) patients, another emergency unit 106 (15.6%), cardiologist 41 (6%), general practitioner 36 (5.3%), and others 233 (34.1%). The median time from the onset of symptoms till emergency call was 190 min, from the first contact with a team of the National Emergency Medical Service till hospital admission 60 min, and from the onset of symptoms till hospital admission 4.8 h.
Conclusion:
The total prehospital delay in our study was unacceptably prolonged, with patient’s decision time as the major contributor. The delay could be substantially shortened by (1) increased awareness of the general population, particularly of individuals at high cardiovascular risk and (2) continuous medical education and regular practical training of the primary care providers about coping with medical emergencies.
Introduction
Cardiovascular diseases are the leading cause of death worldwide.1–4 According to the World Health Organization, 17.7 million people died from cardiovascular diseases in 2015, representing 31% of all global deaths: of them 7.4 million were due to coronary heart disease.2,3 This disease could be presented in different clinical forms and acute myocardial infarction (AMI) is the most life-threatening one.5,6,7 It is generally associated with ~30% mortality rate and about 50% of the deaths occur prior to arrival at the hospital.1,6,7 Overall, prognosis is highly variable and depends largely on the extent of the infarct, the residual left ventricular function, and whether the patient underwent revascularization.5,6,8 Early recognition and evaluation of patients with AMI and rapid transportation to a specialized coronary care unit are crucial for timely revascularization and improved clinical outcomes.6,8 Clinical studies showed that prehospital delay in AMI was associated with decreased possibility of revascularization and mortality increased with time to reperfusion therapy.5,6,9 Patients with AMI treated within 2 h of infarction onset receive the most clinical benefit from reperfusion treatment.6,8–14 These facts gave us a reason to evaluate the prehospital care of patients with AMI referred to the largest emergency hospital in Bulgaria, located in the capital city of Sofia, aiming to identify the determinants and degree of prehospital delay.
Methods
In our prospective observational study, we included 682 consecutive patients with AMI, hospitalized from May 2008 to December 2014 at the largest emergency hospital in Bulgaria, located in the capital city of Sofia. The inclusion criteria were as follows:
Detection of rise of cardiac troponin T (TnT) and/or megabyte (MB) fraction of creatine kinase (MBCK) with at least one value above the 99th percentile of the upper reference limit measured with a coefficient of variation ≤10%, as recommended by the current European Society of Cardiology (ESC) Guidelines for diagnosis of AMI5–7
Symptoms of acute myocardial ischemia or electrocardiographic changes consistent with AMI,5–7 concomitant to pathologically increased TnT and/or MBCK
Type 1 AMI according to the universal definition of myocardial infarction 7
Age ≥18 years
Written informed consent for participation in the study
Feasible follow-up of the patients during their hospital stay.
Exclusion criteria for our study were as follows:
Pathologically increased TnT and/or MBCK due to proven alternative condition/disease
AMI type 2 to type 5 according to the universal definition of myocardial infarction 7
Mentally disabled patients (irrespective of the reason) unable to understand or sign the written informed consent
Transfers from or to other hospitals
Previous AMI in the last 30 days.
An approval of the study was obtained from the local ethics committee. The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The detailed medical history was taken from each patient and/or from the available medical documentation about the (1) onset of clinical symptoms, (2) concomitant cardiovascular risk factors and diseases, (3) demographic and socioeconomic data, and (4) first medical contact (FMC). We analyzed the following prehospital time intervals: (1) onset of symptoms to emergency call, (2) onset of symptoms to FMC, (3) FMC to hospital admission, and (4) onset of symptoms to hospital admission.
Statistical analysis
The statistical analysis was performed by SPSS statistical package, version 16.0 (SPSS Inc, Chicago, IL). The data were summarized by frequencies and percentages for the categorical variables and by minimal, maximal, mean values, and standard deviation for the continuous ones as well as median for very skewed data distribution. For comparison of categorical variables, we used independent χ2 test and Fisher’s exact test. The normality of distribution of continuous data was assessed by Shapiro–Wilk test. T-test and analysis of variance (ANOVA) were used for comparison of parametric data and Mann–Whitney U test and Kruskal–Wallis test for nonparametric ones. Univariate logistic regression was used for evaluation of the independent influence of various variables on the risk for in-hospital complications as well as odds ratio (OR) for the strength of each variable. The results were considered to be statistically significant for p value <0.05.
