
Abstract
Background:
Point-of-care ultrasound plays an important role in patient management in the prehospital setting. Prehospital ultrasound training for the paramedics has been developed in the West for many years. However, the present training curriculum for the local ambulance personnel does not include point-of-care ultrasound. This study is the first of its kind in Hong Kong on the feasibility of teaching ambulance personnel how to perform focused assessment with sonography in trauma by a 1-day course.
Objective:
It aimed to assess whether the ultrasound-naïve ambulance personnel could acquire the skills and knowledge of point-of-care ultrasound following a tailor-made training programme.
Methods:
This was a prospective observational study. The training programme was a 1-day course consisted of didactic lectures and hands-on practice. Each participant was assessed by a written test and a skills test. Descriptive statistics were used to describe the ambulance personnel and their results of the written and skills test. Significance testing was by Mann–Whitney U test and Spearman correlation test where appropriate.
Results:
Seventeen members of Ambulance Service Institute (Hong Kong Branch) participated in the programme. All of them currently are the ambulance personnel and they joined the programme via the captioned institute. Enrollment was voluntary. The median score in the written test was 20 out of 25. The median time to complete the four views of the focused assessment with sonography in trauma scan was 3.4 min. There was no significant relationship between test performance and educational background and work experience of the ambulance personnel.
Conclusion:
Training the local ambulance personnel point-of-care ultrasound is feasible. Their acquisition of skills and knowledge of point-of-care ultrasound after a 1-day course was satisfactory.
Introduction
Development of portable ultrasound systems began in the 1990s. Thereafter, the ultrasound systems have become more compact in size and lighter in weight so that the application of ultrasound could be expanded to the prehospital setting. 1 Ultrasound is a useful diagnostic adjunct especially in the prehospital environment where physical examination may be difficult or unreliable. 2 Experience from the West has demonstrated that prehospital ultrasound is feasible and can be taught to prehospital personnel, including paramedics with good retention of the ultrasound skills.3,4 Furthermore, studies showed that the practice of point-of-care ultrasound (POCUS) by paramedics in the United States not only resulted in improvement in the diagnostic accuracy but also in streaming patient care, and triaging patients to an appropriate center of care especially for trauma patients.5,6 With the help of focused assessment with sonography in trauma (FAST), unnecessary needle decompression was avoided in 30% of trauma patients suspected to have pneumothorax. 6 In total, 22% of patients were changed to appropriate centre on the basis of POCUS evaluation of patients. 5 The training of the ambulance personnel in Hong Kong is different from the West. The majority of them can be considered equivalent to Emergency Medical Technician-Intermediate level. The clinical challenges they face, nonetheless, may not be very different from other parts of the world. The use of POCUS in the prehospital setting by them should therefore be considered valuable. This study aimed to assess whether the ultrasound-naïve ambulance personnel could acquire the skills and knowledge of POCUS following a tailor-made training programme.
Methods
This was a prospective observational study undertaken as a collaboration between the Emergency Medicine Unit of The University of Hong Kong and the Ambulance Service Institute (Hong Kong Branch). The training programme was a 1-day course (Table 1). The primary objective was to equip an ambulance personnel with the knowledge and skills in performing a FAST with a portable ultrasound device. It consisted of three 30-minute didactic lectures and 200-minute hands-on practice using a digital simulation system and portable ultrasound machines (SonoSim ultrasound education and training product, GE Vscan Extend, and Logiq E portable ultrasound machine) and human models. Pre-course reading materials consisting of the lecture contents were sent to enrollees 1 week in advance. The teaching materials were in English but the medium of instruction in class was in Chinese. The instructors were either specialists in emergency medicine or advanced practice nurses with more than 10 years of experience in POCUS. The ambulance personnel were recruited from the members of the Ambulance Service Institute (Hong Kong Branch). Enrollment was voluntary. The only exclusion criterion was prior training in POCUS. The instructor to ambulance personnel ratio was limited to 1:4.
Content of the 1-day training programme.