Results
A total of 431 (63.2%) of our AMI patients were males; p value for males/females was <0.001. Table 1 shows some basic characteristics of the analyzed population.
Characteristics of the study participants at enrollment.
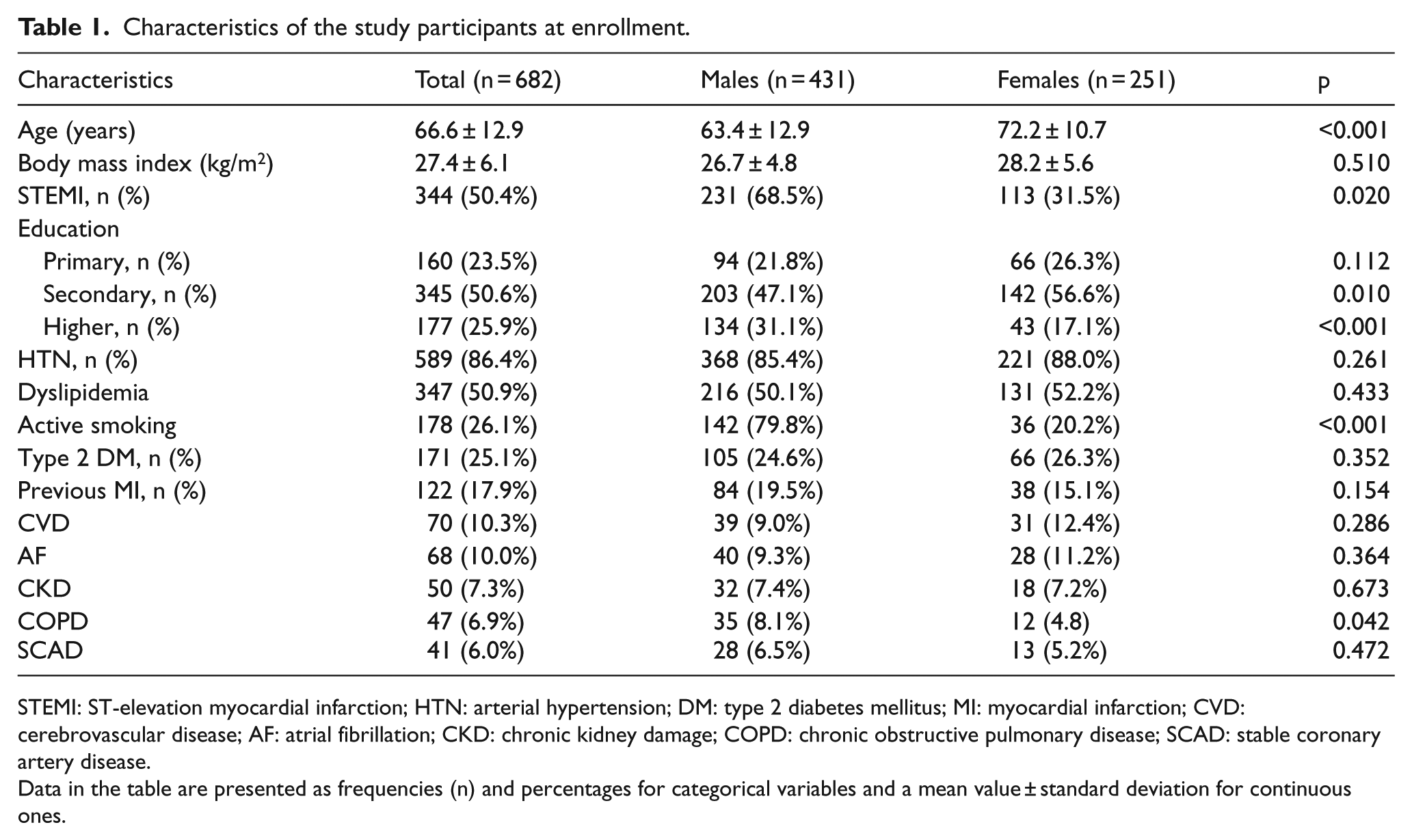
STEMI: ST-elevation myocardial infarction; HTN: arterial hypertension; DM: type 2 diabetes mellitus; MI: myocardial infarction; CVD: cerebrovascular disease; AF: atrial fibrillation; CKD: chronic kidney damage; COPD: chronic obstructive pulmonary disease; SCAD: stable coronary artery disease.
Data in the table are presented as frequencies (n) and percentages for categorical variables and a mean value ± standard deviation for continuous ones.
FMC was with the National Emergency Medical Service (EMS) for 266 (39.0%), another emergency unit 106 (15.6%), a cardiologist 41 (6%), a general practitioner (GP) 36 (5.3%), and others 233 (34.1%). In all, 105 (15.4%) patients were transported by the National EMS, 196 (28.7%) by another emergency service, and 381 (55.9%) by private/other transport (p < 0.001).
Onset of symptoms to emergency call
The median from the onset of symptoms till emergency call was 190 min. For patients who called the National EMS, it was 180 min. For patients who called another emergency service, the median of this interval was 241 min, and for those who called a non-emergency medical institution, it was 305 min (p = 0.164).
Onset of symptoms to first medical contact
The median of the time from the onset of symptoms till FMC was 3.5 h. For patients who contacted the National EMS, it was 3.7 h. The median from the emergency call till arrival and departure of the ambulance was 15 min. The median from the onset of symptoms till FMC for patients who contacted another emergency service was 3.2 h, a GP 7.7 h, a cardiologist 3.4 h, another clinical specialist 4.2 h, and a nurse 4.9 h (p < 0.001).
First medical contact to hospital admission
The median of the time from the FMC with the National EMS till hospital admission was 60 min. The median of the time from the FMC with another emergency service till hospital admission was 90 min, a GP 110 min, a cardiologist 90 min, another clinical specialist 105 min, and a nurse 118 min (p < 0.001). For diabetics, the median of this interval was 72.5 min, and it was 55.0 min for non-diabetics (p = 0.023); for hypertensives, the median time was 60.0 min, and it was 50.0 min in patients without arterial hypertension (p = 0.001); and for patients with cerebrovascular disease (CVD), the median time was 67.5 min, and it was 55.0 min for patients without CVD (p = 0.031).
Onset of symptoms to hospital admission
The median time from the onset of symptoms till hospital admission was 4.8 h: 4.2 h for males and 5.8 h for females (p = 0.003). For patients with ST-elevation myocardial infarction (STEMI), the median of this interval was 4.3 h, and for non-ST-elevation myocardial infarction (NSTEMI), it was 5.4 h (р = 0.001). The median time from the onset of clinical symptoms till hospital admission according to patient’s education was as follows: primary education—6.3 h, secondary education—4.4 h, and higher education—3.8 h (p = 0.022).
Figure 1 shows the percentage of patients within three of the time intervals assessed by us.5–7
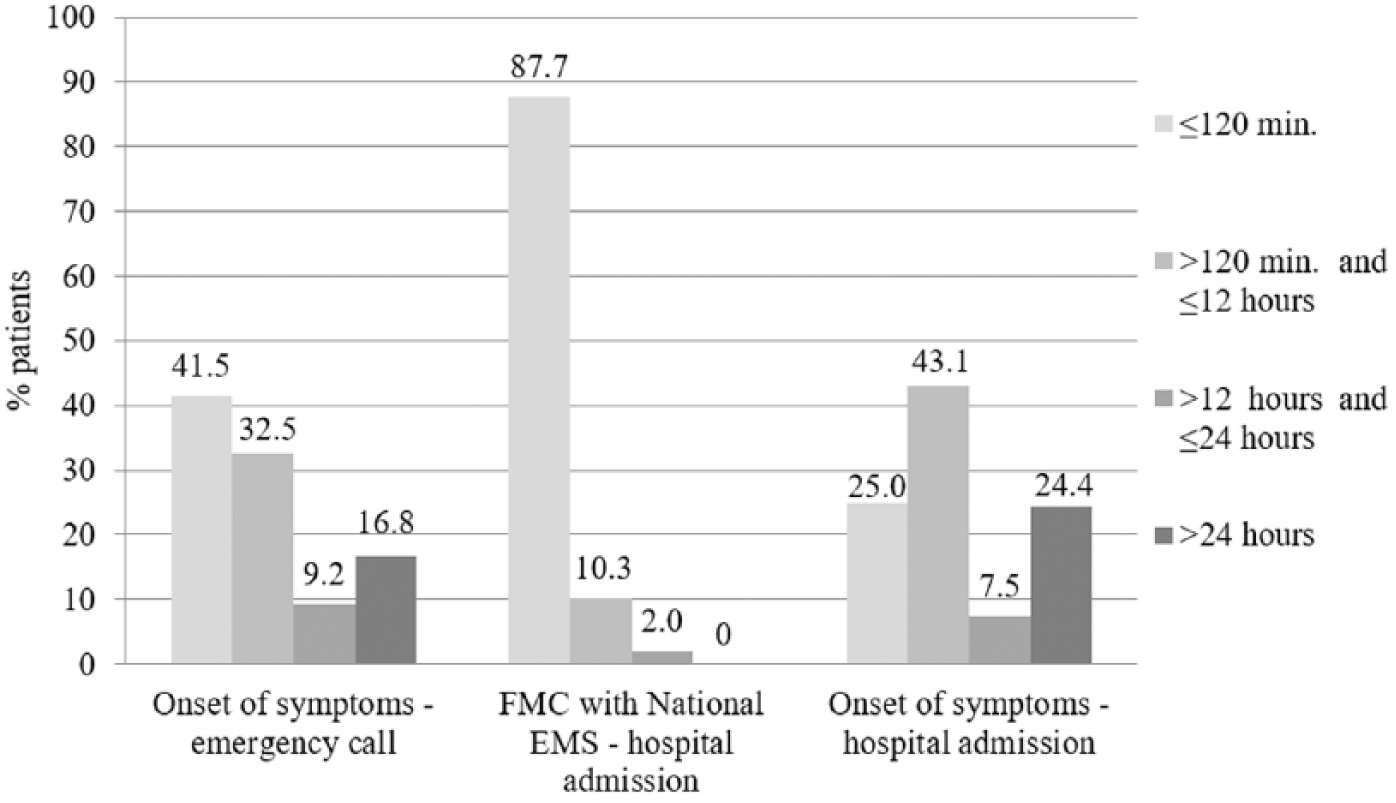
Percentage of patients within three of the assessed time intervals in our study (p < 0.001).
The time interval from the onset of symptoms till hospital admission according to the FMC is shown in Figure 2.
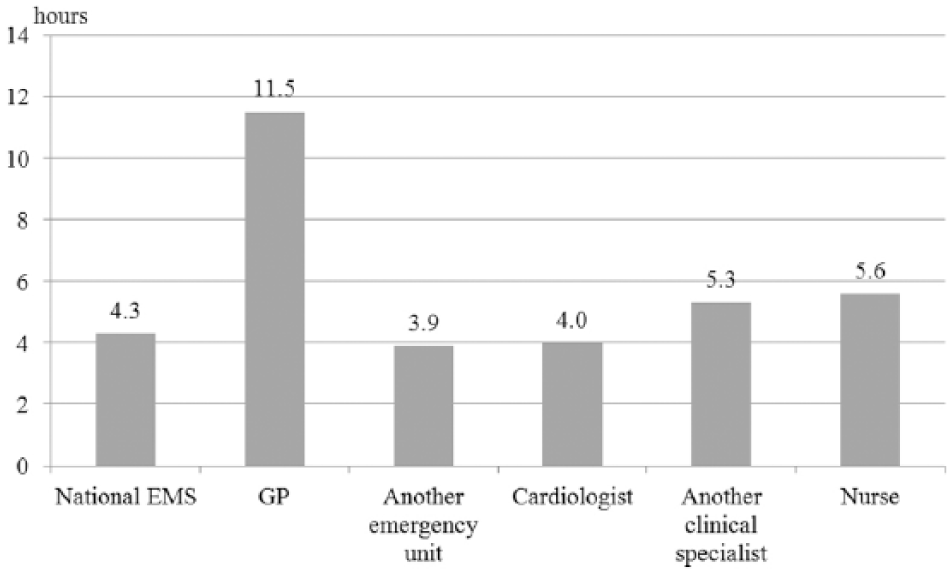
Time interval (expressed by the median value) from the onset of clinical symptoms till hospital admission according to FMC; p < 0.001 for FMC with a GP versus National EMS, another emergency unit, a cardiologist, another clinical specialist, or a nurse; p = 0.004 for FMC with National EMS versus another clinical specialist or a nurse; and p = 0.002 for FMC with another emergency service versus another clinical specialist or a nurse. Another emergency unit—emergency unit or another emergency service, not managed by the National EMS.