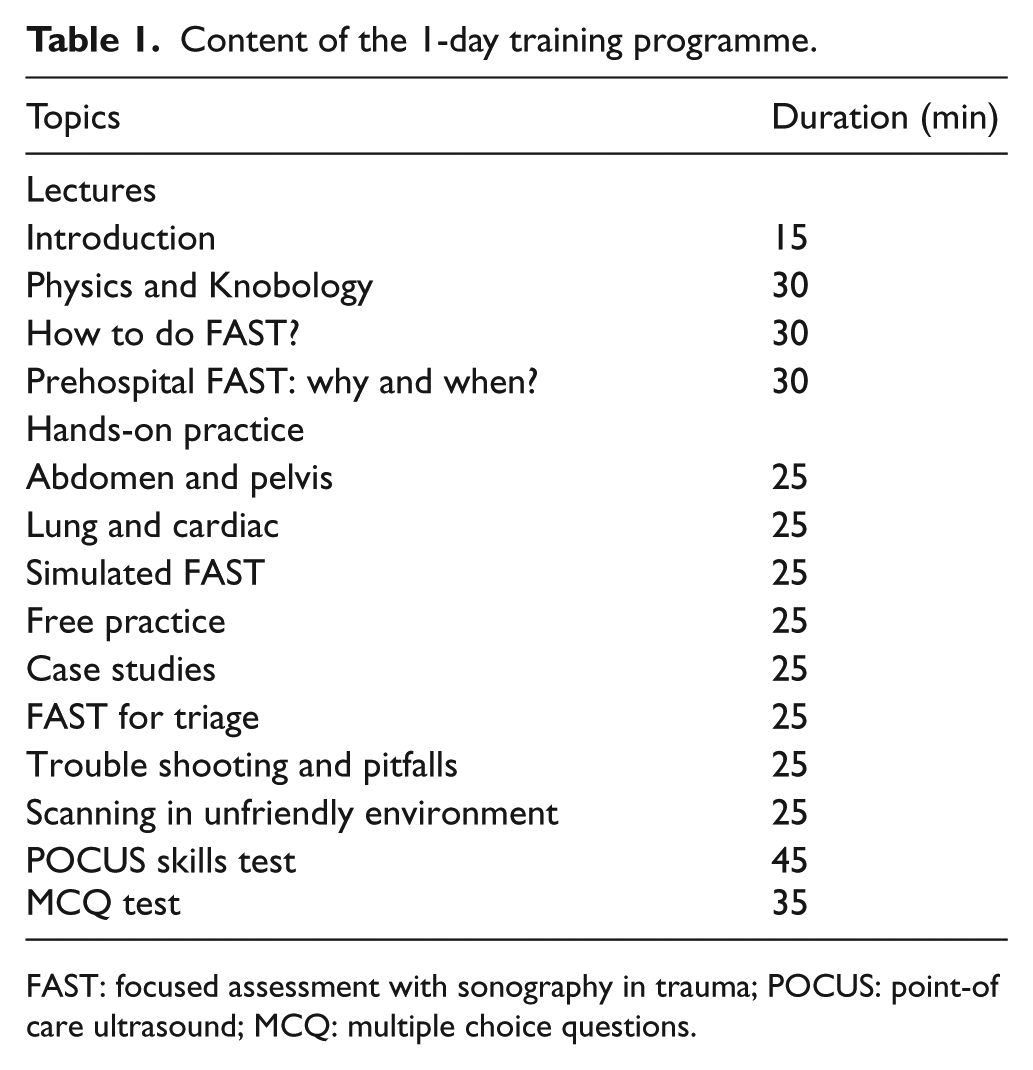
FAST: focused assessment with sonography in trauma; POCUS: point-of care ultrasound; MCQ: multiple choice questions.
At the end of the programme, each participant would be assessed on their ability to demonstrate the hepatorenal recess, splenorenal recess, rectovesical pouch, and the pericardial window on a healthy human model using a GE Vscan Extend device. Therefore, this exercise did not test their ability to identify abnormal findings. The assessment would be timed. Adequacy of the ultrasound images was judged by an instructor. Each participant then went through a written test consisted of 25 multiple choice questions (MCQ) on the knowledge of prehospital application of POCUS following the skills test. There were 5 questions on knobology, 15 on FAST, and 5 on the application of ultrasound for prehospital triage. Each correct answer would score 1 mark. Marks were not deducted for wrong answers.
Descriptive statistics were used to describe the ambulance personnel and their results of the written and skills test. Difference in performance was compared according to the educational level of the ambulance personnel by the Mann–Whitney U test. The relationship between their performance and years of work experience was evaluated by the Spearman correlation test. A P value < 0.05 was considered significant. Data were managed by SPSS 24.0 for Windows (SPSS, Chicago, IL, USA).
Results
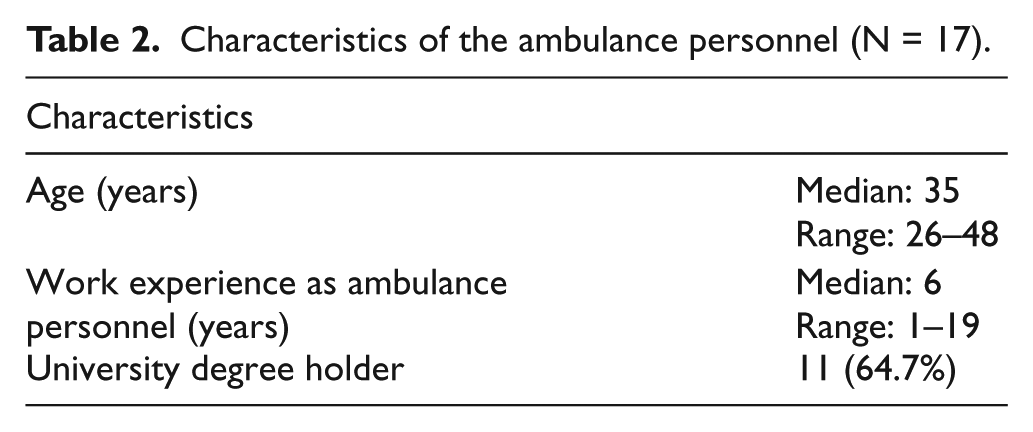
The training programme was conducted on 9 December 2017 from 9 a.m. to 5 p.m. Seventeen ambulance personnel enrolled to the programme. Five instructors (four clinicians and one nurse) were recruited. The median of the work experience of the 17 ambulance personnel was 6 years and 11 held a university degree (Table 2). The median time to obtain an adequate image of the hepatorenal recess, splenorenal recess, rectovesical pouch, and the pericardial window was 3.4 min and 3 out of the 17 students completed the skills test within 2 min. The median score of the MCQ test was 20. Seven got a score above 20 (Table 3). There was no significant difference in performance between students with and without a university degree (Table 4). Years of work experience had an insignificant positive correlation with performance (Table 5).
Characteristics of the ambulance personnel (N = 17).
Results of skills test and written test.