Treatment
The therapeutic approach was as follows: conservative—288 (42.2%), percutaneous coronary intervention (PCI)—394 (54.1%), and fibrinolysis—25 (3.7%). Of all AMI patients transported by the National EMS, 89.5% (94 of 105) had reperfusion therapy compared to 75.5% (148 of 198) of those transported by another emergency service and 46.5% (177 of 381) by private/other transport (p < 0.001). The median time from the onset of symptoms till coronary reperfusion was 4.9 h: 4.6 h for National EMS users, 4.8 h for patients transported by another emergency service, and 7.8 h for those using private/other transport (p = 0.03).
Clinical outcome
In-hospital mortality was 13.6% (n = 89): 14 of these patients (15.7%) were transported by the National EMS, 21 (23.6%) by another emergency service, and 57 (60.7%) by private/other transport (p < 0.001). In-hospital complications occurred in 18.9% (n = 129) of all patients who survived AMI for the follow-up period. Table 2 demonstrates the different prehospital factors with significant impact on the risk for development of in-hospital complications after AMI according to the logistic regression analysis.
Impact of demographic and socioeconomic factors on the risk for development of in-hospital complications after AMI.
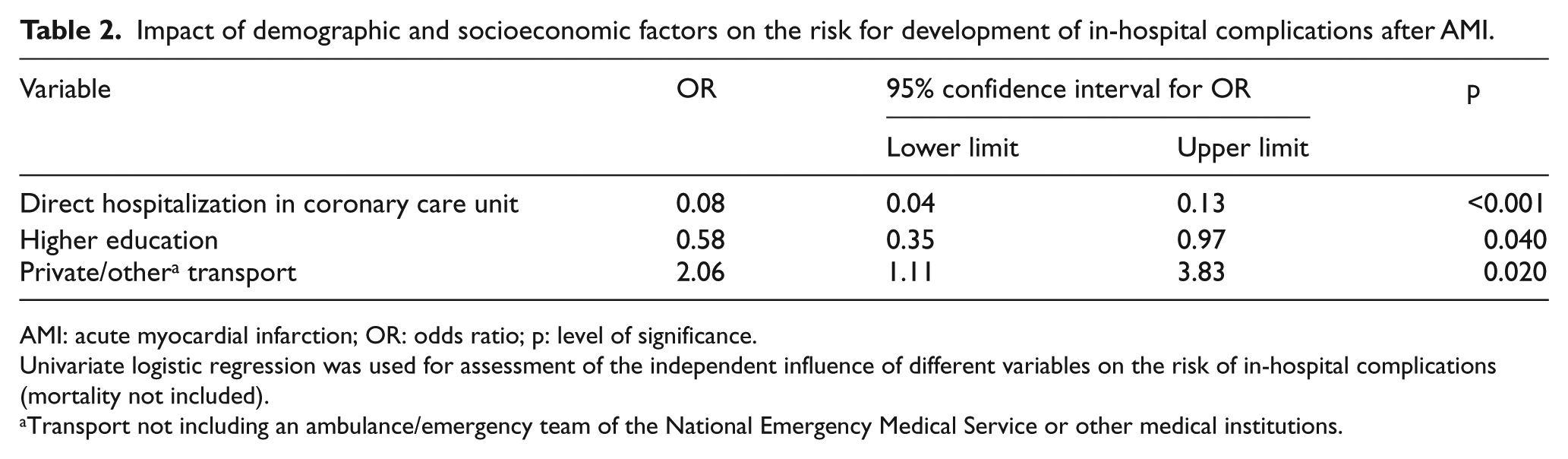
AMI: acute myocardial infarction; OR: odds ratio; p: level of significance.
Univariate logistic regression was used for assessment of the independent influence of different variables on the risk of in-hospital complications (mortality not included).