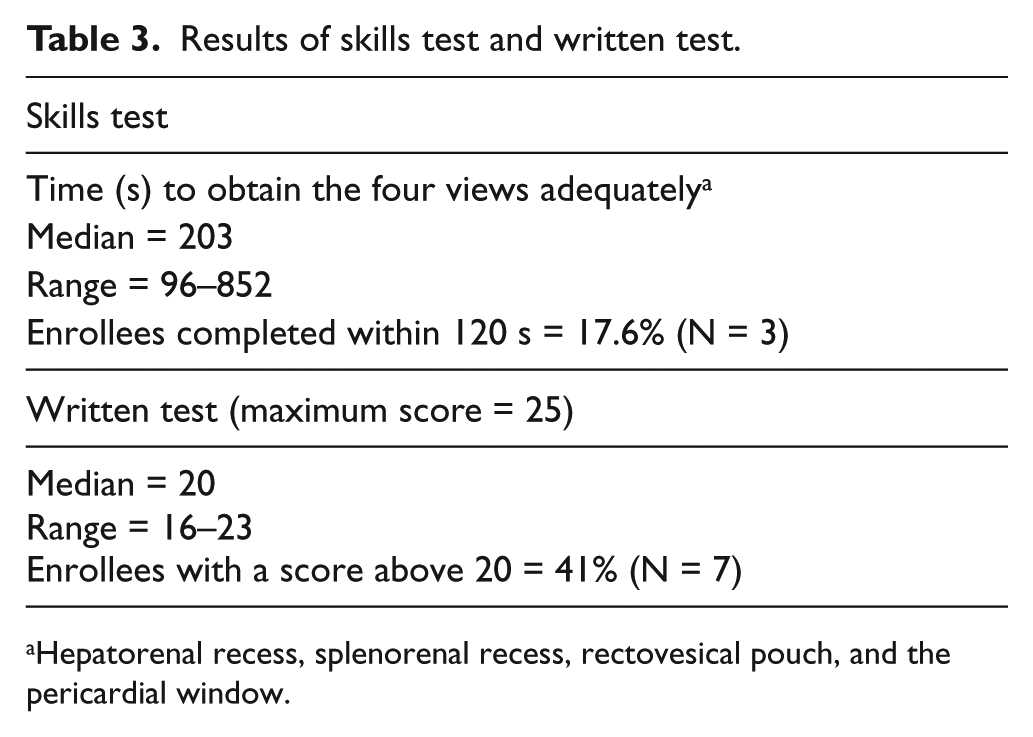
Hepatorenal recess, splenorenal recess, rectovesical pouch, and the pericardial window.
Performance and ambulance personnel’s educational background.
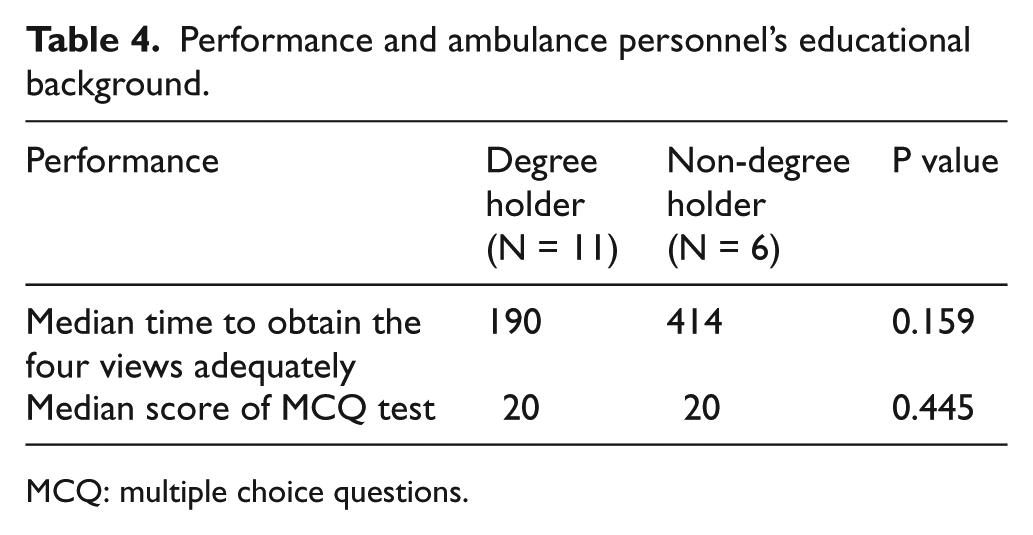
MCQ: multiple choice questions.
Performance and ambulance personnel’s work experience.
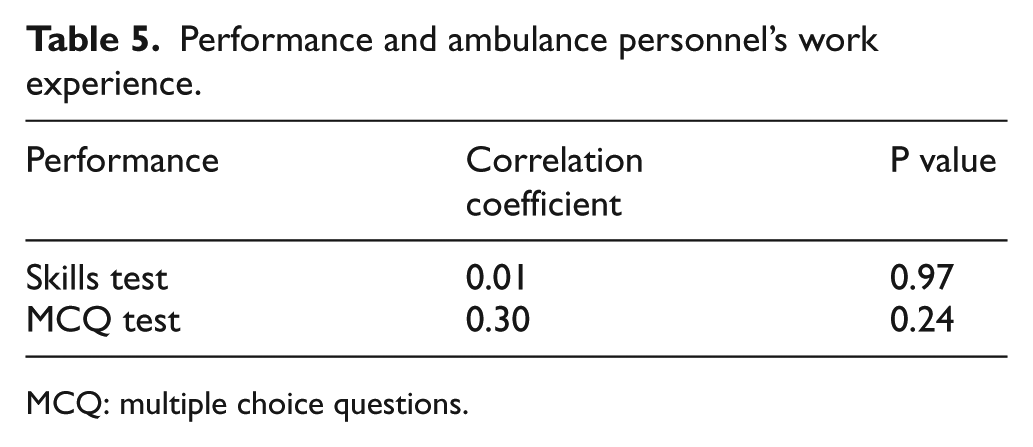
MCQ: multiple choice questions.
Discussion
Most studies on prehospital ultrasound were done in the West and suggested that prehospital personnel could perform focused ultrasound assessment of patients satisfactorily.7,8 Because of the difference in training of prehospital care providers, the results cannot be generalized to Hong Kong. This study is the first local one on the feasibility of teaching ambulance personnel how to perform FAST by a 1-day course. The results from the skills and knowledge assessment suggest that it is feasible to teach Hong Kong’s ambulance personnel POCUS through a concentrated course. While the exact learning curve for focused ultrasound is unknown, a study reported good performance in a field trial of ultrasound by ultrasound-naïve paramedics after 8 contact hours of training. 8 It is evident that the ambulance personnel in this study could acquire the POCUS knowledge effectively as the median score in the MCQ test was 20 out of 25. This may be because ample time for self-study (1 week) was given to them before the commencement of the course. The purpose of sending them the lecture materials beforehand was to allow more time to hands-on practice during the 1-day training. As for the skills in performing the FAST assessment, the time for completion ranged from 1.6 to 14.2 min. Only three participants could complete within 2 min. A systematic review reported that the time required for a FAST examination varied between 1 and 10 min. 9 Thus, there should be room for improvement for the local ambulance personnel. While it is important to complete a FAST examination as soon as possible, accuracy is not to be ignored. To improve, incorporation of ultrasound physics and anatomy into the present curriculum of the emergency medical service (EMS) may help. Furthermore, the training programme needs to be more skill oriented with more time allocated to practice. Refresher courses are also desirable.
The study reveals a lack of significant relationship between test performance and educational background and work experience. This finding suggests that ultrasound training can be implemented as an in-service programme and started now. The latter is especially important if the local EMS is to take the portable ultrasound systems to the roadside.
Limitations
This study is limited by its small sample. When more courses are organized, a bigger sample of ambulance personnel with more varied background could give a clearer answer to the feasibility of teaching POCUS to them. In this course, pathologies were only shown as simulated images on computers. It is unknown if the ambulance personnel can detect real pathologies. Further studies should include assessment by proctored examination in real patients.
Footnotes
Acknowledgements
This report cannot be completed without the effort from our instructors. The authors sincerely thank Drs Dora Lee, Ralph Cheung, Tony Chan, Stanley Chau, and Jacky Chan for being the instructors in the programme. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
We confirm that the manuscript has been submitted solely to this journal and is not published, in press, or submitted elsewhere. And we confirm that we have checked the manuscript submission guidelines and complied with any specific policy requirements specified. We also have prepared (a) a complete text minus the title page, acknowledgements, and any running headers of author names, to allow blinded review and (b) a separate title page with author information.
Informed consent
Written informed consent was obtained from the subjects for their anonymized information to be published in this article.
Ethical approval
We confirm that Ethical Committee approval was sought where necessary and is acknowledged within the text of the submitted manuscript.
Human rights
We further confirm that any aspect of the work covered in this article that has involved either experimental animals or human patients has been conducted with the ethical approval of all relevant bodies, and that such approvals are acknowledged within the manuscript.