Transport not including an ambulance/emergency team of the National Emergency Medical Service or other medical institutions.
Discussion
Our results showed that the total period from the onset of the clinical symptoms till hospital admission was unacceptably long—a median of 4.8 h with only 25% of the patients hospitalized within the recommended 120 min of AMI onset.5,6 International studies demonstrated a very wide range of prehospital times—from a few minutes to several days.12–19 According to published data, the median prehospital time in the United States was 3.5 h, in the United Kingdom it was 2.5 h, in Japan it was 4.5 h, and in South Korea it was 4.4 h.14–20 The most significant delay in our study occurred from the onset of symptoms till the patients searched for medical help. Other authors have also reported this period, known as “decision-making time,” to be the longest prehospital delay in AMI patients.6,13–15 Possible explanations might be (1) insufficient awareness of the patients about their health state, (2) aware but hesitative patients (or their relatives), (3) atypical/vague symptoms, and (4) comorbidities and/or severely compromised clinical state with “masked” symptoms of AMI.
Less than 40% of our AMI patients called the National EMS and only 15.4% of them used an ambulance for this service: despite calling EMS, many patients preferred to use other transport to hospital. It was probably a subjective decision of the patients and/or their relatives, not clinically justified; according to our analysis, the use of private/public non-medical transport was associated with higher in-hospital mortality and twofold increase in the risk of in-hospital complications. The better outcomes of EMS users in our study compared to other ways of transportation were probably due to (1) higher rate of reperfusion therapy, (2) shorter time from the onset of symptoms till coronary reperfusion, and (3) better prehospital care provided by the EMS teams such as high level of daily clinical experience with AMI patients, usage of established protocols for initial anti-ischemic therapy, and better triage at hospital admission. Other studies also found that the number of AMI patients calling EMS was much less than expected—usually <50%.13–19,21 Instead, many first contacted their family physician and this prolonged the prehospital time.14–18,22 Possible subjective explanations for this finding might be (1) patients did not feel ill enough to call EMS, (2) patients looked for some type of advice/support before calling EMS, and (3) patients trusted the family physician’s initial examination and believed he or she was responsible to notify EMS further if necessary. In our study, FMC with a GP was associated with the longest prehospital delay.
Our results and the results of other authors outline two basic directions for avoidance of prehospital delay. At patient’s level, prehospital delay could be reduced by educational campaigns aiming to increase the awareness of the general populations and particularly of high-risk individuals and their relatives about alarming cardiovascular symptoms as well as the necessary actions that should be taken if such symptoms appear. Interventions that could reduce prehospital delay at the primary care providers’ level include educational outreach visits and training on regular basis, interprofessional learning, audit and feedback, and use of decision support tools.
The limitations of our study are as follows:
The number of patients in our study does not allow our results to be extrapolated to all patients with AMI.
We analyzed the influence of some of the most common but not all possible factors that could exert influence on the prehospital times.
The factors we investigated could have a different impact on prehospital times in other countries due to differences in the structure and functioning of EMS and other prehospital institutions.
In conclusion, the total prehospital delay in our study was unacceptably prolonged, with patient’s decision time as the major contributor. The delay could be substantially shortened by (1) increased awareness of the general population, particularly of individuals at high cardiovascular risk and (2) continuous medical education and regular practical training of the primary care providers about coping with medical emergencies.
Footnotes
Acknowledgements
The authors would like to thank Associated Professor Mircho Vukov from New Bulgarian University, Sofia, Bulgaria, for his kind advices and assistance with the statistical analysis. All the authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the Hong Kong Journal of Emergency Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Our study and the manuscript submitted to HKJEM were not funded by any institutions, organizations, third parties, grants, or other financial sources.
Human rights
Performance of our study and publication of data from it in the current manuscript are not associated with any violation of human rights.
Availability of data and materials
All materials and data related to the current manuscript and the study on which it was based are available and at the disposal of Prof Maria Hristova Milanova and Stefan Naydenov Naydenov.
Informed consent
Written informed consent was obtained from each patient included in the study before enrollment. The signed informed consent forms are available with Prof Maria Hristova Milanova.
Ethical approval
The study was approved by the ethical review board of the local ethics committee (Resolution No. 272/21.01.2008). The study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.